


INTRODUCTION
Atrial fibrillation (AF) is a common arrhythmia with increasing incidence [1]. AF is associated with considerable morbidity and mortality including heart failure (HF) and stroke [2]. Therefore, screening for AF is important, and various screening tools have been suggested [3]. Nonetheless, it remains under-diagnosed due to asymptomatic patients. In addition, systematic screening of AF exhibited low-cost effectiveness [4]. Ultimately, it is important to identify patients who are at high risk of AF.
Obesity, high blood pressure, and alcohol consumption are associated with incident AF [5–7]. These conditions are modifiable risk factors resulting in adverse atrial remodeling and potential HF if left uncontrolled. Physical activity is associated with the development of AF, and AF patients exhibit a decrease in exercise capacity [8]. A decrease in cardiorespiratory fitness is associated with an increased risk of AF [9]. Cardiopulmonary exercise testing (CPX) is a non-invasive indicator for assessing the cardiovascular and pulmonary components of exercise responses. The impact of exercise capacity according to CPX on the risk of AF in healthy individuals remains unknown. Therefore, we aimed to examine the association of exercise capacity with the risk of incident AF in healthy subjects within a 3-year study period.
METHODS
This was a retrospective study that utilized a health promotion center database. The population who visited the healthcare center for comprehensive health evaluations between January 2008 and December 2020 were enrolled. We compared patients who exhibited new-onset AF to the AF-free control population. This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center in the Republic of Korea (IRB number: 2021-04-022-001). IRB approved a request to waive the need for informed consent. The research presents no more than minimal risk of harm to the subjects and involves no procedures for which written consent is required.
Study population
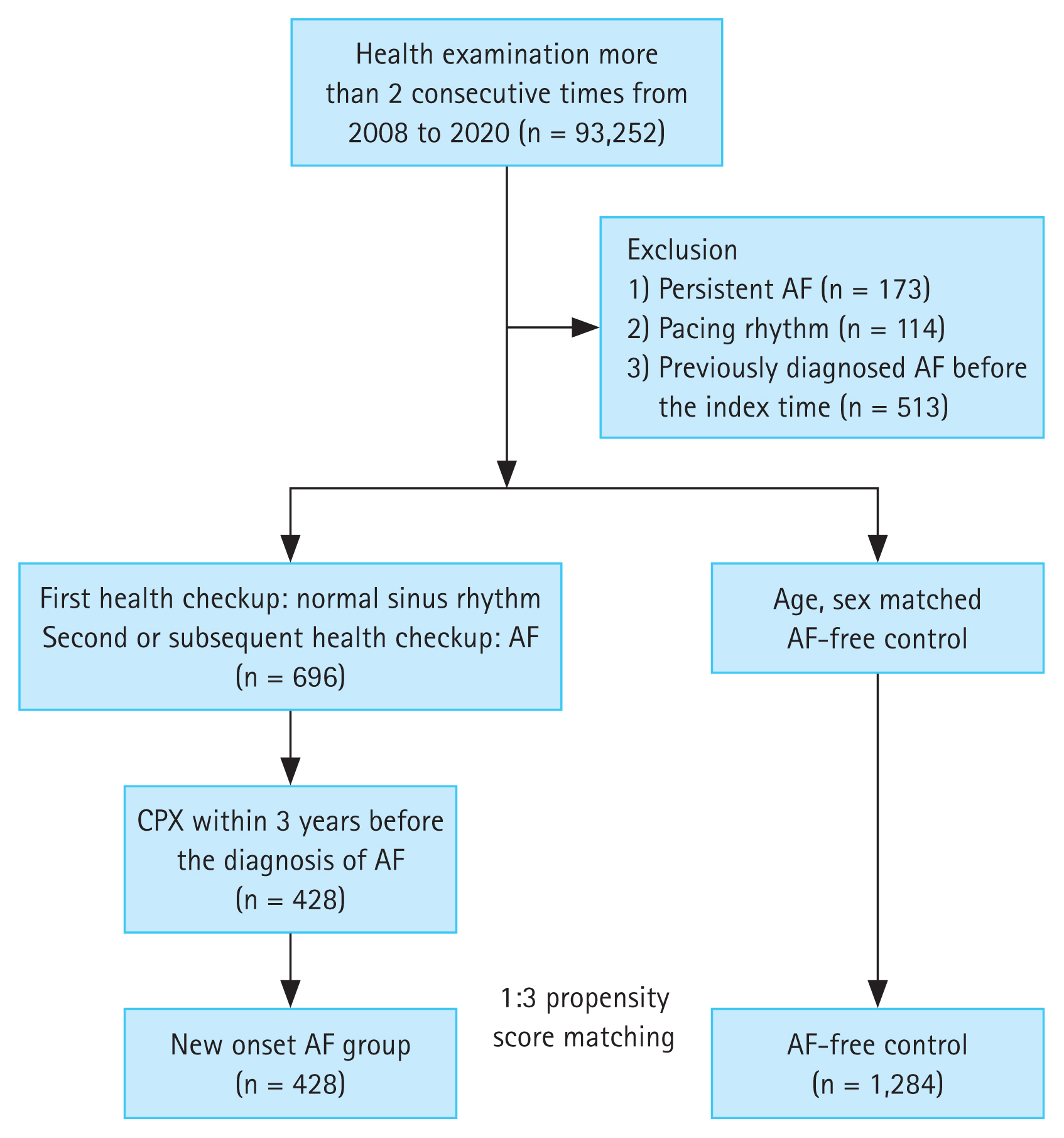
We evaluated asymptomatic adults older than 18 years of age who had undergone more than 2 consecutive health checkups. We included subjects who exhibited normal sinus rhythm on the first health examination and who developed AF by electrocardiogram (ECG) on the second or subsequent health examinations. The timing of AF diagnosis was defined as the index time. We excluded subjects who exhibited persistent AF or pacing rhythm, and who were diagnosed with AF at the first health examination or identified with AF in our electronic health records system according to the diagnostic code before the index time. Subjects who underwent CPX within 3 years before the diagnosis of AF were examined. An AF-free control population, matched for age and sex, was randomly selected from the same database as the case population. We examined covariates including basic demographic data, comorbidities, and results of the health checkups (Fig. 1).
Cardiopulmonary exercise testing
Exercise testing was performed in an exercise laboratory supervised by an exercise physiologist. The subjects underwent maximal, symptom-limited metabolic treadmill (Quinton Q4500; Cardiac Science Corp., Bothell, WA, USA) exercise testing using the Bruce or modified Bruce protocol according to age and exercise capacity. Measurements of ventilator gases during exercise were performed using Trueone 2400 (Parvo Medics, Sandy, UT, USA). Subjects underwent 12-lead ECG, and heart rate and systolic and diastolic blood pressures (SBP, DBP) were measured at baseline, during each stage, and in the recovery phase. In addition, oxygen consumption (VO2), carbon dioxide production (VCO2), and minute ventilation (VE) values were obtained. Finally, the following calculations were performed [10]:
Peak oxygen consumption (pVO2) was defined as maximum oxygen consumption calculated using established equations based on age and sex. Aerobic capacity was defined as peak VO2.
Metabolic equivalents (METs) were used to represent exercise capacity.
Peak rate pressure product (RPP) represents myocardial oxygen consumption which was calculated by multiplying SBP with heart rate.
Statistical analyses
The baseline characteristics are presented as the mean ± standard deviation for continuous variables and as frequency with percentage for categorical variables. Continuous variables were compared using the unpaired t-test, while categorical variables were compared using either the χ2 test or Fisher’s exact test as appropriate. The AF and control groups were matched at a 1:3 ratio according to age and sex. We performed logistic regression and calculated univariate odds ratios (ORs) for the risk factors. In addition, the risk of new-onset AF was assessed using a multivariable logistic regression model including hypertension, diabetes, and BMI and is presented as adjusted OR and 95% confidence interval (CI). p values < 0.05 were considered statistically significant. All statistical analysis was performed using SAS software, Version 9.3 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
In total, 93,252 patients who had undergone health examination more than two consecutive times from 2008 to 2020 were screened; 800 patients were excluded according to the exclusion criteria. Overall, 696 patients developed new-onset AF during the second or subsequent health checkups. Among these, 428 underwent CPX within 3 years before the diagnosis of AF. Finally, the study population in the analyses included 428 cases (mean age 58.4 ± 7.6 yr, male 95.6%) with 1,284 controls (mean age 58.1 ± 7.4 yr, male 96.2%). Body mass index (BMI) was higher in the case group (25.2 ± 2.7 vs. 24.4 ± 2.7 kg/m2) as was hypertension (40.6% vs. 31.8%) compared to the control. The baseline characteristics of the patients are summarized in Table 1. In logistic regression analysis, the OR for body weight was 1.04 (95% CI 1.03–1.05) and 1.10 (95% CI 1.06–1.15) for BMI.
Cardiopulmonary exercise testing parameters
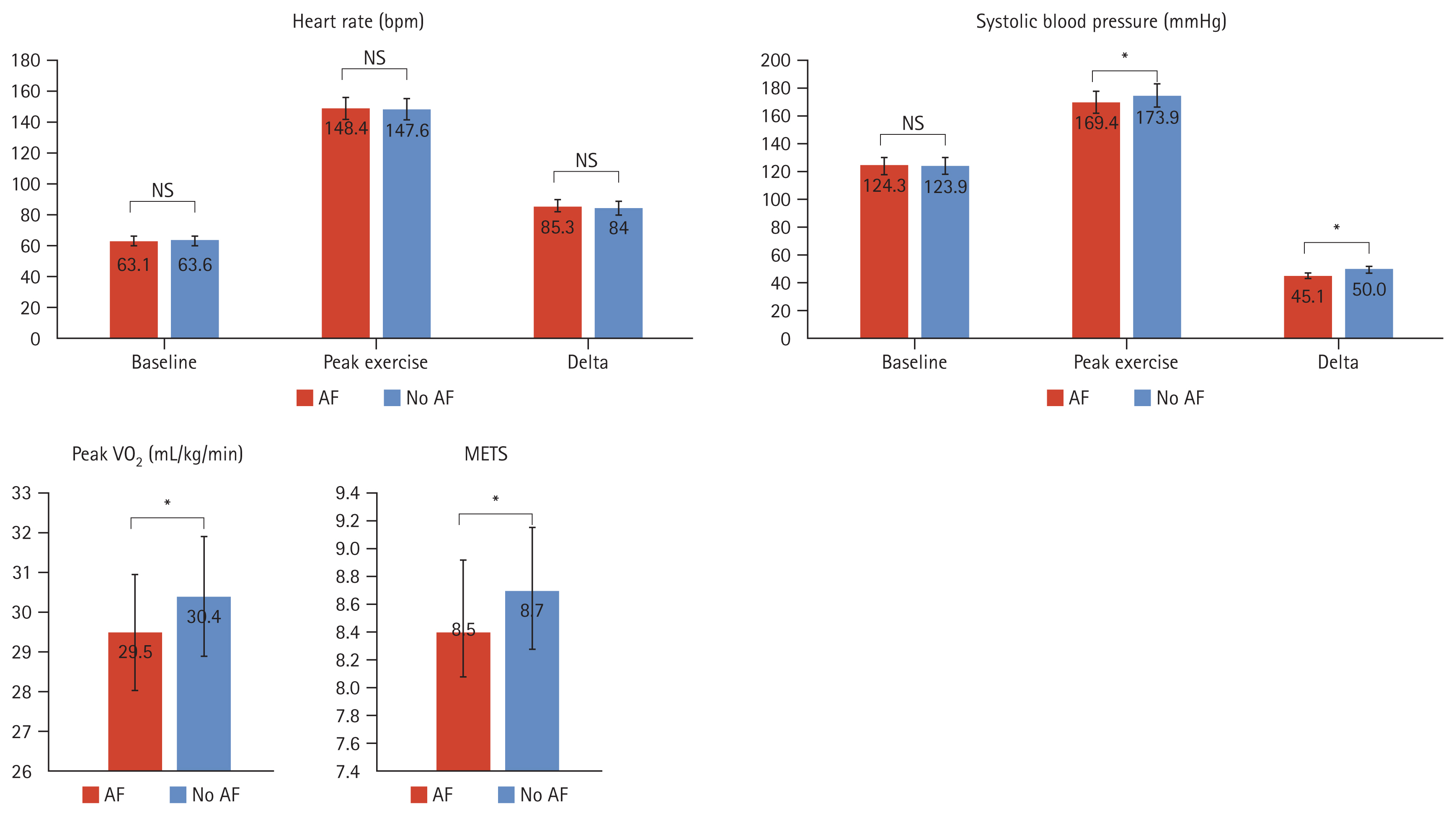
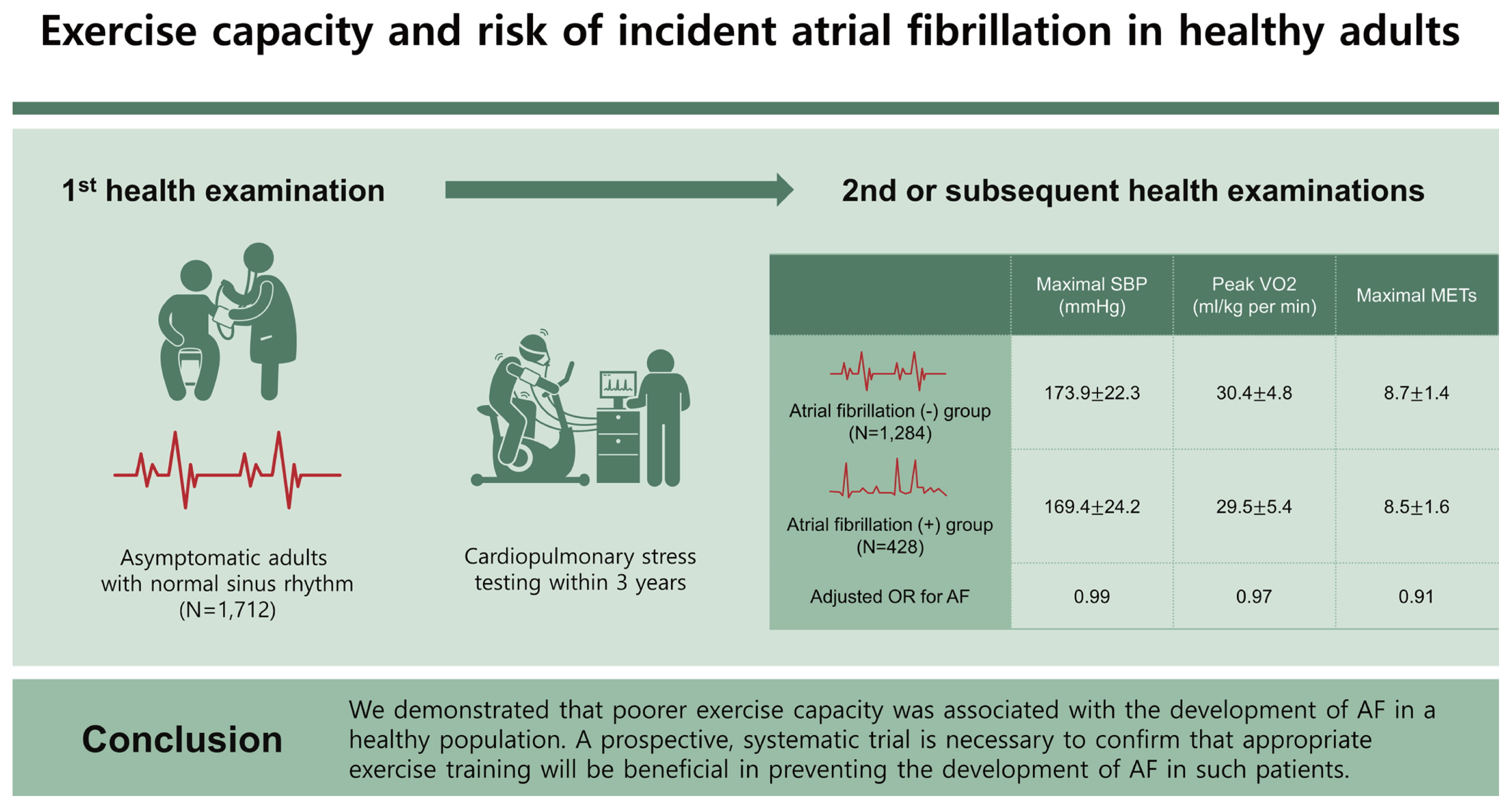
Exercise parameters are summarized in Table 2. Most of the parameters were within the normal range. There were significant differences in maximal SBP (case 169.4 ± 24.2 vs. control 173.9 ± 22.3 mmHg), peak VO2 (29.5 ± 5.4 vs. 30.4 ± 4.8 mL/kg per minute), and maximal METs (8.5 ± 1.6 vs. 8.7 ± 1.4) between the two groups (Fig. 2). In the univariate analysis, the crude ORs were 0.99 for maximal SBP (95% CI 0.98–1.00), 0.96 for peak VO2 (95% CI 0.94–0.99), and 0.89 for maximal METs (95% CI 0.82–0.96). In the multivariable logistic model, adjusted OR was 0.99 for maximal SBP (95% CI 0.98–0.99), 0.97 for peak VO2 (95% CI 0.95–0.99), and 0.91 for maximal METs (95% CI 0.83–0.98).
DISCUSSION
We examined the prognostic value of exercise parameters associated with incident AF in health checkup subjects. In our analysis, we demonstrated that poorer exercise capacity was associated with the development of AF. In the adjusted model, every 1 MET increase was associated with a 9% risk reduction of incident AF, and a 1 mL/kg/min increase in peak VO2 was associated with a 3% risk reduction of incident AF.
Cardiopulmonary exercise testing
CPX is a combination of standard exercise testing and the measurement of ventilator gas exchange amounts for assessing exercise capacity in patients suspected of having cardiovascular or pulmonary disease [11]. Several reports have indicated that AF is associated with a decrease in exercise capacity. Several studies have also shown that peak VO2 is decreased in patients with AF, especially in HF [12,13]. Most studies analyzed patients with cardiovascular disease including AF or HF. In our study, we evaluated healthy subjects who had never been diagnosed with AF, and the parameters of exercise testing were within normal limits in those subjects and the AF groups. We suggest that a subtle decrease in exercise capacity is prognostic of the future development of AF in a healthy population. In heart rate and DBP response during exercise, no significant differences in baseline, maximal, and delta heart rates were observed between the two groups. Subjects who developed AF within 3 years exhibited similar baseline SBP but 5 mmHg lower maximal and delta SBP. Hemodynamic responses to exercise depend on cardiac output and peripheral resistance. Therefore, SBP typically increases with exercise, while DBP remains the same or decreases [10]. In other words, an inadequate increase in SBP during exercise reflects impaired contractile reserve and circulatory impairment. In a previous study, peak SBP was 10 mmHg lower in patients with AF compared to those without AF [14]. These results indicate that exercise performance progressively decreases in patients with subsequent AF development. We excluded CPX data more than 3 years prior to the occurrence of AF, assuming that the change in exercise capacity or atriopathy would be reflected within 3 years. Subjects who were included in our study underwent CPX for health checkups and not for suspicion of other cardiac diseases or complaints. Therefore, our study may represent the prognostic effectiveness of CPX in a healthy population.
Risk factors of AF
Obesity, especially with lean body mass, and alcohol consumption are known risk factors for AF [5,15]. Recently, body weight fluctuation, dynamic changes in hemoglobin levels, and blood pressure variability have been suggested to be associated with increased risk of incident AF [16–18]. Lifestyle modifications and a multifaceted educational intervention are needed to prevent or optimize treatment of AF. Higher physical activity is also associated with lower AF incidence [19]. However, competitive athletes or endurance-type activities including marathon runners exhibit increased risk for developing AF [20]. Therefore, regular exercise at the appropriate intensity may have a protective effect against AF and can be a modifiable risk factor [21]. We demonstrated the relationship between exercise capacity and incident AF within 3 years in a healthy population. This suggested the possibility that exercise training may protect against the development of AF. Further systematic prospective studies are needed to confirm this finding.
Limitations
This is a retrospective, single-center study from a health checkup database. We excluded subjects who were previously diagnosed with AF according to our electronic health records system. Nevertheless, it is possible that some subclinical AF patients might have been included in both groups. Selection bias may exist because not all subjects underwent all of the exams. In addition, some variables were not included in the analysis. For example, we could not analyze echocardiography or medications due to the absence of data. We attempted to adjust for other risk factors of AF but could not identify and adjust for all confounding variables.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





