


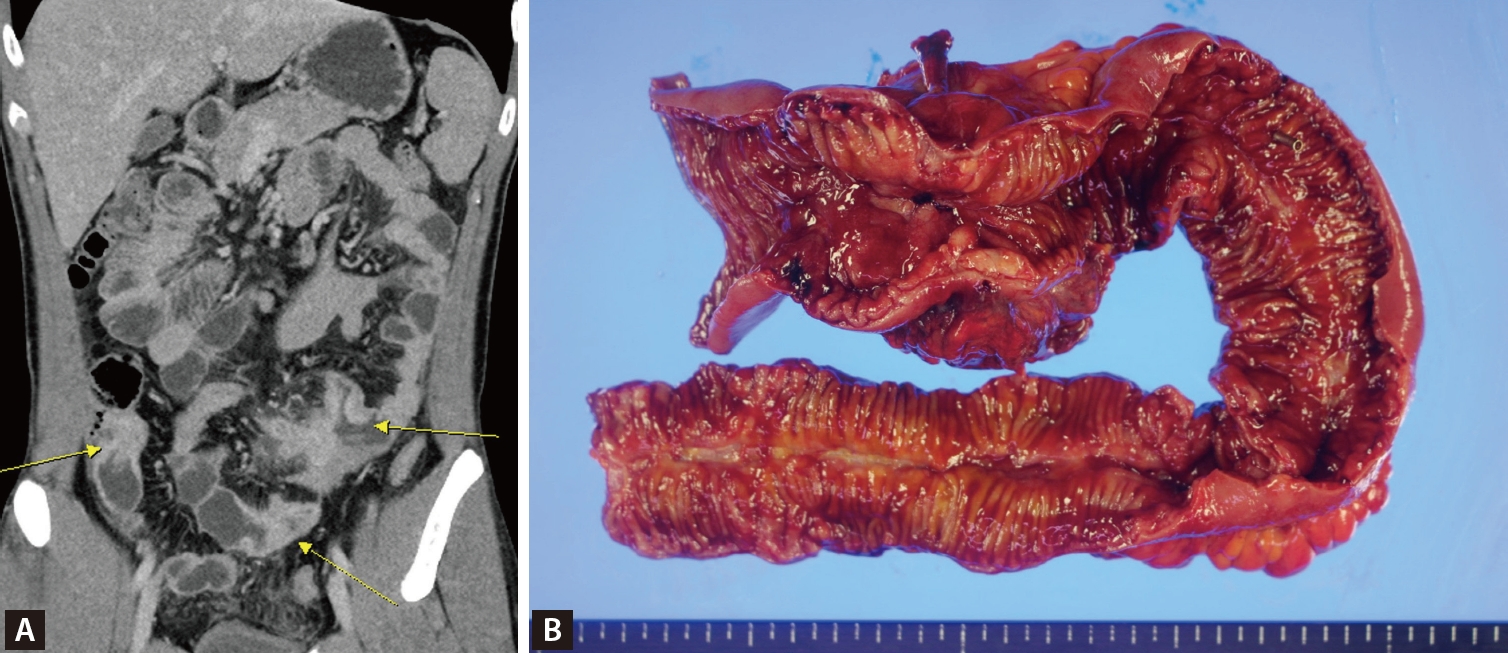
A 30-year-old man was diagnosed with ankylosing spondylitis five years ago and was treated with non-steroidal anti-inflammatory drugs and sulfasalazine. Three years later, the patient underwent small bowel resection due to chronic abdominal pain and was diagnosed with ileal Crohn’s disease with multifocal strictures, microperforation, and an abscess (Fig. 1). After the surgery, the patient was treated with azathioprine, followed by methotrexate. Approximately nine months ago, the patient’s back pain worsened, leading to the introduction of adalimumab. The patient had no history of tuberculosis, a negative interferon-gamma release assay (IGRA) test result, and unremarkable chest radiography result. During follow-up, the patient remained clinically stable on combination maintenance therapy.
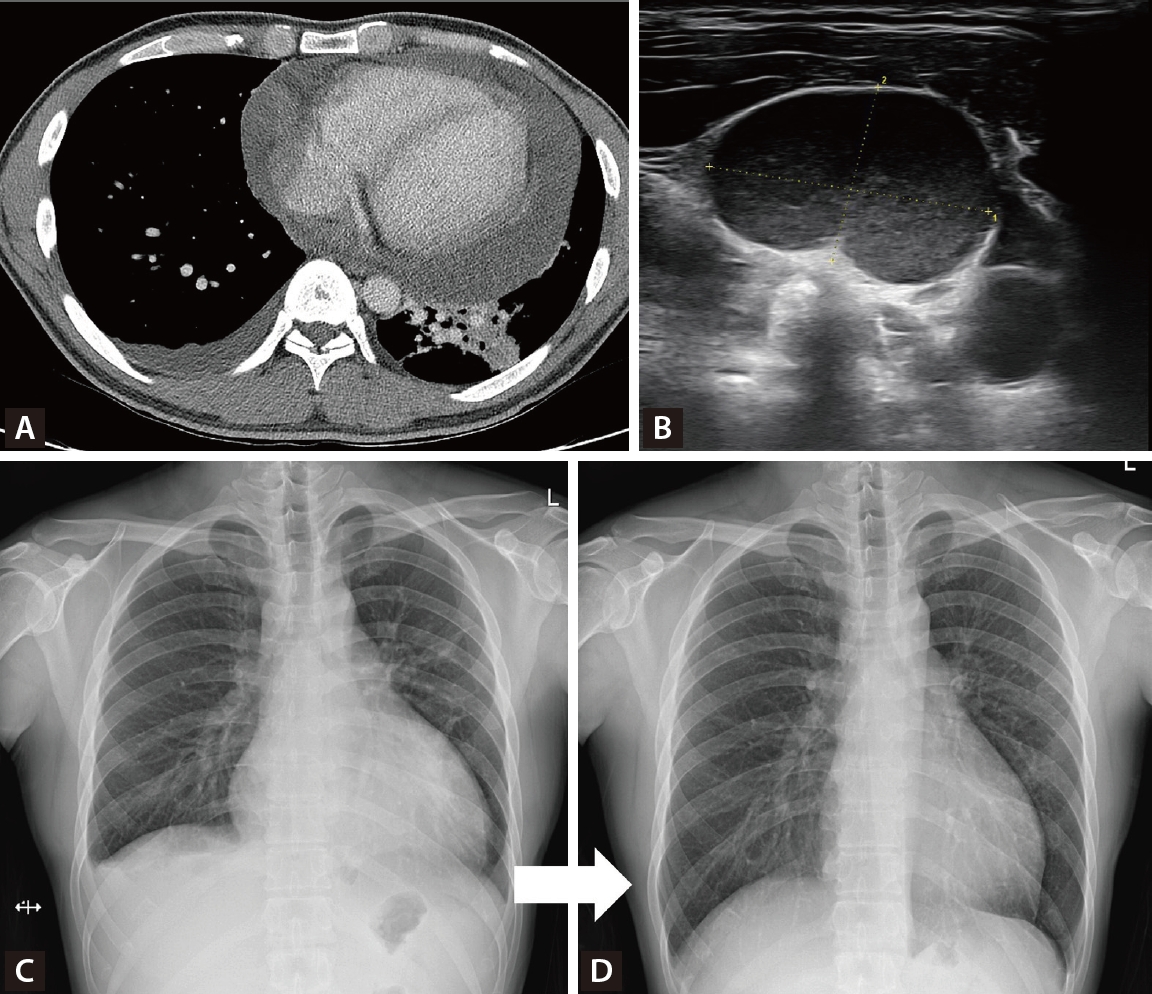
However, the patient developed persistent cough, dyspnea, and shortness of breath over one month, showing no improvement with conventional management, along with several palpable cervical lymph nodes. Chest computed tomography revealed a large pericardial effusion with impending tamponade physiology and diffuse parenchymal infiltration in the left lung field (Fig. 2A). Ultrasound-guided biopsy of the cervical lymph nodes revealed granulomatous inflammation with necrosis (Fig. 2B). Pericardiocentesis drainage was performed, showing positive AFB with M. tuberculosis culture, and adenosine deaminase (ADA) 11.3 IU/L, which was compatible with tuberculous pericarditis, and IGRA result were positive. Standard anti-tuberculosis medication (HREZ) was initiated for six months with rapid symptom improvement (Fig. 2C, D).
Pericarditis is an important extra-pulmonary presentation of tuberculosis. Its late diagnosis may result in serious complications, such as constrictive pericarditis, cardiac tamponade, and increased mortality rate [1]. Tuberculous pericarditis can be diagnosed by examining the pericardial exudate or by detecting a good response after anti-tuberculous drug use in patients with pericarditis [2]. High ADA levels have also been associated with tuberculous pericarditis [3]. Early suspicion and prompt management in patients with immunosuppressive treatment are crucial for improving treatment outcome of tuberculous pericarditis [4,5].
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





