


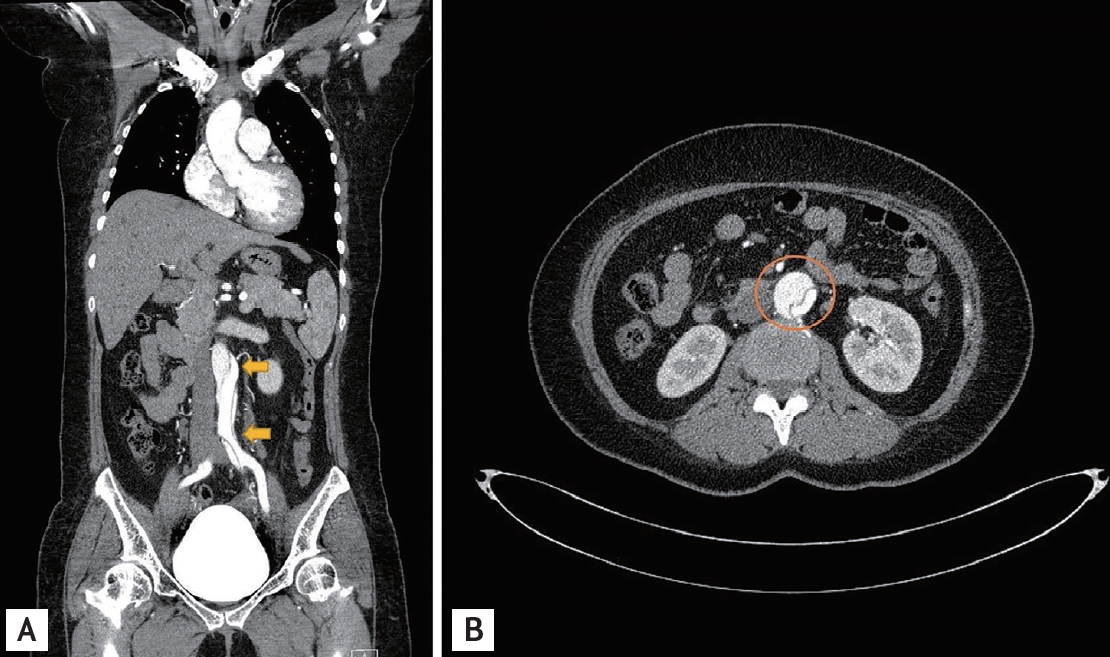
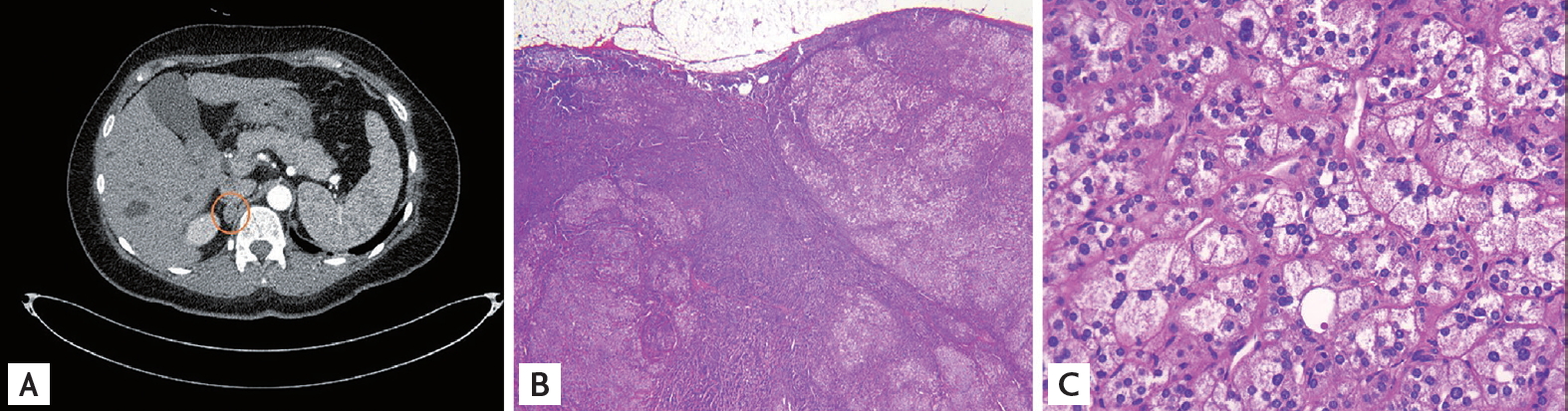
A 42-year-old woman presented to the emergency department with acute-onset severe abdominal pain. Hypertension had been diagnosed 3 years previously, which was well controlled with amlodipine 5 mg and valsartan 80 mg. On arrival, her blood pressure was 140/80 mmHg. Serum potassium was 2.3 mmol/L and arterial blood pH and HCO3 were 7.468 and 27.5 mmol/L, respectively. Electrocardiogram revealed normal sinus rhythm and left ventricular systolic function was normal on transthoracic echocardiography. Contrast-enhanced computed tomography revealed aortic dissection (Stanford type B) with dilated infra-renal abdominal aorta (Fig. 1). Additionally, a mass approximately 10 ├Ś 17 mm in size was incidentally detected in the right adrenal gland (Fig. 2A). Adrenal function tests showed: plasma renin activity 0.16 ng/mL/hr, aldosterone 17.7 ng/dL, aldosterone:renin ratio 110 (< 30). Saline infusion test was performed and aldosterone level after infusion was 29.7 (< 10) ng/dL. The patient was diagnosed with primary hyperaldosteronism (PA) caused by adrenal adenoma. After adenoma removal, serum potassium normalized and blood pressure was well controlled despite reduction in antihypertensives. Adrenal adenoma was confirmed by histopathology (Fig. 2B and 2C). Hypertension and atherosclerosis remain the commonest predisposing factors for dissecting aortic aneurysm. Therefore, it is most frequently seen between the 5th and 7th decades following longstanding degenerative hypertensive changes. Previously, PA was considered a rare cause of secondary hypertension. However, recent developments in diagnostic tests have revealed a higher incidence than previously thought. Moreover, recent studies have demonstrated possible vasculotoxic effects of hyperaldosteronism on arterial structure, with remodeling, fibrosis, proliferation, and modification of the collagen and elastin content, independent of the blood pressure. Following accurate diagnosis, surgical resection of an adenoma or medical treatment with an aldosterone antagonist for bilateral adrenal hyperplasia can lead to favorable clinical outcomes. From our experience, it is reasonable to consider PA as a possible cause of aortic dissection.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |