


INTRODUCTION
It is well known that patients with acute myocardial infarction (AMI) have a higher risk of ischemic events than patients with stable coronary artery disease. Many studies have shown that potent P2Y12 receptor inhibitors (RIs), such as ticagrelor or prasugrel, could reduce ischemic events compared with clopidogrel in patients with acute coronary syndrome (ACS) [1–3]. Therefore, recent guidelines for the treatment of AMI have reported that ticagrelor or prasugrel over clopidogrel is recommended before percutaneous coronary intervention (PCI) and maintained over 12 months unless there are contraindications such as an excessive risk of bleeding [4,5]. Nevertheless, recent studies of patients with AMI in East Asians reported that potent P2Y12RIs could increase the risk of bleeding rather than reduce ischemic events [6–8]. Therefore, in actual clinical practice, it tends to be frequently used to intentionally switch between a potent P2Y12RI and clopidogrel depending on the patient’s baseline characteristics, clinical conditions, or physician’s decision. However, while a previous study has shown that early post-discharge switches from potent P2Y12RI to clopidogrel (the P-C) were not associated with an increased risk of ischemic events in stabilized AMI patients [9], another study has found that P2Y12RI switching after discharge from index admission was associated with adverse clinical adverse events during 1-year follow-up [10]. However, the current status and clinical outcomes of in-hospital P2Y12RI switching remain unknown.
Therefore, the purpose of our study was to assess the current status of in-hospital P2Y12RI switching and to investigate which P2Y12RI affected the clinical events before and after P2Y12RI switching.
METHODS
Study population
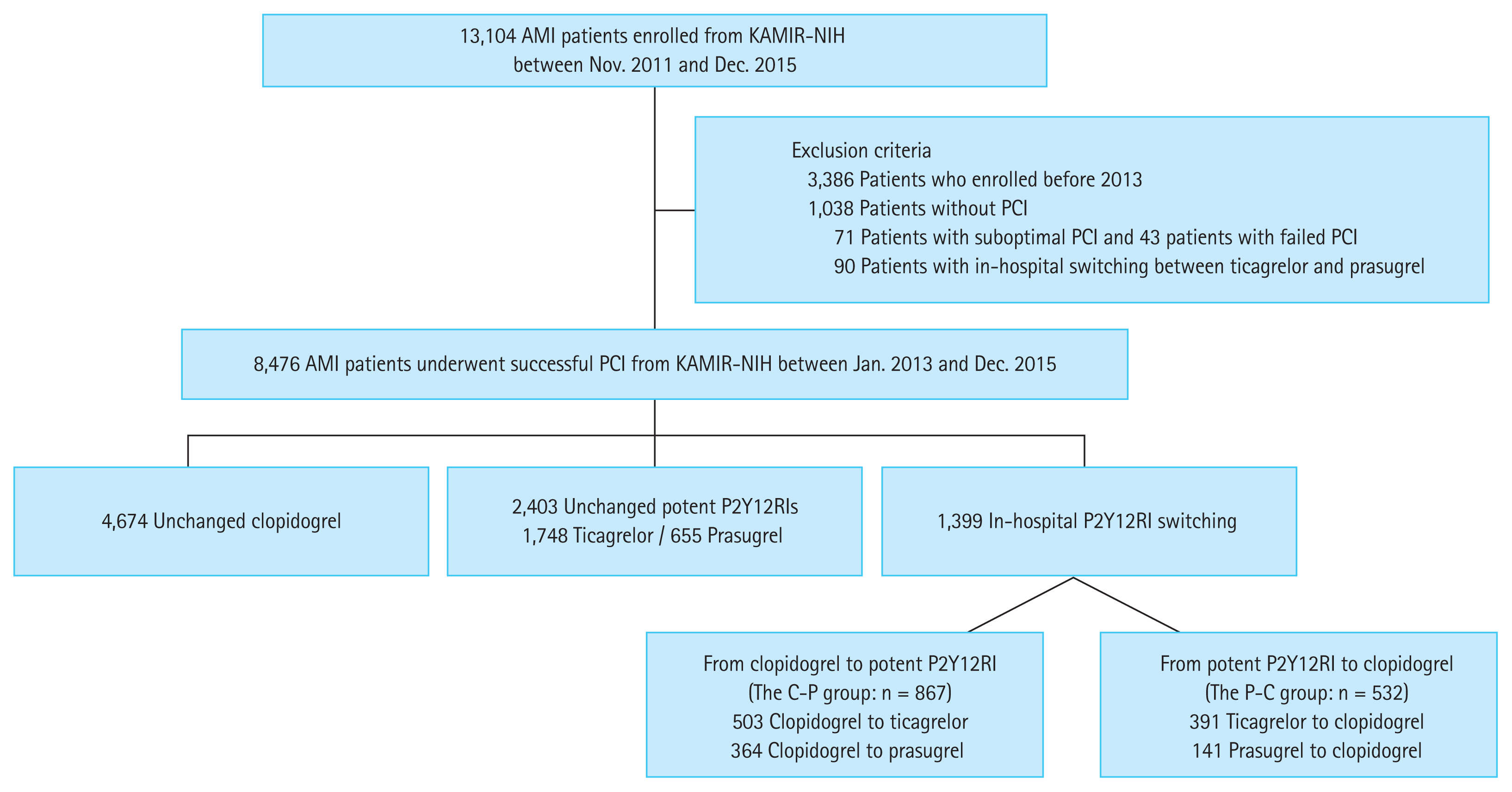
We analyzed 13,104 patients with AMI between November 2011 and December 2015 from the Korea Acute Myocardial Infarction Registry-National Institute of Health (KAMIR-NIH), which is a prospective, multicenter, web-based observational cohort study from 20 centers in South Korea [11]. We excluded patients who were enrolled before 2013, those who did not undergo PCI, those with suboptimal or failed PCI, and those with in-hospital switching between potent P2Y12RIs (ticagrelor and prasugrel). According to in-hospital P2Y12RI strategies, we divided the enrolled patients into three groups: unchanged clopidogrel, unchanged potent P2Y12RIs, and in-hospital P2Y12RI switching. Patients with in-hospital P2Y12RI switching could be subdivided into two groups: those who switched from clopidogrel to potent P2Y12RI (the C-P) and those who switched the P-C. Unfortunately, we could not know exactly why P2Y12RIs were switched during hospitalization, because KAMIR-NIH was an observational study with no variables to explain it. Therefore, we investigated each clinical event before and after P2Y12RI switching to determine if there was a cause-and-effect relationship between P2Y12RI switching and clinical events and to evaluate which P2Y12RI affected the ischemic and bleeding events. We also examined whether the loading dose (LD) was administered just before P2Y12RI switching and compared the clinical outcomes between patients with and without LD.
The study protocols were approved by the Institutional Review Board of each participating center and conducted in accordance with the Declaration of Helsinki 2013. Written informed consent was obtained from all patients for participation in the study. The approval numbers were CNUH-2011-172 and CNUH-2022-003 of Chonnam National University Hospital, and CHOSUN 2021-11-002 of Chosun University Hospital. Trained study coordinators at each participating institution collected data using a formalized form.
Determination of events-related P2Y12RIs
In principle, the P2Y12RIs administered when a clinical event occurred were considered event-related P2Y12RIs. However, it is well known that the efficacy of potent P2Y12RIs appears immediately after administration and lasts for at least 3 days after discontinuation (especially ticagrelor) [12,13]. Therefore, it could be considered that pre-switching potent P2Y12RIs were related to bleeding events that occurred within at least 3 days after switching to clopidogrel, and post-switching potent P2Y12RIs were related to bleeding events that occurred just after switching from clopidogrel (the day of switching). Conversely, pre-switching clopidogrel was related to bleeding events that occurred before switching, and post-switching clopidogrel was related to bleeding events 7 days after switching from potent P2Y12RIs. However, since it was unclear which P2Y12RI was related to bleeding events that occurred 4 days after switching from ticagrelor to clopidogrel, the bleeding-related P2Y12RI was considered to be “indeterminate.” When ischemic events occurred within a few days after P2Y12RI switching, it was very difficult to determine whether the ischemic events were directly related to post-switching P2Y12RIs or the persistent severe clinical conditions resulting from pre-switching P2Y12RIs. Therefore, in these cases, the ischemic event-related P2Y12RI was also considered to be “indeterminate.”
Intervention and medications
The choice of antiplatelet agents (clopidogrel, prasugrel, or ticagrelor), antithrombotic therapy, the timing of invasive strategies (primary or early or delayed), vascular assessment sites, pre- or post-dilatation, type of stents, and use of periprocedural glycoprotein IIb/IIIa inhibitors were determined based on the clinical status of AMI patients according to the clinical decision of operators in each institute. Antiplatelet agents were administered to all patients prior to PCI, with aspirin 300 mg LD and clopidogrel 300 or 600 mg LD or prasugrel 60 mg LD or ticagrelor 180 mg LD. Simultaneously, PCI was performed in a standard and conventional manner. After the intervention, all patients were required to take one of the following three P2Y12RIs along with aspirin, which included a maintenance dose (MD) of clopidogrel 75 mg once a day, 10 mg or 5 mg MD of prasugrel once a day, or 90 mg ticagrelor twice a day. It was customary to continue dual antiplatelet therapy (DAPT) for at least 12 months in our registry, if possible. However, P2Y12RIs were unrestrictedly switched according to the physician’s decision. In addition, they were free to decide whether to administer the LD before switching. Other medical treatments based on standard therapies for AMI patients were also freely administered, considering the patient’s condition.
Study endpoints
Primary composite endpoints were net adverse cardiovascular events (NACEs), defined as a composite of cardiac death, nonfatal MI, stroke, or thrombolysis in myocardial infarction (TIMI) major bleeding during hospitalization. The efficacy outcomes were major adverse cardiovascular events (MACEs), defined as a composite of cardiac death, non-fatal myocardial infarction (MI), definite stent thrombosis, or stroke during hospitalization. The safety outcome was TIMI major bleeding during hospitalization. Secondary endpoints were the individual component endpoints, and TIMI major or minor bleeding during hospitalization. Non-fatal MI was defined as reinfarction, which was diagnosed by comprehensively considering the clinical signs or symptoms, the criteria of electrocardiogram diagnosis, or significant changes in cardiac troponin based on the Third Universal Definition of Myocardial Infarction [14], and the periprocedural myocardial injury or infarction was rigorously excluded. Stroke was defined as the inclusion of both ischemic and hemorrhagic stroke.
Statistical analysis
Categorical variables are expressed as frequencies and percentages and continuous variables as mean ± standard error of mean. Categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test, as appropriate, and continuous variables were assessed using Student’s t test or one-way analysis of variance. When we performed pairwise comparisons between any two groups, the Bonferroni correction method was used.
To minimize the effect of selection bias between in-hospital P2Y12RI strategies, first, a multivariate logistic regression model with an “enter” method was performed using the independent variables for all individual outcome components. Only variables with a p value < 0.05 in the univariate analysis were included in the multivariate model. It was also used to compare clinical outcomes between four subdivided subgroups and between patients with and without LD. Second, the propensity score (PS) was estimated using a multivariable logistic regression model, wherein the in-hospital P2Y12RI switching strategy was checked in reverse on all baseline clinical, angiographic, and procedural characteristics and in-hospital medications. Thereafter, both patients with unchanged clopidogrel and those with unchanged potent P2Y12RIs were one-to-one matched with those with in-hospital P2Y12RI switching as per the PS using the nearest neighbor matching within a caliper width of 0.05 of the standard deviation of the logit of the PS. Third, patients were weighted based on the probability of each individual receiving a specific treatment given the confounders and adjusted using the inverse probability weight (IPW) method. The weights were 1/PS in patients with in-hospital P2Y12RI switching and 1 / (1 − PS) in patients with unchanged clopidogrel and those with unchanged potent P2Y12RIs. The balance between the two groups after PS matching or IPW adjustment was assessed by calculating the standardized mean difference (SMD). The SMD was calculated by dividing the difference in means or proportions by standard error and was considered an imbalance if the absolute value was greater than 0.10. All variables were well balanced, except for aspirin, due to the small sample size (Supplementary Table 1). All statistical tests were two-tailed, and a p value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS for Windows version 27.0 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics of all the patients
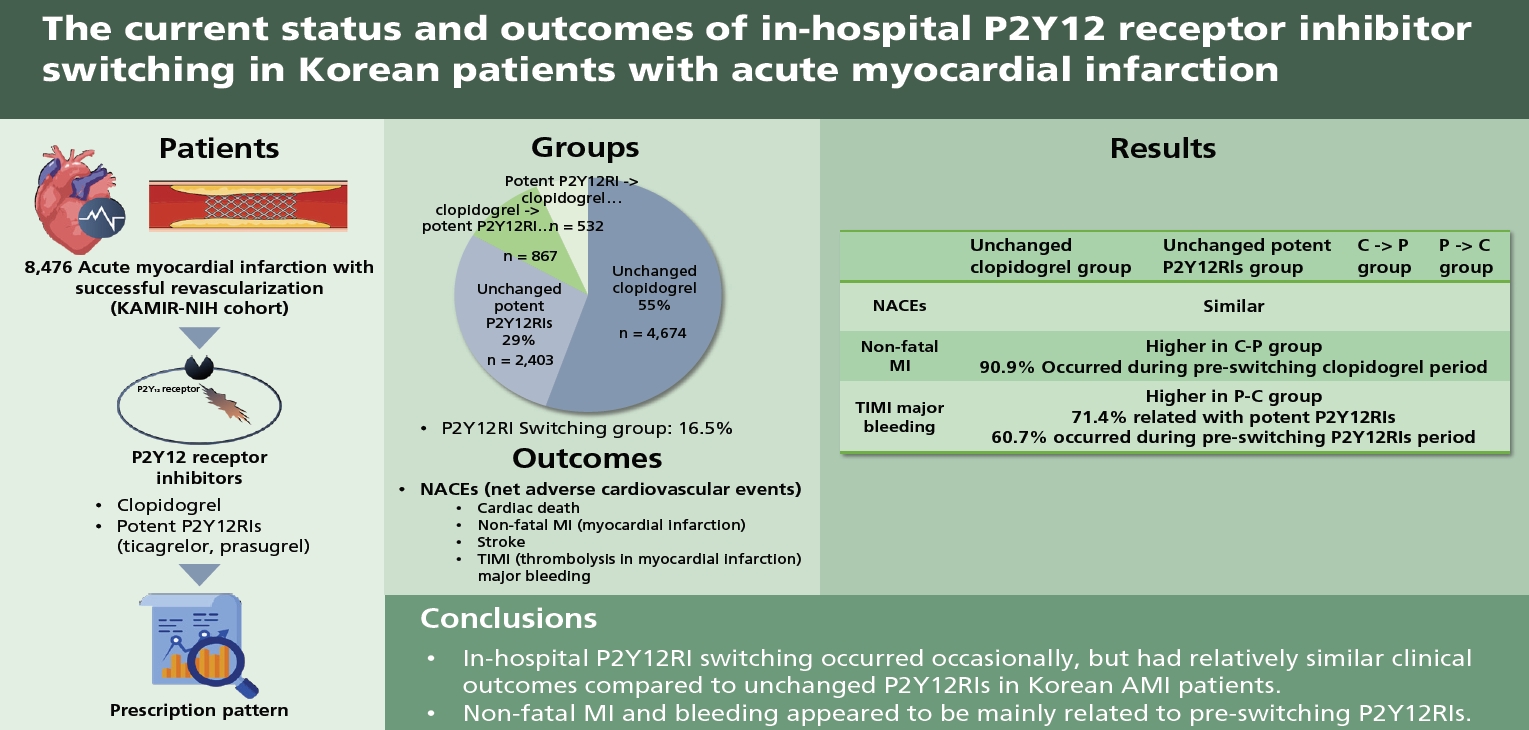
Between January 2013 and December 2015, a total of 8,476 AMI patients who underwent successful PCI were analyzed from the KAMIR-NIH. Among them, 4,674 patients (55.1%) were continuously administered clopidogrel, 2,403 patients (28.4%) were continuously administered with a potent P2Y12RI, and 1,399 patients (16.5%) were switched between clopidogrel and a potent P2Y12RI during hospitalization. Switching from clopidogrel to ticagrelor occurred in 503 patients, and switching from clopidogrel to prasugrel in 364 patients (the C-P group, all 867 patients). Switching from ticagrelor to clopidogrel occurred in 391 patients and from prasugrel to clopidogrel in 141 patients (the P-C group, all 532 patients) (Fig. 1).
There were significant differences in baseline clinical and procedural characteristics and in-hospital medications between the three groups (Table 1). The average period of hospital stay in the in-hospital P2Y12RI switching group was 6.48 ± 0.19 days, that from admission to P2Y12RI switching was 2.14 ± 0.08 days, and that from PCI to P2Y12RI switching was 1.62 ± 0.76 days. In 74.9% (1,048 patients) of the P2Y12RI switching group, P2Y12RIs were switched within 2 days after PCI.
Clinical outcomes between unchanged P2Y12RIs and P2Y12RI switching
There were no significant differences in NACEs among the unchanged clopidogrel, the unchanged potent P2Y12RIs, and P2Y12RI switching groups (Table 2). However, TIMI major or minor bleeding was significantly higher in the P2Y12RI switching group than those in the unchanged clopidogrel group. Consistent results were observed after all confounding variables were adjusted using multivariate regression, PS matching, and IPW analysis (Supplementary Table 2).
Clinical outcomes between the unchanged P2Y12RIs, the C-P, and the P-C groups
There were also no significant differences in NACEs among the four groups (Table 2). However, the C-P group had a higher incidence of non-fatal MI compared to that in the unchanged clopidogrel and unchanged potent P2Y12RIs groups, and the P-C group had a higher incidence of TIMI major bleeding compared to that in the unchanged clopidogrel group (Table 3).
The in-hospital P2Y12RI switching and the timing of clinical events
A large amount of total ischemic (27/35 patients, 77.1%) and total bleeding events (45/66 patients, 68.2%) occurred within 3 days before and after P2Y12RI switching (between D-3 and D+3).
Twelve patients (0.9%) experienced both ischemic and bleeding events before or after P2Y12RI switching. The in-hospital clinical progress summary of 12 patients is shown in Supplementary Table 3. The definite cases of ischemic events that developed after in-hospital switching from potent P2Y12RIs to clopidogrel due to bleeding events were numbers 1, 2, 6, and 7, and the bleeding event that developed after in-hospital switching from clopidogrel to a potent P2Y12RI due to an ischemic event was number 12.
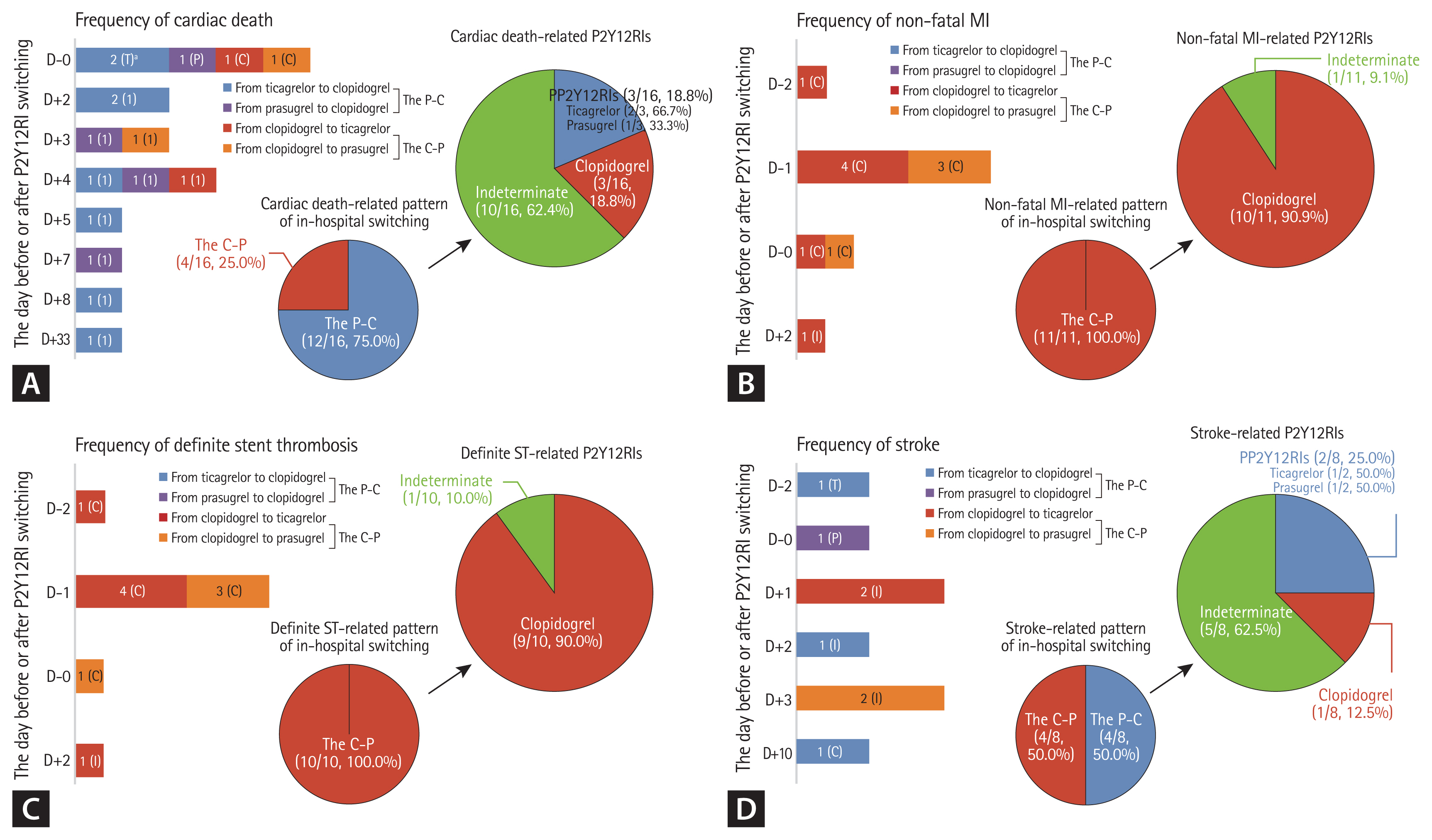
Most of the cardiac deaths (12/16 patients, 75%) occurred in the P-C group. However, in most cases, it was not clear which P2Y12RI was related to cardiac death, except in cases that occurred on the day of P2Y12RI switching (D-0) and 33 days after P2Y12RI switching (D+33). Therefore, 62.4% of all cardiac deaths (10/16 patients) remained indeterminate in cardiac death-related P2Y12RI (Fig. 2A).
All nonfatal MI occurred in the C-P group, and most of them (10/11 patients, 90.9%) occurred during the administration of clopidogrel before switching, or on the day of P2Y12RI switching (D-0). Therefore, nonfatal MI appeared to be strongly associated with pre-switching clopidogrel (Fig. 2B).
Most of the definite stent thromboses (9/10 patients, 90.0%) also were related to pre-switching clopidogrel, however, many cases of the all strokes-related P2Y12RI (5/8 patients, 62.5%) remained indeterminate (Fig. 2C and 2D).
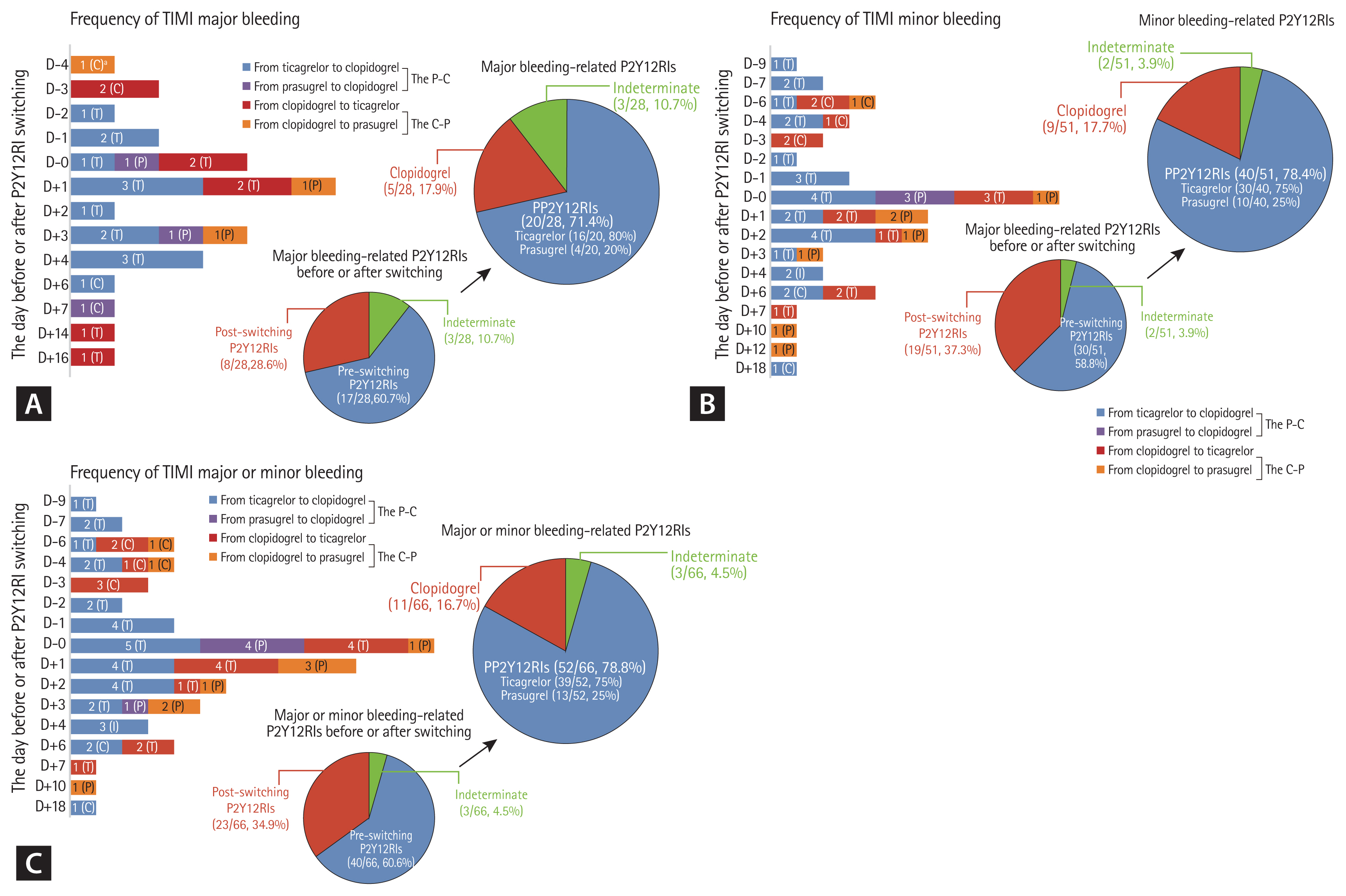
Thirteen patients had both TIMI major and minor bleeding. Moreover, 60.7% of TIMI major bleeding (17/28 patients), 58.8% of TIMI minor bleeding (30/51 patients), and 60.6% of TIMI major or minor bleeding were related to pre-switching P2Y12RIs (Fig. 3). Further, 42.8% of TIMI major bleeding (12/28 patients) and 48.5% of TIMI major or minor bleeding (32/66 patients) were related to pre-switching potent P2Y12RIs, and 28.6% of TIMI major bleeding (8/26 patients) and 30.3% of TIMI major or minor bleeding (20/66 patients) were related to post-switching potent P2Y12RIs. Therefore, potent P2Y12RIs were strongly related to TIMI major bleeding (20/28 patients, 71.4%) and TIMI major or minor bleeding (52/66 patients, 78.8%) (Fig. 3A and 3C).
Clinical outcomes between no LD and LD before switching
Baseline clinical and procedural characteristics and in-hospital medications were observed between the no LD and LD groups in both the C-P and the P-C groups (Supplementary Table 4). Only 21.6% of the P2Y12RI switching group (302/1,399 patients) received a LD of P2Y12RIs before switching. Of these, 22.8% of the C-P group (198/867 patients) were given a LD of potent P2Y12RIs (180 mg in ticagrelor or 30 to 60 mg in prasugrel), and 19.6% of the P-C group (104/532 patients) were given a LD of clopidogrel (300 to 600 mg) just before switching. Through multivariate regression analysis, there were no significant differences in MACEs, NACEs, and TIMI major bleeding between no LD and with LD of both the C-P and the P-C groups (Table 4).
Only three out of 10 patients who had suffered MI during pre-switching clopidogrel were switched to potent P2Y12RIs with a LD. Conversely, even though TIMI major or minor bleeding had already occurred before switching, including on the day of P2Y12RI switching (D-0), two patients in the C-P group and six patients in the P-C group were switched to P2Y12RIs with a LD followed by MD.
DISCUSSION
Our study was conducted to assess the clinical outcomes of in-hospital P2Y12RI switching compared to unchanged P2Y12RIs and to determine the clinical event-related P2Y12RIs before and after switching in Korean patients with AMI. The main findings of our study are that in-hospital P2Y12RI switching occurred occasionally (16.5%) and had no significant differences in NACEs compared to unchanged P2Y12RIs. Non-fatal MI and TIMI major bleeding were mainly related to pre-switching P2Y12RIs and in-hospital bleeding complications were still strongly related to potent P2Y12RIs. Therefore, it appears that in-hospital P2Y12RI switching was not the cause of clinical events, but a response to expected or already occurring clinical events.
Western registries reported that switching antiplatelet therapy from one agent to another during the index hospitalization ranged from 5% to 60% [15,16]. In the Switching from Clopidogrel to New Oral Antiplatelet Agents during PErcutaneous Coronary Intervention (SCOPE) registry, switching of oral antiplatelet therapies occurred in approximately 10% of ACS patients within the first month after the acute event [17]. Our study showed that the incidence of in-hospital P2Y12RI switching was 16.5% from KAMIR-NIH, which is not uncommon compared to Western registries.
This was a retrospective study using data from KAMIR-NIH between 2013 and 2015, the early period when ticagrelor or prasugrel was introduced and used in South Korea. Despite the fact that the bleeding risk of potent P2Y12RIs in East Asian patients was still unknown, in-hospital P2Y12RI switching was not infrequent and occurred mainly 2 days after PCI. Although it is not known exactly from KAMIR-NIH data why P2Y12RIs were switched during hospitalization, it is estimated that the angiographic features and the result of PCI had a great influence on the decision of in-hospital P2Y12RI switching. In actual clinical practice, P2Y12RI switching may be attributed to a variety of factors, including the clinical setting, patient characteristics, concomitant therapies, costs, social issues, development of side effects, medication adherence, and patient/physician preference [18]. Our study showed that most of the total ischemic or bleeding events in the P2Y12RI switching group occurred within 3 days before and after P2Y12RI switching; therefore, it appears that the adverse clinical event was one of the major factors causing in-hospital P2Y12RI switching in our clinical practice.
Our study showed that the incidences of MACEs and NACEs in the P2Y12RI switching groups were 2.5% and 4.1%, respectively, which were not significantly different compared to unchanged clopidogrel and to unchanged potent P2Y12RIs groups. Even considering that there were many P2Y12RI switching before or after adverse events in actual clinical practice, the event rate of the P2Y12RI switching group appears to be acceptable compared to the unchanged P2Y12RIs. In particular, it was very rare for an ischemic event to occur after P2Y12RIs were switched due to bleeding and vice versa. We have always been concerned about increasing ischemic risk after de-escalation of P2Y12RIs in the acute phase of MI patients; however, there was no difference in MACEs between the unchanged potent P2Y12RIs and the P-C groups in our study. Therefore, even though the current guidelines do not recommend P2Y12RI switching during hospitalization, it seems that selective in-hospital switching from potent P2Y12RIs to clopidogrel could be effective in reducing in-hospital bleeding only for Korean AMI patients who are not at high risk of ischemia. However, large-scale, long-term, randomized trials are required to establish the efficacy and safety of in-hospital P2Y12RIs in Korean patients with AMI.
A previous study, which showed high incidences of MI, stroke, and bleeding in the P2Y12RI switching group, from Korean AMI patients from the Health Insurance Review and Assessment Service (HIRA) database [10] differs from our study in many ways. Our study assessed in-hospital P2Y12RI switching outcomes in older patients and patients with acute-phase MI, but the HIRA study assessed 1-year outcomes of P2Y12RI switching in patients with stabilized MI after discharge. Therefore, our study showed a relatively higher incidence of all-cause death and bleeding and a lower incidence of MI and stroke compared to the HIRA study. However, since non-fatal MI was much higher in the C-P group and bleeding was much higher in the P-C group than that in the unchanged clopidogrel group in our study, the results of our study also appear to be similar to those of the HIRA study. However, it should be noted that our study tried to determine the correlation between pre- or post-switching P2Y12RIs and adverse clinical events and found that many non-fatal MI and bleeding events were mainly related to pre-switching P2Y12RIs. This result means that P2Y12RI switching was more likely not a direct cause of adverse clinical events. We believe that the HIRA study should also have analyzed the causal relationship between switching and clinical events to accurately evaluate the impact of P2Y12RI switching; therefore, much attention is needed in interpreting its findings.
To date, there have been several studies on the efficacy and safety of P2Y12RIs in Korean patients with AMI; however, most of these studies have excluded patients with in-hospital P2Y12RI switching from the analysis [6,19,20]. This is because two or more P2Y12RIs are used, making it difficult to assess the outcomes of a single P2Y12RI. Our study on event-related P2Y12RI in the in-hospital P2Y12RI switching group showed that nonfatal MI was related to clopidogrel, and bleeding was related to potent P2Y12RIs. When we judged these results in combination with previous studies on the efficacy and safety of potent P2Y12RIs, potent P2Y12RIs still had a high bleeding tendency in Korean patients with AMI. Since East Asians have the lowest thrombogenicity compared to other races, East Asian patients with cardiovascular disease have reduced anti-ischemic benefits and elevated bleeding risk with antithrombotic therapy, including potent P2Y12RIs, compared to Caucasian patients [21]. In addition, although the effect of reducing ischemic events of potent P2Y12RIs was significant in the early phase after PCI when compared to clopidogrel, the risk of bleeding was continuously and gradually increasing during the maintenance phase of DAPT [22]. Therefore, clinical trials to find the best strategy for reducing bleeding without increasing ischemia in East Asian patients are mostly about the de-escalation strategy of potent P2Y12RIs [23–25]. However, most of the trials on de-escalation that have been or are in progress have decided to switch potent P2Y12RIs after at least 1 month following PCI; therefore, our findings may provide basic data for the in-hospital de-escalation strategy of potent P2Y12RIs in the future.
International expert consensus on switching platelet P2Y12RI therapies recommended that in the acute/early phase (≤ 30 days from the index event), switching should occur with the administration of LD in most cases, except for patients who are de-escalating therapy because of bleeding or bleeding concerns [26]. We do not know exactly why the rate of P2Y12RI loading before switching was low (21.6%) in our study and could not find that LD administration was necessarily consistent with the clinical events. Some cases of inappropriate loading were observed, such as not loading when switching after MI occurrence, loading when switching after bleeding, or switching to a potent P2Y12RI even after bleeding occurred. However, there were no significant differences in ischemic and bleeding events between the no LD and LD groups in our study. We believe that the LD should be properly administered as recommended in the guidelines for in-hospital switching; however, further studies on the impact of LD before switching are needed in East Asian patients who are known to have a high risk of bleeding.
Our study had several limitations. First, we could not exactly determine the reasons for in-hospital P2Y12RI switching because of the limitation of registry data. Therefore, it was impossible to accurately assess whether the switching of P2Y12RI affected adverse clinical events, even though we analyzed the association between pre- or post-switching P2Y12RIs and adverse clinical events. Furthermore, in-hospital events may be related to other clinical factors in addition to P2Y12RIs. However, we are confident that the results of our study can identify the current status of in-hospital P2Y12RI switching and provide basic data for further studies on the optimal timing of P2Y12RI switching. Second, our study was based on a nonrandomized, prospective, and observational registry; therefore, selection bias could not be completely avoided when comparing between in-hospital P2Y12RI switching and unchanged P2Y12RI groups, although it was partially compensated by multivariate logistic regression, PS-matched, and IPW-adjusted analyses. Third, our study was a small, nonrandomized cohort study that assessed the efficacy and safety of LD before switching; therefore, selection bias was hardly avoidable and the ischemic event rates were very low. Therefore, our study was underpowered to evaluate the benefit of reducing ischemic events according to LD before switching. Fourth, there were few medical records regarding other adverse effects of P2Y12RI including dyspnea, heart block, and no external bleeding or any overt bleeding that did not meet any of the TIMI major or minor bleeding criteria.
In conclusion, our study showed that in-hospital P2Y12RI switching occurred occasionally, but had relatively similar clinical outcomes compared to unchanged P2Y12RIs. Non-fatal MI and bleeding events in the in-hospital P2Y12RI switching group appeared to be mainly related to pre-switching P2Y12RIs, and in-hospital bleeding complications were still strongly related to potent P2Y12RIs in Korean AMI patients. Therefore, further, large, long-term randomized trials are needed to evaluate the efficacy and safety of in-hospital P2Y12RI switching and to determine the optimal timing of potent P2Y12RI switching in Korean AMI patients who underwent PCI.
KEY MESSAGE
1. In-hospital P2Y12 receptor inhibitor (RI) switching occurred occasionally (16.5%), but had relatively similar clinical outcomes compared to unchanged P2Y12RIs in Korean acute myocardial infarction patients.
2. Non-fatal myocardial infarction and bleeding events in patients with in-hospital P2Y12RI switching appeared to be mainly related to pre-switching P2Y12RIs.
3. The rate of P2Y12RI loading before in-hospital switching was low (21.6%); therefore, loading should be properly administered as recommended in the guidelines.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





