


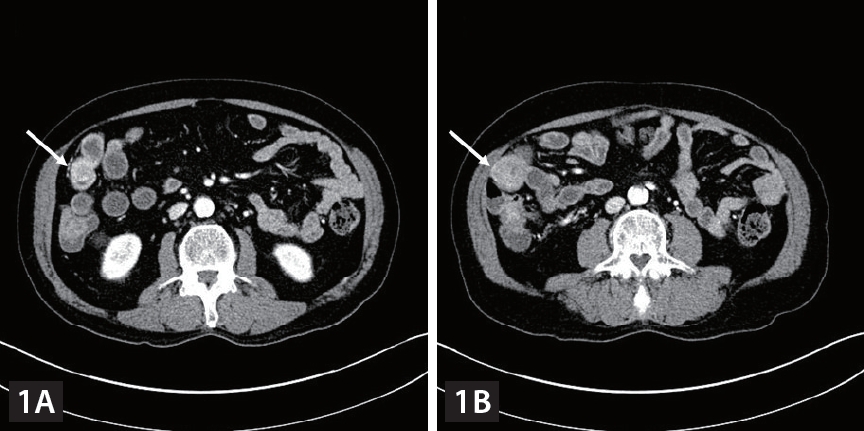
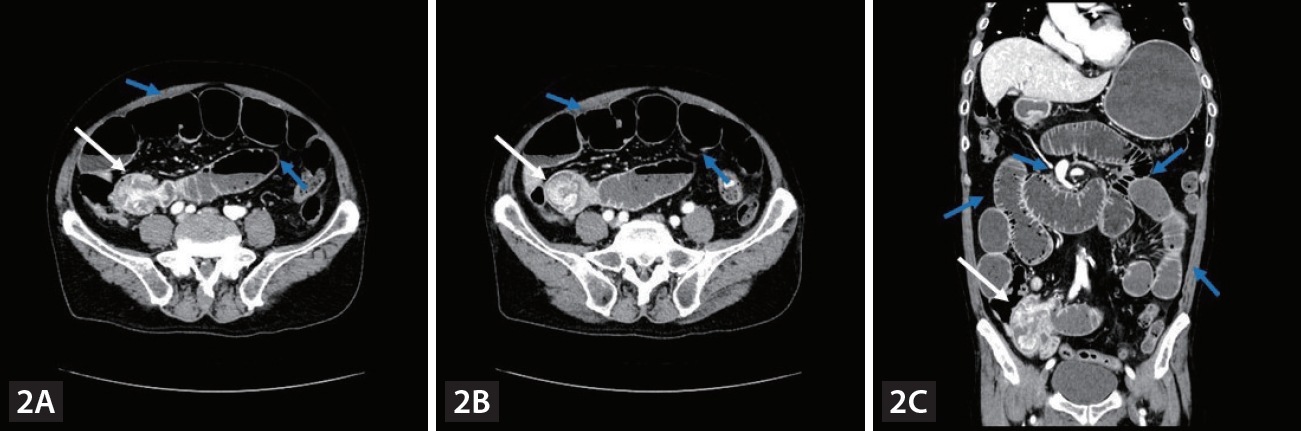
A 75-year-old man with chronic hepatitis B was diagnosed with pulmonary metastases from hepatocellular carcinoma (HCC) and was treated in order with sorafenib, regorafenib and nivolumab. However, nivolumab treatment was discontinued after the 13th administration because of poor general condition. After 2 years of conservative management, follow-up computed tomography (CT) showed no definite viable tumor in the liver and no pulmonary metastatic lesions and tumor markers were not elevated. However, iron deficiency anemia (IDA) was observed. Fecal occult blood test was negative. Although further esophagogastroduodenoscopy and colonoscopy were performed, no definite cause of the gastrointestinal (GI) bleeding was identified. While prescribing iron supplements, we performed follow-up examinations. Six months later, follow-up abdominal CT showed polypoid enhancing masses in the distal ileum (Fig. 1). There was no viable intrahepatic lesion. Laboratory results showed IDA and elevated protein induced by vitamin K absence or antagonist-II level (90.8 mAU/mL). The patient denied melena. Polypoid lesions were not detected on colonoscopy and video capsule endoscopy. Three months later, the patient visited the emergency room complaining of nausea, vomiting and abdominal pain. The AFP level was 1.9 ng/mL and PIVKA-II level was 98.7 mAU/mL. An abdominal CT scan showed polypoid enhancing masses in the distal ileum at intussuscipiens, suggesting intussusception of the ileum with a lead point (Fig. 2). Segmental small bowel resection and endto end anastomosis were performed. The histological findings were consistent with those of metastatic HCC (Fig. 3). Small bowel intussusception in adult due to metastasis from HCC is extremely rare. To date, only four cases have been reported. Two cases were diagnosed with HCC metastasis to the small bowel manifesting as intussusception, and one case was diagnosed with double-balloon enteroscopy, and the other case was diagnosed with 11C-Acetate PET/CT. Our case was a small bowel metastasis of HCC manifested as obscure-occult GI bleeding, resulting in intussusception. To our knowledge, this is the first report of HCC metastasis to the small bowel manifested as obscure-occult GI bleeding. Even if HCC metastasis to the small bowel is rare, if HCC patients exhibit obscure-occult GI bleeding symptoms, it should be considered.
This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 05-2023-039). Requirement for informed consent was waived after review of IRB because it was practically impossible and this study was of retrospective design.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





