


INTRODUCTION
Acute myocardial infarction (AMI) has been considered as a critical illness related to high mortality and morbidity worldwide. In AMI, timely treatment is important for improving clinical outcomes, but pre-hospital delay may hinder such improvements [1].
Diabetes mellitus (DM) is one of the major risk factors for atherosclerotic cardiovascular disorders [2,3]. Patients with DM often present with atypical clinical symptoms [4] and have treatment delays when they experience AMI [5]. That is, since patients with DM tend to be at high risk of asymptomatic AMI [6], it is important to identify possible clinical symptoms of AMI and reduce the treatment delay.
Therefore, we aimed to evaluate the association between time to presentation and outcomes among patients with diabetes and AMI through a nationwide observational study, with a particular focus on evaluating their relationship with three-year all-cause mortality.
METHODS
Data source
The present study is a post-hoc analysis of the subgroup of patients with DM from the Korea Acute Myocardial Infarction Registry-National Institutes of Health (KAMIR-NIH) registry, which was implemented between November 1, 2011 and December 31, 2015. KAMIR-NIH was a nationwide, multicenter, web-based prospective observational cohort; 20 tertiary high-volume centers performing percutaneous coronary intervention (PCI) in patients with AMI participated in this cohort [7]. The protocol for the KAMIR-NIH registry was adequately ratified by the steering committee of the institutional review board at each institution [7], and it was approved by the steering committee of the Institutional Review Board in Chonnam National University Hospital (IRB No. CNUH-2011-172).
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki of the World Medical Association [8]. The protocol of this study was approved by the steering committee of the institutional review board in Chonnam National University Hospital (IRB No. CNUH-2022-376). The requirement for obtaining informed consent was waived owing to the studyŌĆÖs retrospective nature.
Study design
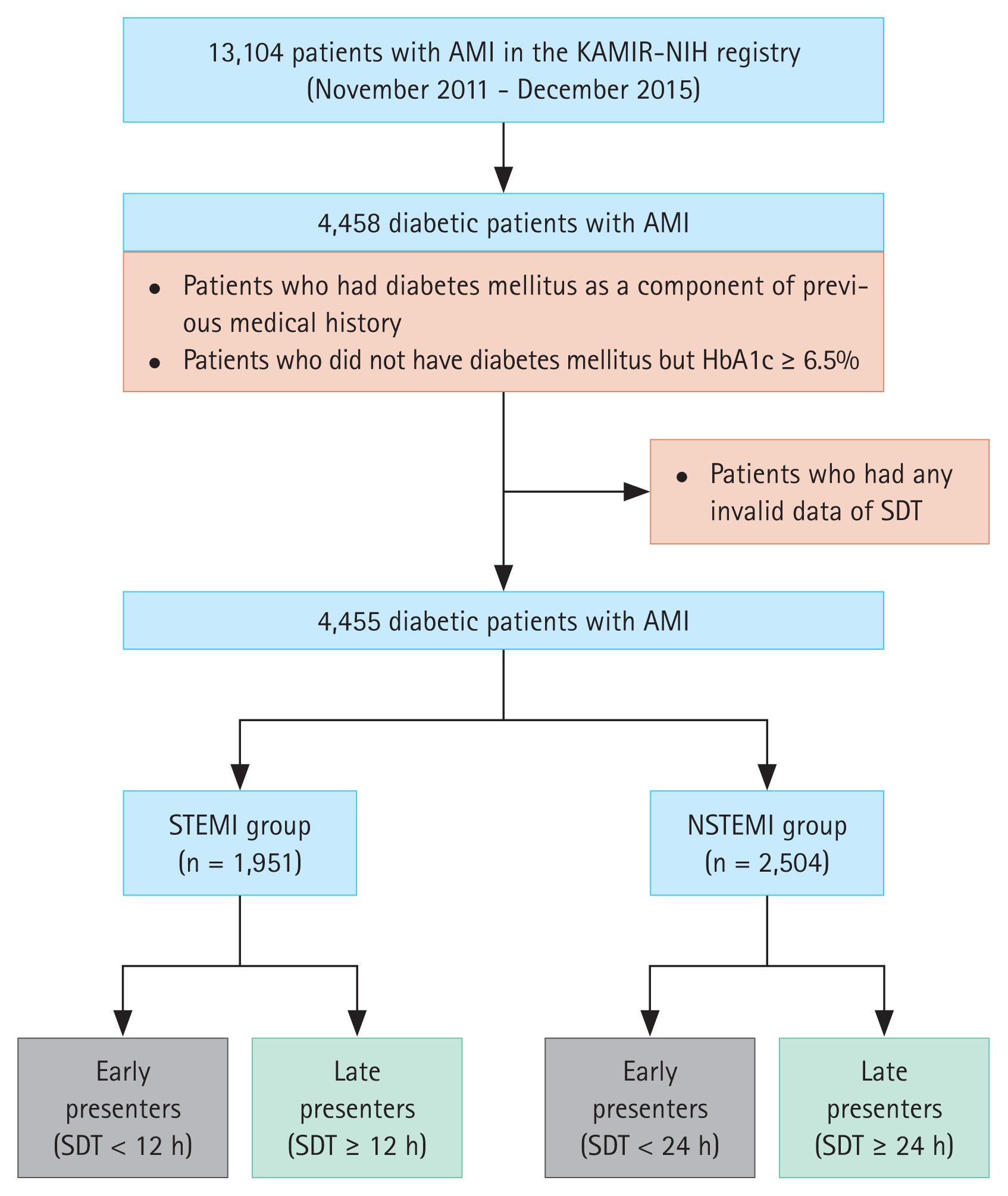
The study scheme is illustrated in Figure 1. In total, 4,458 participants with AMI and concomitant DM out of the 13,104 participants from the KAMIR-NIH registry were primarily selected after including (1) those who had DM as a component of previous medical history or (2) those who did not have DM but glycated hemoglobin (HbA1c) Ōēź 6.5%. After excluding those who had any invalid data of symptom-to-door time (SDT), 4,455 patients were selected and categorized into two groups depending on the final diagnosis (ST-elevation myocardial infarction [STEMI; n = 1,951] or non-STEMI [NSTEMI; n = 2,504]). Each group was subdivided into early and late presenters according to SDT.
Definitions
Several contemporary guidelines and standards define AMI as an increase or decrease in the values of cardiac biomarkers and one or more of the following conditions: (1) symptoms or signs of myocardial ischemia; (2) ischemic findings in the electrocardiogram, such as ST-segment deviation, T-wave inversion, or development of pathological Q-waves; (3) cardiac imaging evidence indicating loss of viable myocardium or abnormal regional wall motion; and (4) existence of intracoronary thrombus determined using coronary angiography. STEMI refers to a medical condition combining AMI elements and new onset ST-segment elevation in two or more continuous leads [9,10].
The presence of DM was considered if the patient had DM as one of the previous comorbid diseases or showed HbA1c levels Ōēź 6.5% at the initial presentation. A family history of ischemic heart disease was defined as a previous or current medical history of coronary artery disease or heart failure (HF) in any of the patientŌĆÖs immediate family members. Imaging guidance during the index PCI was defined as using intracoronary imaging modalities such as optical coherence tomography or intravascular ultrasound. Left main coronary artery (LMCA) disease was defined as 50% narrowing of the LMCA. Multivessel disease was defined as the presence of significant stenosis in Ōēź 2 epicardial coronary arteries, indicating either Ōēź 70% stenosis in Ōēź 2 coronary arteries or Ōēź 70% narrowing in one coronary artery with LMCA. To quantify and stratify the degree of antegrade intracoronary flow, we utilized the thrombolysis in myocardial infarction flow grading system [11]. Left ventricular ejection fraction (LVEF) was estimated using two-dimensional transthoracic echocardiography. The infarct-related artery was defined as the coronary artery responsible for the symptoms and/or signs of AMI with plaque disruption and thrombus formation. The lesion characteristics within the infarct-related artery were stratified using the American College of Cardiology/American Heart Association lesion classification [12]. The definitions of all these parameters were determined by the steering committee board of the KAMIR-NIH registry [7,13].
The definition of the time to presentation of AMI was based on SDT, which is the interval from symptom onset to presentation at the hospital. Specifically, in STEMI patients, late presentation was determined when SDT was Ōēź 12 hours, while in NSTEMI patients, late presentation was determined when SDT was Ōēź 24 hours. These criteria were based on previously published studies [6,14].
Three-year mortality outcomes
The clinical follow-up was conducted for approximately 36 months. Regarding treatment estimates, the primary endpoint was all-cause mortality, a composite of cardiac and non-cardiac death. Secondary endpoints included both cardiac and non-cardiac death.
Statistical analysis
As mentioned, all participants were subdivided into STEMI and NSTEMI groups. Further, the two groups were subdivided into early and late presenters, according to SDT. These subgroups were compared in terms of baseline clinical and procedural characteristics and mortality outcomes. Continuous data are described as means with standard deviation and were compared using a 2-tailed StudentŌĆÖs t-test or analysis of variance, whereas discrete (categorical) data are described as frequencies with percentages and were compared using the PearsonŌĆÖs chi-square test and FisherŌĆÖs two-by-two exact test. p value < 0.05 was considered statistically significant.
Our analysis was intended to determine whether time to presentation is independently associated with mortality among patients with DM and AMI, a sizable subgroup of the overall AMI population. To minimize selection bias due to baseline characteristics between two groups, we fit the inverse probability of treatment weighting (IPTW) as an exact matching method with statistical adjustment for residual confounders. The propensity scores were constructed with 30ŌĆō31 baseline covariates (for the overall population, 31 covariates were used, and for both the STEMI and NSTEMI groups, 30 were used), and they were directly used as inverse weights to estimate the average treatment effect [15,16]. These covariates included final diagnosis (STEMI vs.NSTEMI), sex, age, emergency medical service (EMS) utilization, Killip class (Killip class IIIŌĆōIV vs. IŌĆōII), body mass index, previous history, smoking, family history of ischemic heart disease, HbA1c strata (< 6.5%, 6.5ŌĆō9.0%, and Ōēź 9.0%), LVEF, use of PCI, vascular approach (femoral versus radial approach), use of glycoprotein IIb/IIIa inhibitors, thrombus aspiration, imaging guidance, infarct-related artery, lesion characteristics, thrombolysis in myocardial infarction flow grade, LMCA disease, multivessel disease, use of thrombolysis and discharge medications.
Survival curves were plotted via the KaplanŌĆōMeier method. The log-rank test was used to compare treatment estimates between the two groups. Participants with missing data in these variables or no follow-up were excluded from the survival analysis.
In addition, we further evaluated the mortality outcomes in accordance with the degree of dysglycemia. After utilizing Cox-proportional hazards regression models, adjusted hazard ratios (HRs) for primary and secondary endpoints were estimated between the three different HbA1c strata. In this regression model, the independent variables contained final diagnosis (STEMI vs. NSTEMI), time to presentation (early vs. late presentation), sex, age, EMS utilization, Killip class, body mass index, previous history, smoking, family history of ischemic heart disease, LVEF, use of PCI, vascular approach (femoral versus radial approach), use of glycoprotein IIb/IIIa inhibitors, thrombus aspiration, imaging guidance, infarct-related artery, lesion characteristics, thrombolysis in myocardial infarction flow grade, LMCA disease, multivessel disease, use of thrombolysis and discharge medications.
Data manipulation and analysis was conducted using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
In total, 4,455 participants with AMI and DM were included in the statistical analysis; 43.8% (n = 1,951) were diagnosed with STEMI, and 56.2% (n = 2,504) with NSTEMI. The proportion of late presenters was 17.5% for STEMI and 29.0% for NSTEMI. The baseline clinical and procedural characteristics that demonstrate different trends in the early and late presenters are summarized in Table 1.
Overall, late presenters were older and were more often female, with relatively lower utilization of EMS than early presenters. Both hypertension and DM were more prevalent in the late presenters than in the early presenters. In contrast, late presenters had lower proportions of smokers and a less prevalent family history of ischemic heart disease than their counterparts. The late presenters had lower LVEF and initial thrombolysis in myocardial infarction flow grades, but a higher LMCA disease prevalence than the early presenters. The late presenters received less PCI with lower rates of the femoral approach and thrombus aspiration than the early presenters. Beta-blockers, renin-angiotensin system inhibitors (i.e., angiotensin-converting enzyme inhibitors or angiotensin receptor blockers), and statins were less frequently prescribed for the late presenters than for the early presenters.
In the STEMI group, late presenters were older and had a greater proportion of female patients with lower application of EMS than did the early presenters; moreover, the late presenters smoked less, had a lower LVEF, and received less PCI and fewer prescribed medications, such as beta-blockers, renin-angiotensin system inhibitors and statins. In the STEMI group, the rate of in-hospital death was statistically higher in late presenters than in early presenters. In the NSTEMI group, similar trends were observed regarding the distributions of age, sex, EMS use, smoking history, and LVEF. However, the rates of PCI and medication prescriptions were comparable between the early and late presenters in the NSTEMI group. The early presenters were more likely to undergo thrombus aspiration than the late presenters in this group.
The baseline characteristics after adjustment for baseline covariates with IPTW are shown in Supplementary Table 1.
Three-year mortality outcomes
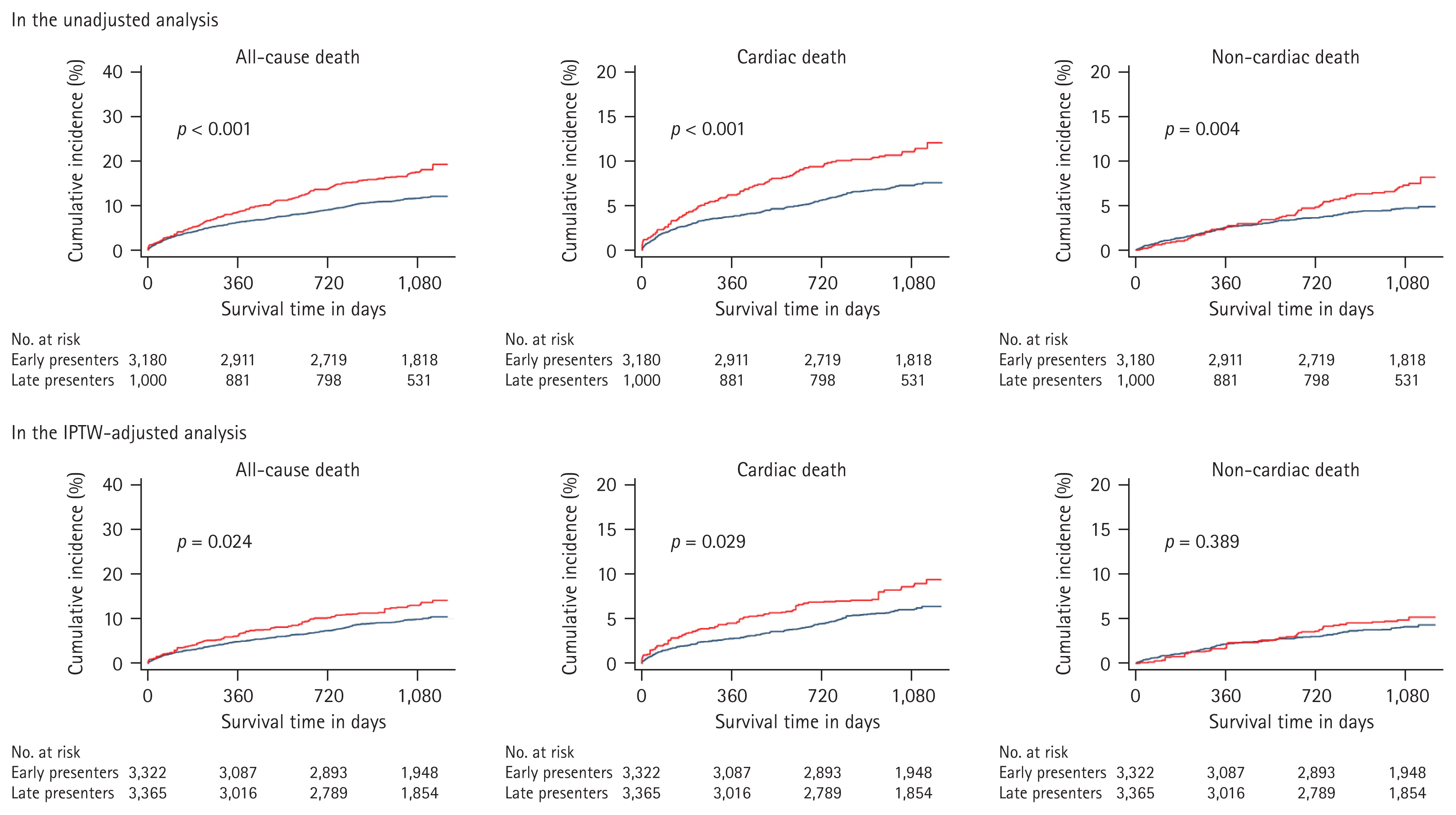
Among the total patient population (n = 4,455), 218 patients were deceased during the index hospitalization, and 57 were lost to follow-up. After excluding them, 4,180 participants were successfully treated, discharged, followed-up, and included in the mortality outcome statistical analysis. The mortality outcomes are summarized in Table 2. The median follow-up intervals were 1,089, 1,090, and 1,088 days in the overall population, STEMI group, and NSTEMI group, respectively. Compared to early presenters, the incidence of all-cause mortality in late presenters was consistently higher in the overall population (11.4 vs. 17.2%; p < 0.001), STEMI group (8.3 vs. 14.8%; p < 0.001), and NSTEMI group (14.1 vs. 18.2%; p = 0.010). Compared to their counterparts, the late presenters had higher incidences of cardiac death in the overall population (7.0 vs. 10.7%; p < 0.001) and STEMI group (4.8 vs. 10.5%; p < 0.001) and non-cardiac death in the overall population (4.4 vs. 6.5%; p = 0.007) and NSTEMI group (5.2 vs. 7.5%; p = 0.032).
In the IPTW-adjusted analysis, although statistically insignificant, the incidence of all-cause mortality was numerically higher in the late presenters than in the early presenters among the overall population (9.1 vs. 12.4%; p = 0.072). Compared to the early presenters, the late presenters had a higher incidence of cardiac death in the STEMI group (4.2 vs. 9.7%; p = 0.034), but had similar incidences in the overall population (5.4 vs. 8.0%; p = 0.113) and NSTEMI group (6.5 vs. 6.5%; p = 0.984).
In the survival analysis using the log-rank test, the cumulative incidence of all-cause mortality was significantly higher in late presenters than in early presenters before and after covariate adjustment with IPTW (Fig. 2).
Stratified analysis according to the initial HbA1c level
We also conducted further stratified analysis according to the initial HbA1c level of each participant, which is summarized in Table 3. Compared to early presenters, late presenters had higher incidences of all-cause mortality with HbA1c of both < 6.5% (adjusted HR: 1.74, 95% confidence interval [CI]: 1.19ŌĆō2.54) and 6.5ŌĆō9.0% (adjusted HR: 1.43, 95% CI: 1.08ŌĆō1.89). After covariate adjustment using IPTW, this difference only persisted in patients with HbA1c < 6.5% (adjusted HR: 2.53, 95% CI: 1.34ŌĆō4.76). In the patients with HbA1c Ōēź 9.0%, however, adjusted HR was comparable between two groups before (adjusted HR: 1.45, 95% CI: 0.80ŌĆō2.64) and after covariate adjustment using IPTW (adjusted HR: 0.82, 95% CI: 0.40ŌĆō1.67).
DISCUSSION
We compared the three-year mortality outcomes among patients with AMI and concomitant DM according to the time to presentation (early vs. late presenters). In the unadjusted data, late presentation worsened the mortality outcomes in the overall population and STEMI and NSTEMI groups. In the overall population, the incidences of both the primary and secondary endpoints were significantly higher in late presenters than in early presenters. In the STEMI group, late presenters had a significantly higher incidence of the primary endpoint, mainly due to an increase in cardiac death. In the NSTEMI group, on the other hand, they had a significantly higher incidence of the primary endpoint, mainly due to an increase in non-cardiac death. Although these different outcomes were statistically attenuated in the weighted dataset after adjusting baseline covariates, thereby the incidence of the primary endpoint was just numerically higher in late presenters than in their counterparts, the survival analysis demonstrated consistent results before and after covariate adjustments.
In the overall population, late presenters tended to be females, older and less likely to receive EMS. At the time to presentation, STEMI diagnosis was higher in early presenters than in late presenters. While early presenters tended to smoke more and had a higher proportion of family history of ischemic heart disease, late presenters had higher proportions of hypertension and DM but lower LVEF. The early presenters received more PCI-intensive medical treatment, with higher prescription rates of beta-blockers, renin-angiotensin system inhibitors, and statins. In early presenters, angiographic and procedural profiles showed lower initial thrombolysis in myocardial infarction flow grades, but more patients received both femoral approach and thrombus aspiration as opposed to their late presenting counterparts.
The trends in the distribution of age, sex, EMS utilization, smokers, and patients with LVEF < 40% in the overall population were also maintained in both the STEMI and NSTEMI groups. In the STEMI group, early presenters received more PCI and more intensive medical treatments than late presenters, with higher prescription rates of beta-blockers, renin-angiotensin system inhibitors, and statins. In addition, in-hospital death rate was lower in early presenters than in late presenters. In the NSTEMI group, however, these differences were not observed; only differences in the rate of thrombus aspiration were observed.
Given that both women and older patients often complain of atypical or absent chest symptoms [17,18], these patients have significant pre-hospital delays [19], and the distributions of age and sex in the study population were sufficiently predictable. Additionally, the lower EMS utilization among the late presenters was sufficiently explanatory, as women are known to utilize EMS less, in accordance with a previous clinical study [19].
Early presenters had a higher proportion of smokers, and this trend is sufficiently supported by well-established evidence regarding the male predominance of tobacco use [20]. The different proportions of male patients in the subgroups may have influenced the biased finding of these smoking populations. Additionally, they had more STEMI and better LVEF than did the late presenters. These findings are sufficiently predictable, given that one clinical study revealed that smokers tend to have more STEMI and better LVEF than non-smokers [21]. Patients with STEMI tend to present complete occlusion of the infarct-related artery than those with NSTEMI [22,23]. Primary PCI is strongly recommended for rapid reperfusion in the STEMI setting [24]. The relatively high incidence of STEMI was likely associated with a lower thrombolysis in myocardial infarction flow grade, which might have influenced the higher rates of PCI, the femoral approach, and thrombus aspiration, than those of their counterparts.
Meanwhile, early presenters received more medications, including beta-blockers, renin-angiotensin system inhibitors, and statins than late presenters. This trend was maintained in the STEMI group. According to another study based on the KAMIR-NIH registry [25], patients treated with PCI received optimal medical therapy than those not treated with PCI. Although the previous study was limited to a nonagenarian AMI population, the results seem consistent with our findings. However, additional studies are needed to confirm these results.
Late presentation adversely affects mortality outcomes, including mortality in both STEMI and NSTEMI [6,14,26,27]. Late presenters with diabetes are at an increased risk of delayed diagnosis and treatment because they are more likely to experience AMI without characteristic chest symptoms [28,29]. In the present study, the proportion of late presenters was higher than that of the general AMI population, as evidenced by other studies (17.5 vs. 11% in STEMI and 29.0 vs. 27.9% in NSTEMI, respectively) [6,14]. According to further analysis of the study participants regarding the features of chest pain as summarized in Supplementary Table 2, approximately 18% of the study population (n = 803) was brought to cardiovascular centers with atypical or no chest pain, similar to other studies based on the Korean AMI population [19,30]. Patients without typical chest pain tended to be older and had pre-hospital delay with more prolonged SDT, higher proportions of females, NSTEMI, Killip classes IIIŌĆōIV, and a higher incidence of in-hospital death than their counterparts. According to clinical studies conducted in South Korea [19,27], both advanced age and female sex are associated with delayed hospital presentation in the AMI setting. Female or older patients with AMI often present with atypical signs or symptoms, as supported by many previous studies [17,31].
According to our HbA1c-based stratified analysis (Table 3), we also found the differential effect of hospital presentation timing on mortality according to initial HbA1c level. Given that HbA1c reflects the cumulative glycemic status of the recent 2ŌĆō3 months [32], these observations suggest that the mortality benefits of early presentation seem to be attenuated under the circumstance with poor glycemic control. It seems to be in line with a previously published study, which demonstrated no prognostic difference between patients with diabetes with and without SDT prolongation [33]. These similarities on all-cause mortality at a higher HbA1c level may be moderately explained by the fact that dysglycemia itself contributes to high rates of adverse cardiovascular outcomes, including mortality [34], and result in greater infarct sizes [34]. Moreover, it would be explained by the ŌĆ£legacy effect,ŌĆØ which means that uncontrolled hyperglycemia leads to endothelial dysfunction on coronary beds [35], therefore results in high angiographic severity such as multivessel disease [36], which consequently attenuates clinical benefits of rapid reperfusion such as in primary PCI.
Interestingly, there were insignificant results related to cardiac death in the NSTEMI group, whereas the STEMI group demonstrated significant differences in terms of both all-cause mortality and cardiac death. Despite not fully accountable but even speculative, patients with STEMI more often have complete occlusion of IRA than those with NSTEMI. Complete blockage of blood supply may exhaust available oxygen in a few moments [37]. Contrarily, low but remnant oxygen levels on account of the partial or incomplete blockage of blood supply may support the myocardial tissues to preserve sufficient levels of adenosine triphosphate, thereby survive for an extended period of time [38]. Therefore, the beneficial effect of early presentation on cardiac death may be more prominent in the STEMI group than in the NSTEMI group.
Meanwhile, this insignificant finding may also be explained to some extent through our further analysis of the NSTEMI group in accordance to different time windows of presentation (Supplementary Table 3, Supplementary Fig. 1). In this analysis, a relative decrease from the third 12-hour interval (36ŌĆō48 h) to the fourth 12-hour interval (Ōēź 48 h) was found, and it could be due to several factors. First, the fourth 12-hour interval received more delayed invasive strategy with slightly higher proportion of door-to-balloon time Ōēź 24 hours, compared to the third 12-hour interval. This tendency may be due to some differences in clinical background, such as relatively low initial LVEF in the fourth 12-hour interval, which meant that the prevalence of HF at initial presentation was higher in the fourth 12-hour interval compared to the third 12-hour interval. Despite theoretical benefits of early invasive strategy providing more opportunities for rapid revascularization and myocardial salvage [39], with accumulative evidence supporting this [40,41], this strategy can also deteriorate clinical outcomes with worsened heart function complicated by contrast-induced acute kidney injury, PCI-induced no reflow phenomenon, or ischemia/reperfusion injury [42ŌĆō44]. Moreover, since a Korean study demonstrated that delayed invasive strategy appears to be one of the reasonable treatments in patients with NSTEMI and concomitant HF [45], our results seem to be expected and imply that many clinicians are still reluctant to perform early invasive strategy in the real-world practice.
There are many published clinical studies on the association of late presentation, represented by SDT prolongation, with outcomes in the AMI population [19,26,27,46ŌĆō48]. Nonetheless, there is insufficient clinical evidence regarding this relationship between patients with AMI and concomitant DM. We examined these associations from the database of the KAMIR-NIH registry and concluded that late presentation was associated with a poorer clinical course in this population.
The results of the present study should be interpreted with caution, owing to several key limitations. First, because the present study was a non-randomized retrospective analysis, no causal relationship can be derived between the time to presentation and mortality outcomes among patients with AMI and concomitant DM. Second, there could be selection bias due to several reasons. Despite adjusting baseline covariates, missing data and the possibility of unmeasured confounders could have caused selection bias. Selection bias could also occur in the data selection process with inclusion and exclusion criteria in the study design. Third, the KAMIR-NIH is a nationwide multicenter observational cohort, and it only includes tertiary cardiovascular institutions. This cohort did not represent the real-world patterns of clinical practice in AMI, including small-and medium-sized medical centers; therefore, it is difficult to generalize our results to all medical centers in the Republic of Korea.
We evaluated the association between time to presentation and mortality outcomes among patients with AMI and concomitant DM. Compared to the AMI population without DM, the proportion of late presenters was high in this population. Late presentation may worsen mortality outcomes; thus, multifaceted and systematic interventions are needed to decrease pre-hospital delays in this population.
KEY MESSAGE
1. Early presentation can confer mortality benefits among patients with diabetes and AMI, like in the general AMI population.
2. Especially, the beneficial effect of early presentation on cardiac death may be more prominent in patients with diabetes and ST-elevation myocardial infarction than in those with DM and non-ST-elevation myocardial infarction.
3. Despite a well-established mortality benefit of rapid reperfusion represented by early presentation, this benefit seems to be attenuated under the circumstance with poor glycemic control.
4. Since late presentation is associated with higher mortality rates in patients with diabetes and AMI, systemic and continued efforts are required to reduce pre-hospital delay, thereby improving mortality outcomes in this population.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





