


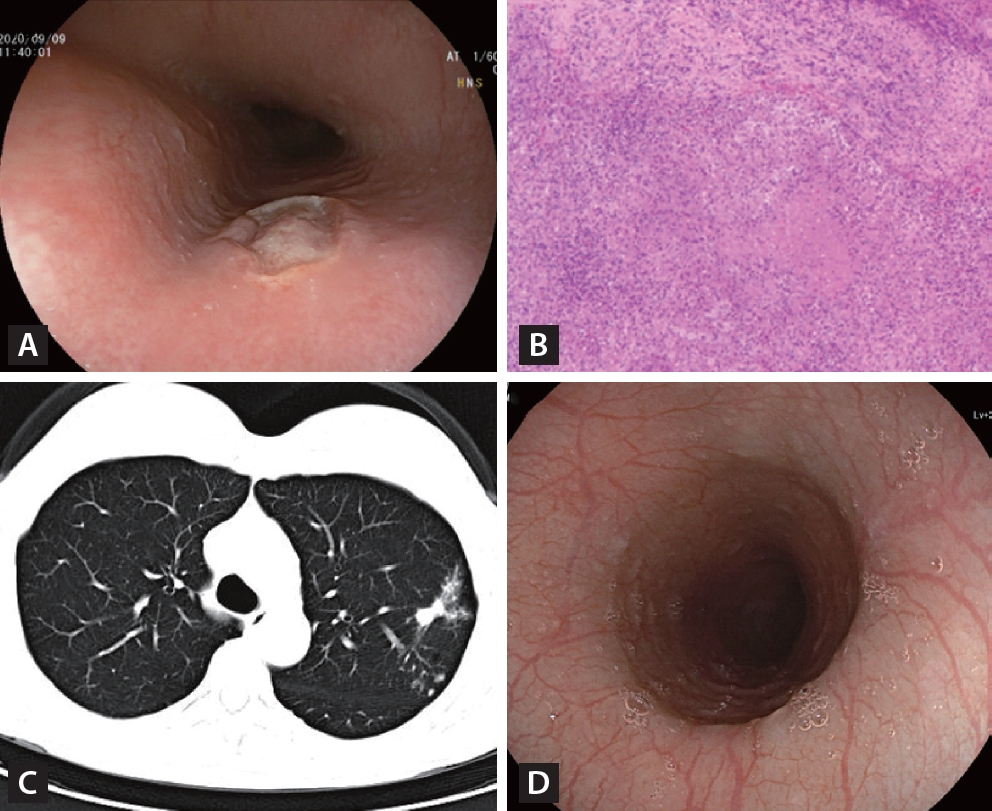
A 46-year-old woman presented with a 3-week history of mild odynophagia and retrosternal pain. She denied fever, cough, weight loss, and history of esophageal carcinoma. She had no recorded medical history. Physical examination was unremarkable with no lymphadenopathy. Laboratory tests were normal. Esophagogastroduodenoscopy showed circumferential circular and deep ulcers with heaped up edges in the upper esophageal region at 28 cm from the incisor (Fig. 1A). Colonoscopy examination was normal. Esophageal biopsy specimens (H&E staining) showed ulceration and caseating granulomas (Fig. 1B). The histopathological characteristics of the esophageal biopsies indicated the possibility of esophageal tuberculosis. Chest computed tomography scan revealed potential pulmonary tuberculosis (Fig. 1C). No enlarged mediastinal lymph nodes were found in adjacent areas. She underwent a bronchoscopy examination. Acid-fast staining and polymerase chain reaction testing of bronchoalveolar lavage fluid for M tuberculosis were positive. The purified protein derivative skin test and T-SPOT. TB assay were also positive. Human immunodeficiency virus screening antibody was negative. Finally, she received a diagnose of esophageal tuberculosis secondary to pulmonary tuberculosis. Esophageal tuberculosis is rare, which is commonly secondary to tuberculosis of lung and lymph nodes [1]. Symptoms are related to the extent of infection, which may include retrosternal pain, dysphagia, haematemesis, and odynophagia [2,3]. The endoscopic features of esophageal tuberculosis is not well defined because of its rarity. Multiple biopsies are suggested to take to detect the evidence of tuberculosis infection. The patient received a standard oral antituberculous regimen with rifampicin, isoniazid, ethambutol, and pyrazinamide per day. Two months after antituberculous treatment, her symptoms of odynophagia and retrosternal pain disappeared. Repeat endoscopy examination showed that the ulcer healed gradually after 12 months of antituberculosis medication (Fig. 1D).
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |