


INTRODUCTION
Clostridioides difficile infection (CDI) is common worldwide and is the most common healthcare-associated infection in North America. Although the estimated national burden of CDI decreased from 476,400 cases in 2011 to 462,100 cases in 2017, CDI is a leading nosocomial infection in the United States [1]. In addition, C. difficile is the most common pathogen (32.2%) detected in cases of acute infectious gastroenteritis among adults treated in United States hospital-based outpatient settings [2]. Few studies have investigated the epidemiology of CDI in Asian countries because of a lack of awareness by physicians and non-optimum diagnostic methods in some places [3]. A recent Korean study using national data from the Health Insurance Review and Assessment Service showed that the incidence of CDI gradually increased from 0.3 per 1,000 admissions in 2008 to 1.6 per 1,000 admissions in 2020, suggesting that the incidence is approaching that in Western countries [4]. Another study using nationwide claims data showed that the length of hospital stay and medical costs were 3.3-fold and 5.0-fold greater, respectively, in patients with CDI than in hospitalized patients with gastroenteritis and colitis as controls [5].
Commercial stool tests for CDI diagnosis include enzyme immunoassay (EIA), glutamate dehydrogenase (GDH) test, nucleic acid amplification test (NAAT), C. difficile culture, and cell cytotoxicity neutralization assay [6]. However, there is currently no single rapid test for the diagnosis of CDI that has been approved by the Food and Drug Administration. Recent guidelines from Western countries recommend multistep diagnostic algorithms for CDI [7,8]. However, the optimum diagnostic strategy for CDI is controversial. NAAT has high sensitivity for detecting C. difficile toxin genes but may indicate simple colonization rather than active infection, resulting in the overdiagnosis of CDI. Toxin EIA has higher specificity but lower sensitivity for diagnosis of CDI in patients with symptoms. In addition, the presence of toxin does not always indicate true CDI in patients with simple colonization or those who have been successfully treated [9]. Because of its high rapidity and accuracy, NAAT-based diagnosis is being increasingly used in South Korea [10]. Although several studies showed that patients with CDI who had positive NAAT but negative toxin EIA developed fewer CDI-associated complications and had lower mortality than patients with both positive examinations, clinical outcomes remain controversial [11]. Few studies to date have focused on the clinical characteristics of patients with CDI in the Asia-Pacific region who test positive only on the NAAT.
The aim of this study was to evaluate the clinical characteristics and predictive factors of patients with CDI who have a positive NAAT but negative toxin EIA.
METHODS
Study design
This retrospective cohort study was performed from January 2015 to December 2015 at Seoul St. Mary’s Hospital, a tertiary teaching hospital in South Korea. Stools from patients aged ≥ 18 years with clinically significant diarrhea were subjected to NAAT, EIA, and toxigenic culture for the diagnosis of CDI. Patients diagnosed with CDI based on positive results of toxigenic culture were enrolled. Patients with a negative NAAT were excluded from the analysis.
Laboratory assays for CDI
Laboratory assays were carried out in accordance with the manufacturers’ instructions. For NAAT, the Xpert C. difficile assay was performed on the GeneXpert® system (Cepheid, Sunnyvale, CA, USA); it detects the gene encoding toxin B (tcdB). Stool samples were swabbed using a transport swab (Copan Diagnostics, Murrieta, CA, USA). The swab contents were suspended in elution buffer before being pipetted into the chamber of the Xpert test cartridge. The cartridge was inserted into the Xpert instrument. The results are given as positive or negative for toxigenic C. difficile. For EIA, we used RIDASCREEN C. difficile Toxin A/B EIA (R-Bipharm AG, Darmstadt, Germany) in accordance with the manufacturer’s instructions. Stool samples (100 μL) were added to 1 mL RIDASCREEN sample dilution buffer in test tubes and vortex-mixed; the supernatants were collected after centrifugation at 2,500 g for 5 minutes. For toxigenic culture, the stool specimens (1 mL) were mixed with 1 mL thioglycolate broth and vortex-mixed for 5 minutes in an 80°C water bath. The suspension was inoculated onto chromID C. difficile agar (bioMérieux, Marcy-l’Étoile, France), a selective medium that promotes C. difficile growth while suppressing that of other Gram-positive and Gram-negative bacteria and fungi. The plates were incubated at 35°C in a Bactron anaerobic thermoregulatory chamber (Sheldon Manufacturing, Cornelius, OR, USA) and interpreted after 24 and 48 hours.
Definitions
CDI was defined as the presence of symptoms (typically diarrhea) and a positive toxigenic culture for C. difficile, with toxigenicity confirmed by either a positive EIA or NAAT. Patients with negative NAAT results were excluded from the study to facilitate investigation of the clinical significance of EIA positivity. The severity of CDI was classified according to the criteria proposed by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America (IDSA/SHEA), which are based on leukocyte counts and renal definitions [8]. At presentation, leukocytosis with a white blood cell (WBC) count of ≥ 15,000/mL or a serum creatinine level of ≥ 1.5 mg/dL was defined as severe CDI. Fulminant or severe complicated CDI was characterized by the presence of hypotension, shock, ileus or toxic megacolon [7]. An immunocompromised state was defined as one of the following: neutropenia (< 1,000 WBCs/mm3); hematologic malignancy; previous allogenic hematopoietic stem cell or solid organ transplantation; inherited severe immunodeficiency (such as chronic granulomatous disease or severe combined immunodeficiency); prolonged use of corticosteroids at a mean minimum dose of 0.5 mg/kg/day of prednisone equivalent for at least 4 weeks within the last 3 months; or treatment during the past 90 days with chemotherapy, T-cell immunosuppressants (such as azathioprine or cyclosporine), tumor necrosis factor-α inhibitors, or specific monoclonal antibodies. High-dose corticosteroids were reported separately if a patient had received one or more doses of prednisone equivalent to 1 mg/kg body weight in the 7 days prior to diagnosis of CDI. Chemotherapy was defined as use of any agent directed against cancer such as alkylating agents or antimetabolites in the 3 months prior to the diagnosis of CDI. Gastrointestinal manipulation included insertion of nasogastric tube or any type of gastrointestinal endoscopy in the previous 7 days.
Clinical data collection
We collected clinical data on demographics, comorbidities, previous hospitalization and surgery, immune system impairment, and hospitalization duration. Data regarding prior use of antibiotics were collected up to 30 days before CDI diagnosis. The clinical variables evaluated were vital signs, complete blood counts, biochemical parameters including serum levels of albumin and creatinine, liver function test results, and the results of endoscopy, if performed; we also noted if antimicrobial treatment was given for CDI. These data were collected from electronic medical records. Patients were followed for 60 days after CDI diagnosis. A response to the initial treatment was defined as having fewer than three unformed stools in 24 hours within 10 days. We defined clinical cure as response to CDI treatment as determined by the clinician. Sustained clinical cure was defined as no recurrence within 4 weeks after successful CDI treatment. Recurrence was defined as a re-emergence of diarrheal symptoms and need for retreatment for a new CDI diagnosis within 60 days after CDI diagnosis. Survival status was monitored at 60 days after CDI diagnosis. If patients were discharged from the hospital before the end of follow-up, they or their relatives were contacted by telephone or at outpatient clinics to ascertain symptoms and vital status at 8 weeks (at home, hospitalized, or dead).
Statistical analysis
Statistical analyses were carried out using the SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Categorical variables were compared using the chi-square test or Fisher’s exact test, and continuous variables were assessed using Student’s t-test or the Mann–Whitney U test. Logistic regression models were used for multivariable analysis to identify risk factors associated with treatment outcome and mortality; variables with a value of p < 0.1 on univariable analyses were included. A p value of < 0.05 was considered indicative of significance.
RESULTS
Clinical characteristics
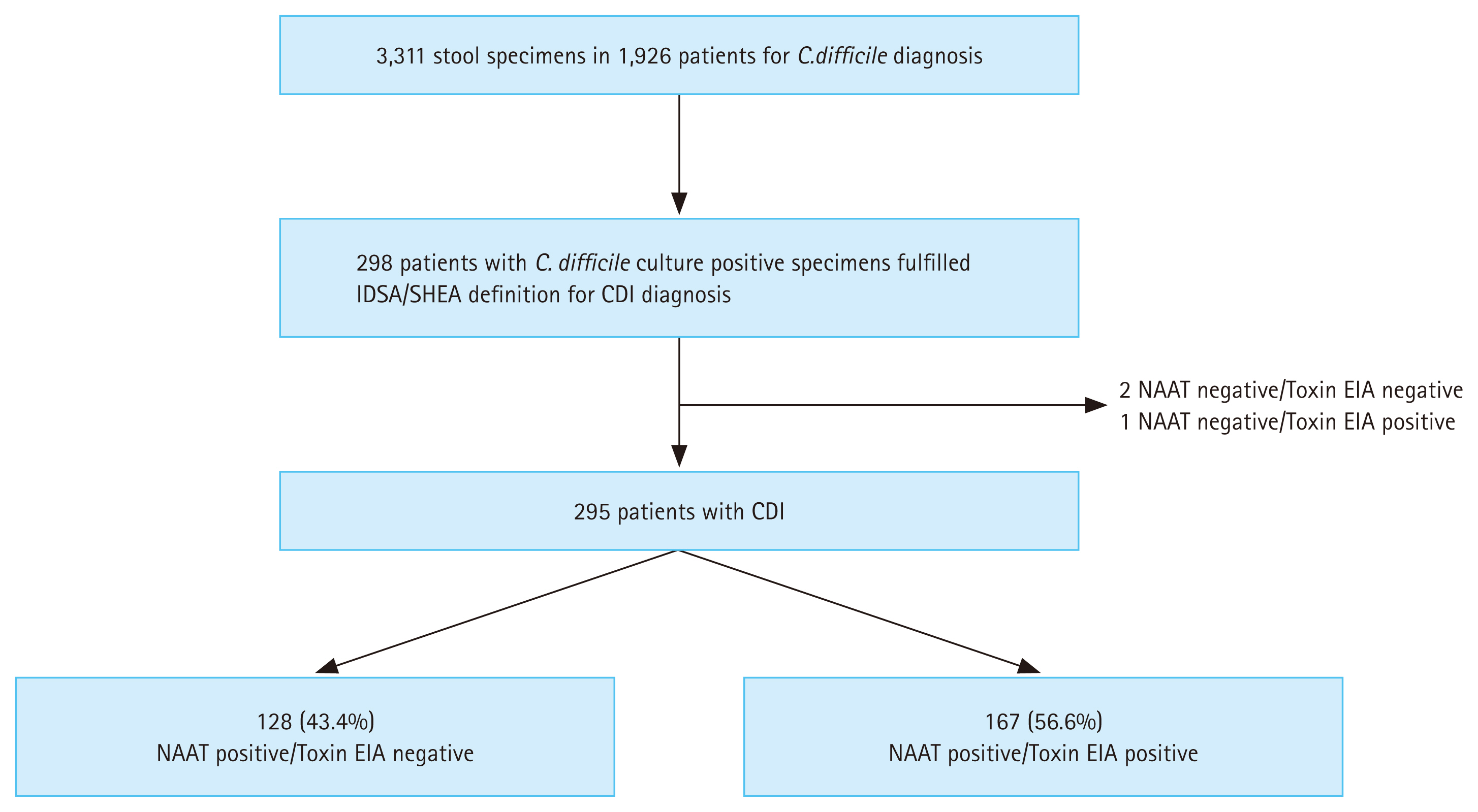
In total, 3,311 consecutive stool samples were subjected to C. difficile culture, NAAT, and toxin EIA (referred to as “Toxin” throughout results) simultaneously to identify the cause of clinically significant diarrhea from January 2015 to December 2015. Among them, 298 culture-positive patients who fulfilled the criteria for CDI, and 3 NAAT-/Toxin− patients were excluded. Factors influencing NAAT+/Toxin− results were evaluated in 295 patients (Fig. 1). Among them, 128 (43.4%) were NAAT+/Toxin− and 167 (56.6%) were NAAT+/Toxin+. Table 1 shows the clinical characteristics of each group. There were no significant differences between the two groups in ≥ 38°C fever at CDI onset, WBC count of < 1,000/mm3, eosinophil count, or the levels of C-reactive protein, creatinine, or albumin. Patients with a history of antibiotic treatment for more than 3 days during the previous 30 days were more likely to test positive than negative on the EIA. Patients who tested negative on the EIA were more likely to receive high-dose corticosteroid (prednisolone ≥ 1 mg/kg body weight). In addition, 181 patients had hematologic (n = 101), solid (n = 78), or both hematologic and solid (n = 3) malignancies. There were no associations between the types of malignancies and the EIA results.
Clinical outcomes
Table 2 summarizes the clinical outcomes in patients with CDI who tested positive on the EIA. In contrast to NAAT+/Toxin+ patients, NAAT+/Toxin− patients were more likely to have less severe disease and to have had no therapy. In these patients, symptoms often improved prior to initiation of treatment. The clinical outcomes were similar between the two groups. Among patients who underwent endoscopy, pseudomembranous colitis was diagnosed in 12 NAAT+/Toxin− patients (48.0%) and 17 NAAT+/Toxin+ patients (39.5%). The rates of clinical cure were 97.5% and 96.3%, the corresponding recurrence rates were 3.4% and 4.5%, the crude in-hospital mortality was 12 (9.4%) and 23 (14.0%), and in-hospital mortality attributed to CDI was 0 (0.0%) and 2 (1.2%) in the two groups, respectively. Previous use of antibiotics, severity, high-dose corticosteroid treatment, and treatment modality (no therapy, metronidazole, or metronidazole plus vancomycin) were significant in univariable analyses. Multivariable logistic regression analysis showed that previous use of antibiotics was inversely associated with negative EIA results (odds ratio 0.276), whereas high-dose corticosteroid was positively associated (odds ratio, 2.533); both associations were statistically significant (Table 3).
DISCUSSION
The present study demonstrated that a substantial proportion (43.4%) of patients tested negative for CDI in the EIA but were diagnosed with it and treated for it. A negative EIA result was inversely associated with prior antibiotic use but positively associated with prior high-dose corticosteroid use. However, the difference in severity of CDI between NAAT+/Toxin+ and NAAT+/Toxin− patients was not statistically significant. In addition, there were no differences in recurrence, in-hospital mortality, or CDI-related mortality between the two groups. Taken together, these findings suggest that patients with CDI who have a negative toxin EIA are at risk of complications, recurrence, and poor clinical outcomes, possibly necessitating treatment. This is consistent with a large multicenter study in the United States that did not identify an association between toxin EIA results and severe clinical outcomes with the exception of a higher recurrence rate in patients with toxin-positive CDI. In that study, toxin positivity was significantly associated with previous antibiotic exposure as well as inpatient care and long-term care facility admission [12]. However, the CDI recurrence rate was similar in both groups of our study. This finding might be attributable in part to less severe outcomes due to lower prevalence of hypervirulent strains in Asia-Pacific countries, explained by the fact that toxin-positive infections were associated with a greater likelihood of recurrence of more highly virulent strains. A large multinational survey study in 13 Asia-Pacific countries showed that C. difficile ribotypes 017 (the most common toxin A−/toxin B+ strain, 16.7%), 014/020 (11.1%), and 018 (9.9%) were prevalent, although with wide variation between countries. The molecular epidemiological characteristics may contribute to the relatively mild clinical course of CDI in Asia, which could be related to the predominance of the ribotype 017 strain that exclusively produces tcdB in this region [3]. Less than 10% of CDIs are caused by hypervirulent strains in South Korea [13]. In addition, a Korean multicenter study on the incidence and clinical characteristics of CDI in 1,367 patients showed that the CDI recurrence rate was 8.9%, complicated CDI was identified in only 3.6% of patients, and the CDI-related mortality rate was 0.51%, suggesting that the clinical features of CDI in Korea are milder than in Western countries [14].
The optimum diagnostic method for CDI is controversial. No diagnostic test can differentiate simple colonization from symptomatic infections, and CDI diagnosis depends on a combination of clinical suspicion and laboratory testing. The primary test is transitioning from EIA to NAAT in several United States hospitals. However, NAATs detect toxin genes, not active toxin, which is essential for CDI development [15]. The clinical significance of C. difficile toxin genes without toxin production by NAAT is unclear and complicated, particularly in inpatient healthcare facilities where C. difficile colonization is more common [16,17].
The guidelines of the American College of Gastroenterology (ACG) state that CDI diagnostic algorithms should include a highly sensitive and specific testing method to help discriminate colonization from active infection only in patients with symptoms suggesting active CDI [15]. The ACG and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines (updated in 2016) recommend a two-step diagnostic testing algorithm for CDI, in which stool is first tested using a highly sensitive NAAT or GDH assay, followed by EIA [7,15]. However, there is no consensus for CDI diagnosis in the Asia-Pacific region. A first South Korean survey of 57 hospitals and 9 laboratories reported that EIA, NAAT, and toxigenic culture, alone or in combination with other assays, were performed in 51 (89.5%), 37 (64.9%), and 37 (64.9%) of these institutions; none were available in 9 [18]. More than 80% of the participating institutions performed NAAT and/or culture with or without a toxin assay. These findings suggest that concerns about CDI are increasing and that highly sensitive diagnostic methods with short turnaround times are needed. The GDH assay is rarely used, having been introduced less than 10 years ago and approved for reimbursement in South Korea only since 2016 [18]. In a South Korean nationwide survey of 150 institutions, 65 used a combination of 2 or more tests. EIA (84.3%) was the most commonly used, followed by NAAT (58.4%) and GDH (25.8%) [6]. In a Japanese prospective multicenter study of 650 stool samples from 566 patients, compared with toxigenic culture as the gold standard, the sensitivities of EIA, GDH, and NAAT were 41%, 74%, and 73%, and their specificities 96%, 98%, and 87%, respectively [19]. The sensitivity and specificity of the two-step algorithm (GDH plus EIA, arbitrated by NAAT) were 71% and 96%, respectively. In a study in Thailand, the sensitivity of NAAT using the BD MAX Cdiff assay to detect tcdB was low (69%) compared with toxigenic culture as the reference standard [20]. These results suggest that the sensitivity of NAAT is lower in such countries than in Western countries and that NAAT and/or GDH might be inappropriate as the first test of a two-step algorithm or as a standard test in Asian countries [19]. However, in South Korea, Song et al. [10] evaluated the accuracy of three diagnostic methods (real-time polymerase chain reaction [PCR] of toxin genes, C. difficile toxin assay, and culture for C. difficile) in 117 cases of CDI in 90 patients. The sensitivity of real-time PCR (87%) was significantly higher than that of the C. difficile toxin assay (49%) and culture for C. difficile (65%). A considerable proportion of patients (29%) were diagnosed only by real-time PCR. Shin et al. [21] reported that the sensitivity and specificity of Xpert compared with toxigenic culture were 90% and 93%, respectively.
ESCMID guidelines suggest that NAAT+/Toxin− results may represent true infection or colonization and so require further evaluation [7]. Because toxin levels in stool could be associated with the severity of diarrhea, patients with CDI who have a negative EIA may have low toxin levels, resulting in less shedding of spores and less severe diarrhea [11]. Although the exact mechanism of false-negative EIA results is unclear, possible causes include interstrain variability and dilution to below the limit of detection secondary to an increased volume and frequency of stool in some patients [22]. In addition, ultrasensitive quantitative toxin EIA cannot accurately distinguish asymptomatic C. difficile colonization from symptomatic infection because colonized individuals without symptoms may also have a positive toxin EIA [23]. In one study, although severe CDI according to the criteria of the IDSA/SHEA guidelines was more common in patients with CDI who had a positive toxin EIA, more than one-quarter of patients with a negative toxin EIA met the criteria for severe CDI. This suggests that a negative toxin result does not necessarily reflect the disease severity [24]. Patients positive on both the NAAT and toxin assay have more severe CDI, a longer duration of symptoms and hospitalization, and increased mortality compared with patients positive only on the NAAT [12,16,25,26]. However, patients with CDI who are positive on only the NAAT have a similar rate of development to severe disease and CDI-related complications than do patients positive on both the NAAT and toxin assay [27–29]. There is clinical uncertainty and lack of evidence about how to manage these patients. In a systematic review and meta-analysis of 26 observational studies (12,737 patients), the 30-day all-cause mortality rate was similar between NAAT+/Toxin+ and NAAT+/Toxin− patients. In addition, treated NAAT+/Toxin− patients had a significantly lower all-cause mortality than untreated patients, suggesting that some NAAT+/Toxin− patients may benefit from treatment [11].
Although CDI is more common in patients with cancer and immunocompromised status, such as those undergoing hematopoietic stem cell transplantation, CDI diagnosis in these patients is difficult [30]. A recent study showed that 274 (57%) of 480 immunocompromised patients with CDI were diagnosed using toxin EIA. In addition, independent predictors of negative toxin EIA included high-dose corticosteroids and leukopenia, suggesting that CDI diagnosis in immunocompromised patients necessitates more sensitive tests such as toxigenic culture or NAAT [29].
Few studies to date have compared the clinical features, relevant exposures, and outcomes of NAAT+/Toxin+ and NAAT+/Toxin− patients with CDI in the Asian-Pacific region, including South Korea. Two Korean studies investigated toxin positivity, but neither compared the clinical outcomes of NAAT+/Toxin+ and NAAT+/Toxin− patients with CDI [31,32]. A recent Korean single-center retrospective study revealed that 83 (43%) patients had a negative toxin EIA among 190 PCR-positive patients using C. difficile cultivated stool specimens. Similar to our results, NAAT+/Toxin− patients with CDI had milder laboratory findings and good prognosis even without treatment. However, there were no differences in clinical outcomes, including mortality and recurrence within 60 days, between NAAT+/Toxin+ and NAAT+/Toxin− patients, similar to our findings. In that study, longer hospital stays and recent high-risk antibiotic exposure were significant factors associated with toxin positivity [33]. Our evaluation was also limited to patients with CDI who had a positive C. difficile toxigenic culture to exclude individuals with simple colonization and allow for analysis of a larger number of samples than in previous studies. Although our study also showed that high-risk antibiotic exposure was a factor associated with toxin positivity, an additional finding was that high-dose corticosteroid treatment before CDI diagnosis was a factor associated with toxin negativity.
The present study has several limitations. First, it was a single-center study with a retrospective design, so not all applicable data were available for collection. Classification of disease severity and previous antimicrobial use was evaluated by reviewing electronic medical records. Second, the effect of CDI treatment on clinical outcomes was incompletely evaluated because the modality, dose, and duration of treatment were variable. Third, we were unable to consider the strain of C. difficile. As previously mentioned, lower rates of CDI caused by hypervirulent strains in South Korea could have biased the outcomes. Fourth, potential risk factors might have been overlooked in the statistical analysis because of the relatively small sample size. Finally, our institution being a tertiary referral center, the cohort included patients with complications and comorbid conditions, and a large proportion were immunocompromised. The resulting referral bias may limit the generalizability of the results. Despite these limitations, our results emphasize the need for individual clinical evaluation and appropriate treatment because CDI-related outcomes were not different between toxin-positive and -negative patients with CDI in South Korea. To confirm these findings, a well-designed prospective multicenter cohort study in the Asia-Pacific region is required.
KEY MESSAGE
1. Clinical outcomes related to CDI are not different between NAAT+/Toxin+ and NAAT+/Toxin− patients, emphasizing the need for individual clinical evaluation.
2. A negative result on the EIA was associated with high-dose corticosteroid use, whereas such a result was inversely associated with previous antibiotic use.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





