


INTRODUCTION
A decreased glomerular filtration rate (GFR) is an important risk factor for coronary heart disease (CHD) [1]. Traditional risk factors for cardiovascular diseases, such as diabetes mellitus, hypertension, dyslipidemia, a history of smoking, and old age, are seen frequently in patients with renal dysfunction [1, 2, 3]. In addition, specific circumstances in patients with renal dysfunction might lead to an increased risk of cardiovascular disease, including the retention of uremic toxins, impaired bone mineral (e.g., calcium) metabolism, chronic anemia, and the impaired clearance of some cytokines [4,5]. A lower GFR and increased proteinuria increase the risk of cardiovascular disease and death, and many studies have shown a relationship between decreased renal function and an increased incidence of cardiovascular events in patients with conventional risk factors for cardiovascular disease, such as diabetes mellitus, hypertension, and preexisting cardiovascular disease [6, 7, 8].
GFR is an independent risk factor for multivessel (MV) disease [9], and a baseline serum creatinine > 1.5 mg/dL in males and 1.3 mg/dL in females were a strong predictor of poor outcome after percutaneous coronary intervention (PCI) in 6,542 patients [10]. Another report demonstrated that patients with chronic kidney disease (CKD) had an increased frequency of in-hospital deaths, cardiogenic shock, recurrent hospitalization, and subsequent coronary artery bypass after the first revascularization of their coronary arteries [11]. An additional study demonstrated that the benefit of coronary revascularization exceeded the risk for renal failure as a result of the intervention [12]; however, the superiority or inferiority of infarct-related artery (IRA)-only revascularization compared with MV revascularization was not demonstrated.
A recent comprehensive meta-analysis of 14 studies revealed no difference in the primary endpoint (death, myocardial infarction [MI], or revascularization) between IRA-only revascularization and MV revascularization in patients with ST-segment elevation myocardial infarction (STEMI), without considering their renal function [13].
The aim of the present study was to evaluate the safety and effectiveness of PCI in patients with acute MI and renal insufficiency, particularly in those with MV disease who are likely to have a higher risk of developing complications after PCI, other major adverse cardiac events (MACE), and requiring repeated PCI.
METHODS
Population
From 2008 to 2011 we enrolled 16,383 patients registered in the Korea Working Group on Myocardial Infarction (KorMI). KorMI is a prospective, multicenter, observational study performed to evaluate treatment practices and outcomes in patients with acute MI around Korea with the support of the Korean Circulation Society. Among the 16,383 patients, 1,207 patients who had renal insufficiency at presentation (GFR < 60 mL/min/m2) and were diagnosed as MI with MV disease were selected. Of these, 176 individuals who did not undergo IRA revascularization were excluded. The remaining patients were divided into two groups: the IRA-only revascularization group (IRA group; patients who underwent revascularization of the IRA, but not all of the stenosed coronary arteries) and the MV revascularization group (MV group; individuals who underwent MV revascularization, including both staged MV PCI and one-stage MV PCI). The mean duration of follow-up was 327.1 ┬▒ 105.0 days.
Definitions
The diagnosis of MI was based upon the 2012 European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation (ESC/ACCF/AHA/WHF) diagnostic criteria for acute MI [14]. Renal function was measured by estimating GFR using the CKD epidemiology collaboration equation [15]. Patients were regarded as having renal insufficiency when they had an estimated glomerular filtration rate (eGFR) < 60 mL/min/m2 at presentation.
MV disease was defined when a coronary angiography (CAG) showed that two or more coronary arteries were stenosed > 50%. IRA-only revascularization was defined as revascularization of only one culprit coronary artery in MV disease during the patient's initial hospitalization, whereas MV revascularization was defined as the revascularization of two or more coronary arteries during hospitalization. A successful PCI was defined as a thrombolysis in myocardial infarction (TIMI) flow of three with residual stenosis < 50% in the IRA. The type of coronary arterial lesion was determined according to the American College of Cardiology/AHA classification.
When the complications after PCI were defined, a cerebrovascular incident was defined as a newly developed neurological disorder with evidence of brain damage. New-onset heart failure was defined as dyspnea of newly developed New York Heart Association class III/IV, orthopnea, rales, elevated jugular venous pressure, or pulmonary congestion on chest X-ray, which were all considered to be related to decreased cardiac function. Coronary arterial injury was defined as a composite of any unintended damage to the coronary arteries during CAG, such as perforation and distal embolization. Major bleeding was defined as bleeding from the body with an drop of hematocrit more than 15%, intracranial bleeding, fatal bleeding, any bleeding that needed surgery or transfusion, or any other bleeding that was regarded as clinically significant, as judged by the investigator. Recurrent ischemia was defined as recurrent symptoms with elevated cardiac markers more than twice the upper limit of the normal range, or newly developed electrocardiographic changes that were compatible with myocardial ischemia. Peripheral arterial complications were defined as a composite of any unintended damage to the peripheral arteries during CAG, such as hematomas or pseudoaneurysms.
Coronary angiography
Baseline data for the study population were collected before CAG, including age, gender, past history including conventional risk factors for CHD, baseline two-dimensional echocardiographic data, baseline laboratory data, and vital signs. Data were collected mostly from clinician's records and the results of in-hospital examinations. CAG was performed after the administration of heparin via a transradial or transfemoral approach. All patients received proper medical treatment before and after CAG, including 100 to 300 mg of aspirin and 300 to 600 mg of clopidogrel before PCI. An additional dose of heparin was administered to maintain the activated clotting time > 250 seconds as needed. When MV disease was noted, the operator of each CAG decided to perform IRA-only revascularization or MV revascularization according to the clinical circumstances. Additional medical therapies were administered to each patient as required. In addition, information regarding the involved coronary arteries (IRA and non-IRAs), strategy of revascularization, medications were collected from the angiographic data.
Clinical endpoints
After CAG, any incidence of complications related to the PCI, including cerebrovascular events, newly developed heart failure, cardiogenic shock, coronary arterial injuries, recurred ischemia, major arrhythmic events (ventricular tachycardia, ventricular fibrillation, atrioventricular block, atrial fibrillation), major bleeding, and peripheral arterial complications, was recorded for patients in each group. We also analyzed the cumulative data for MACE during the follow-up period as the clinical outcomes. MACE included death of cardiac origin, non-fatal MI, repeated PCI, and the need for a coronary artery bypass graft. Incidences of repeated PCI were categorized into three subgroups: target lesion revascularization (TLR; repeated PCI for re-stenosed, previously re-vascularized segments, and adjacent segments within 5 mm of the original lesion), target vessel revascularization (TVR; repeated PCI for the stenosed segment of same coronary artery but not the original lesion), and non-TVR (repeated PCI for another coronary artery, but not the original lesion).
Statistical analysis
The SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. All numerical variables (e.g., age and laboratory data) are presented as means ┬▒ standard deviations, whereas all categorical variables are shown as numbers and percentages. Comparisons between the two groups (IRA vs. MV) were made using independent samples t tests for numerical variables, and chi-square tests or Fisher exact tests for categorical variables. Multiple logistic regression analysis was performed after controlling for factors that showed significant differences at baseline between the two groups to determine whether these factors influenced the clinical end points. In addition, a propensity score-matched model was used to reduce the effect of different baseline characteristics. Kaplan-Meier survival curves were used to compare the incidence of MACEs. All of the tests were two-tailed, and p < 0.05 were considered to indicate statistical significance.
RESULTS
Baseline characteristics
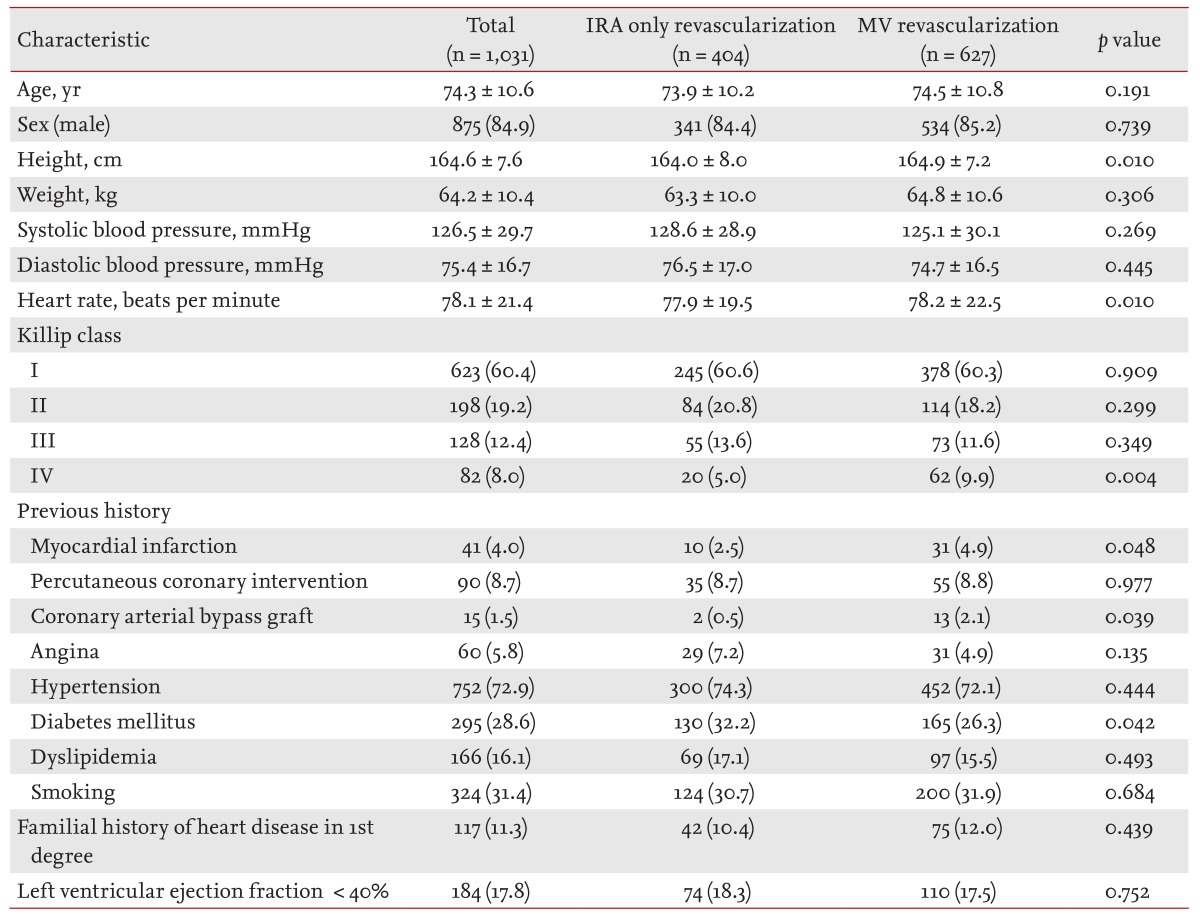
There were no significant differences in age, gender distribution, and weight between the groups. Patients in the IRA group were slightly taller, but the difference was small. Regarding vital signs, blood pressure was not significantly different between the two groups, and differences in heart rate were also small. However, more patients in the MV group presented with cardiogenic shock (Killip class IV) when they visited the hospital compared with the IRA group. There were no significant differences in the prevalence of underlying diseases (previous history of PCI, angina, hypertension, dyslipidemia, smoking, and first-degree heart disease), but history of MI was more common in the MV group, whereas DM was more frequent in the IRA group (Table 1).
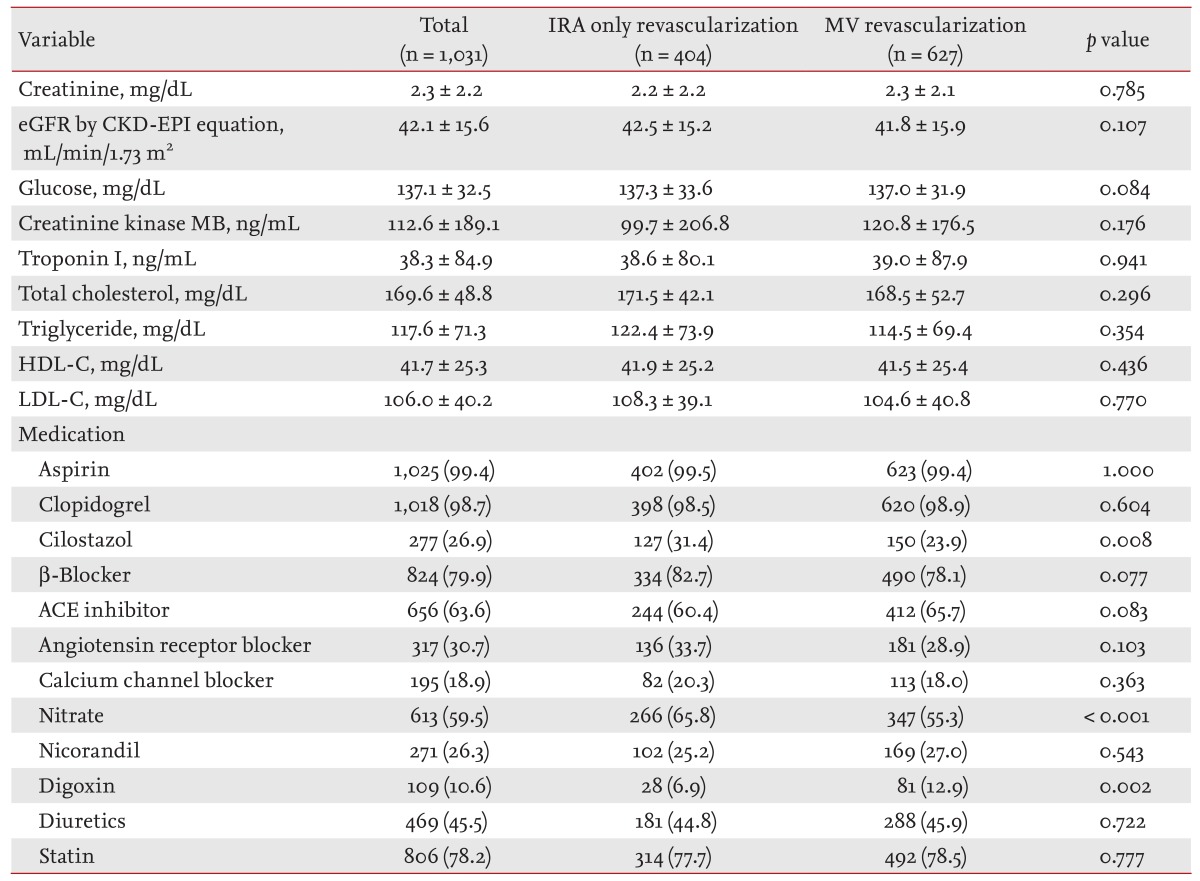
The mean serum creatinine levels were 2.3 ┬▒ 2.2 mg/dL, and there was no significant difference between the two groups. eGFR was also comparable between the two groups. The results of other baseline examinations (serum glucose, creatinine kinase MB, troponin I, total cholesterol, triglycerides, high density lipoprotein cholesterol, low density lipoprotein cholesterol, and the proportion of patients with ischemic heart failure) were also comparable between the groups. Regarding initial medications, nearly all patients in both groups received dual antiplatelet therapy (aspirin and clopidogrel); however, cilostazol and nitrates were given more frequently in the IRA group, whereas digoxin was prescribed more frequently in the MV group (Table 2).
Coronary angiographic findings
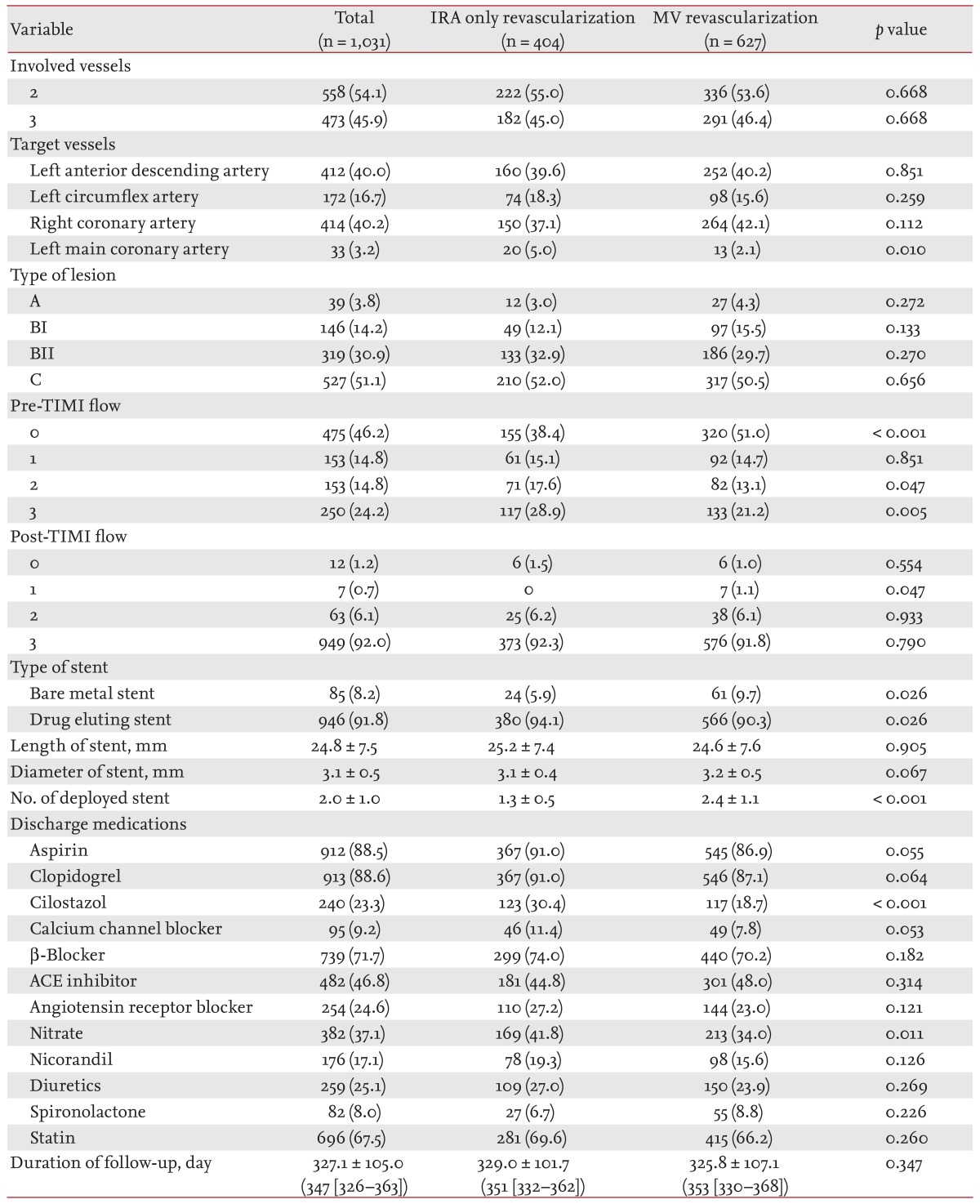
The prevalence of two- and three-vessel disease was not different between the two groups. The distribution of IRA and the type of culprit lesion did not differ, except for left main coronary artery disease, which was more common in the IRA group. Pre-interventional coronary arterial flow was worse in the MV group, as reflected by a higher proportion of pre-TIMI flow 0 and a lower proportion of pre-TIMI flow 3. However, the success rate of PCI did not differ (Table 3).
There were no significant differences in the length and diameter of the deployed stents between the two groups; however, bare metal stents were used more frequently and more total stents were used in the MV group. The medications at the time of discharge and during hospitalization were mostly not different between the two groups; however, cilostazol and nitrates were given more frequently in the IRA group, just as they were in the initial medications (Table 2). After discharge, patients were followed for a mean duration of 327.1 ┬▒ 105.0 days (Table 3).
Complications after PCI
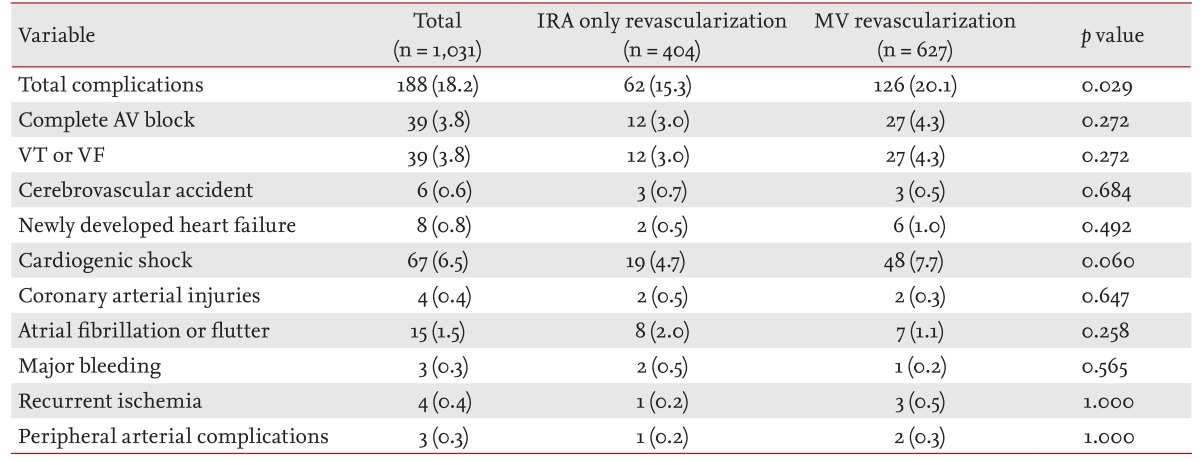
There were no significant differences in the rates of complications between the two groups, although the incidence of each complication tended to be higher in the MV group. However, when considered all together, complications occurred more frequently in the MV group (Table 4).
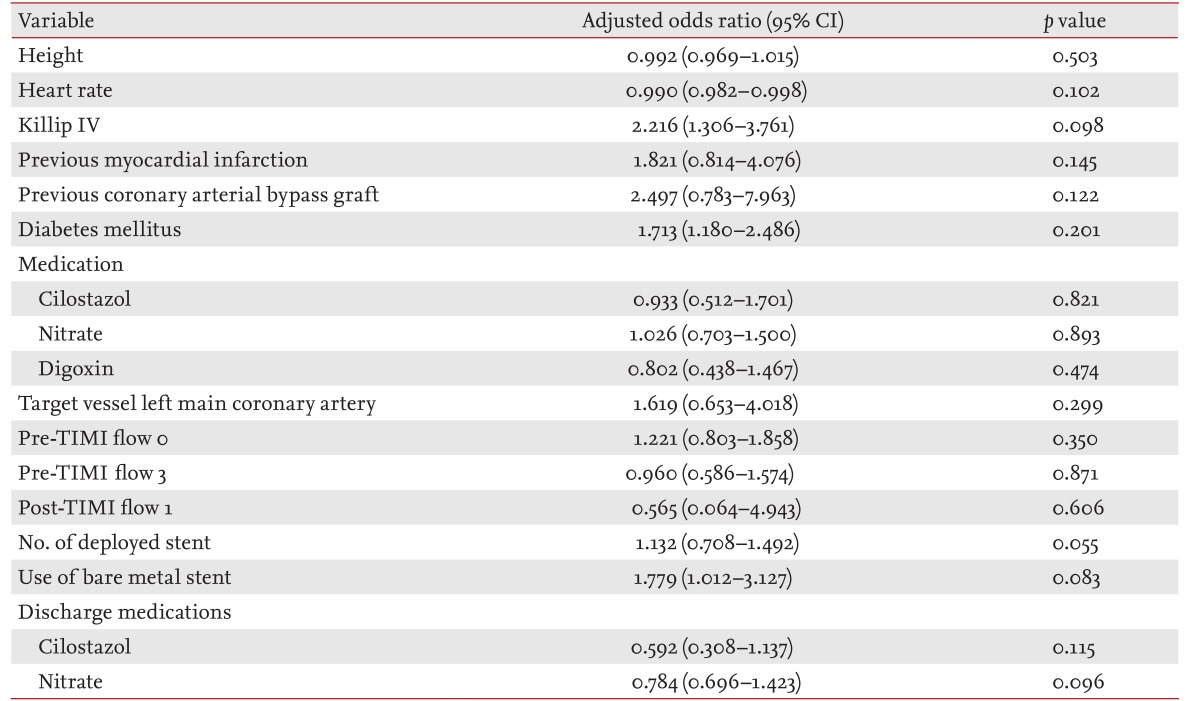
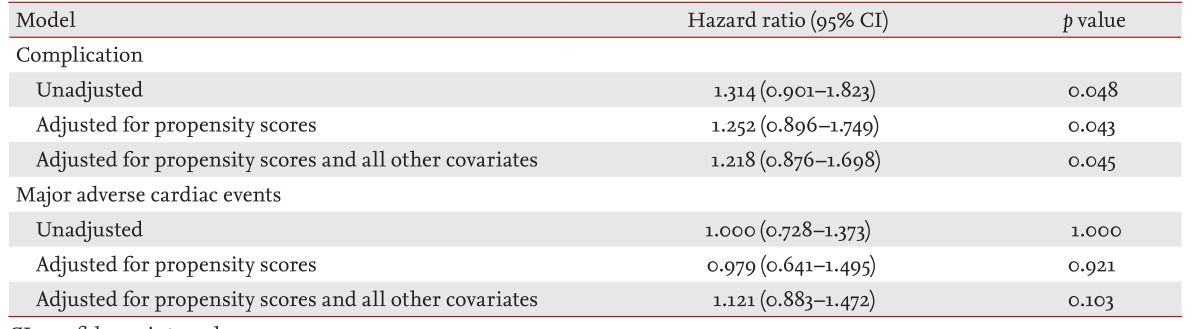
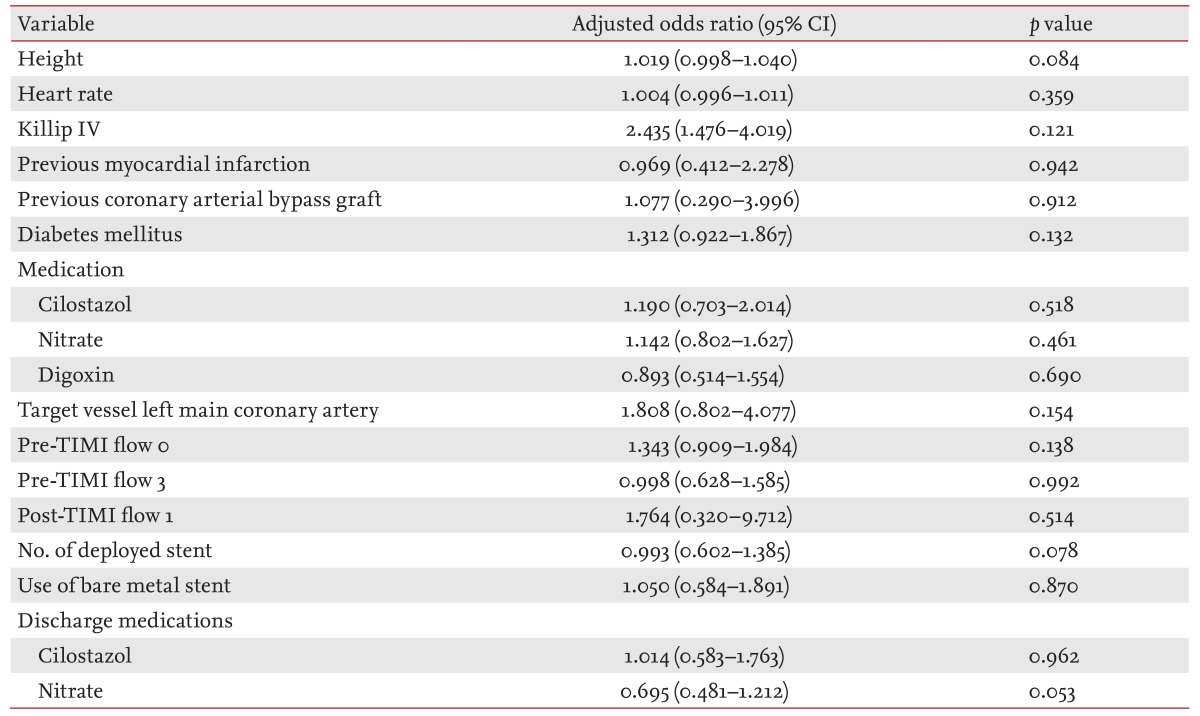
Because there were significant differences in some baseline characteristics, we next performed multivariate logistic regression analysis after controlling for individual factors (height, heart rate, Killip class IV, previous history of MI, coronary arterial bypass graft, diabetes mellitus, in-hospital administration of cilostazol, nitrates, and digoxin, the left main coronary artery as a target vessel, pre-TIMI flow 0 and 3, post-TIMI flow 1, the number and type of stent used, and the administration of cilostazol and nitrate at the time of discharge). The results revealed that none of these were significant risk factors for an increased incidence of complications after PCI (Table 5). When the two groups were compared among propensity-matched patients, MV revascularization was a significant risk factor for complications after PCI (Table 6).
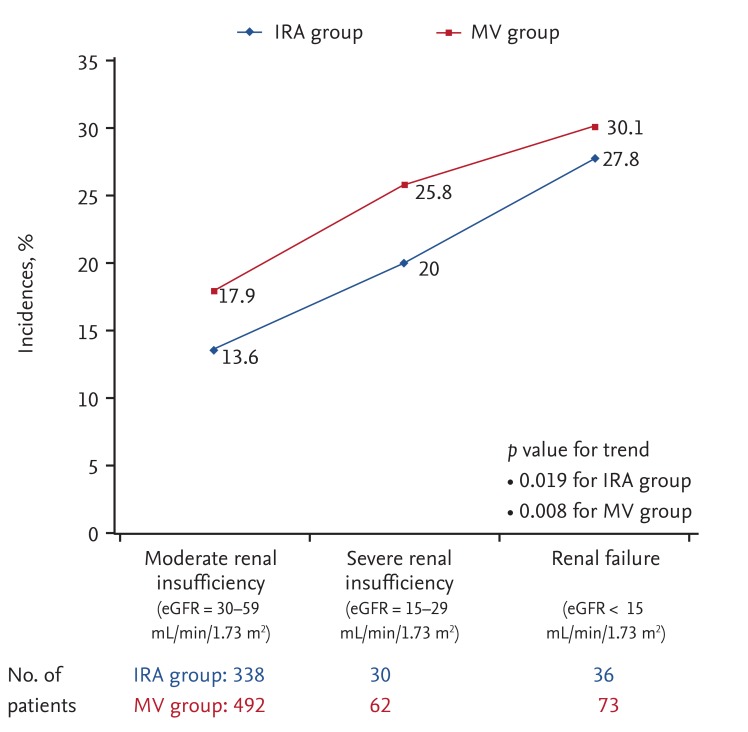
To define whether there is a relationship between renal function and the incidence of complications, the target population was divided into three groups according to eGFR. There was a negative correlation between eGFR and the incidence of complications in each group (Fig. 1).
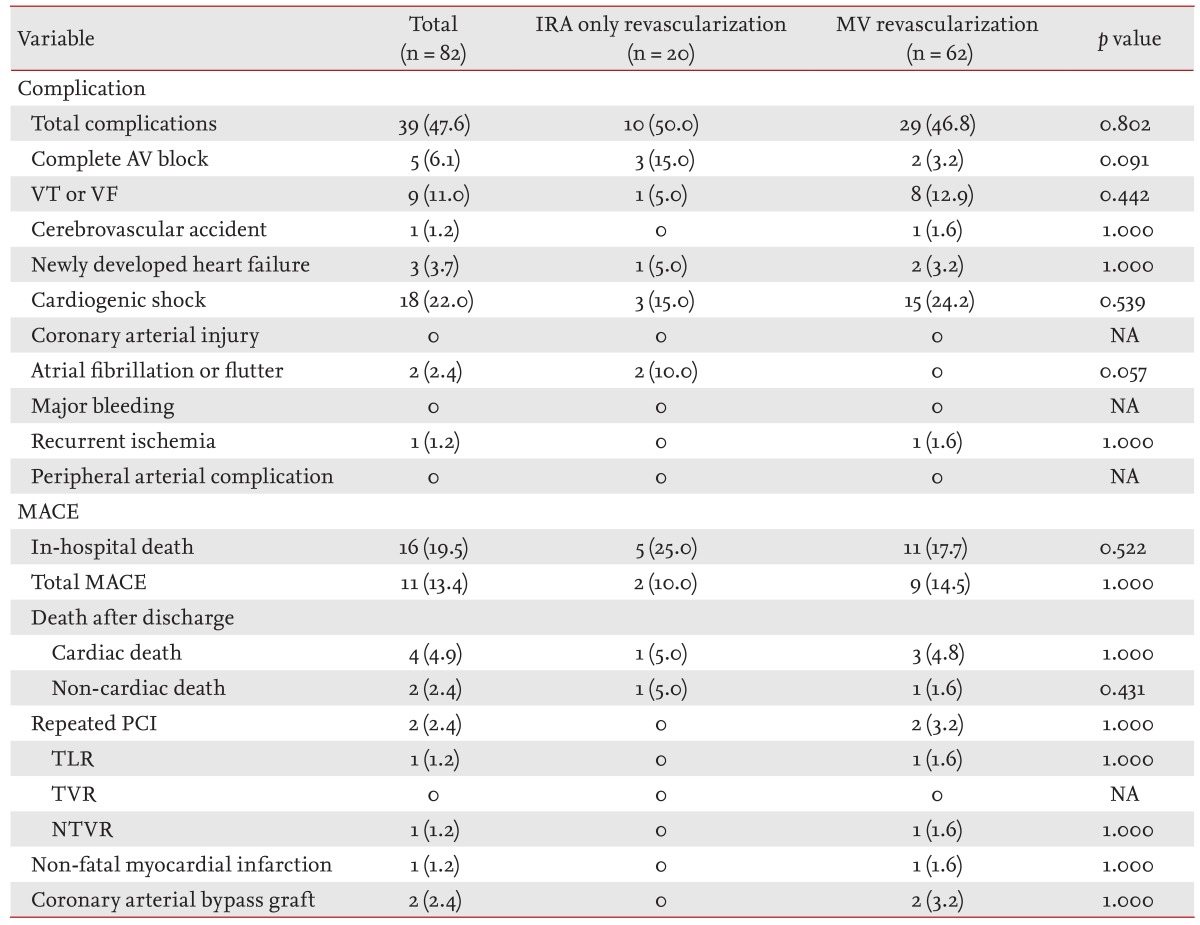
Because patients in the MV group presented more frequently with cardiogenic shock at the time of admission, it could be hypothesized that physicians preferred MV revascularization when a patient exhibited hemodynamic instability, despite the risk of complications after PCI [16]. Therefore, we next analyzed the subgroup of patients who presented with cardiogenic shock (Killip class IV). The incidence of complications tended to be higher in this population compared with the entire patient cohort, but there were no significant differences between the IRA and MV groups (Table 7).
Incidence of major adverse cardiac events
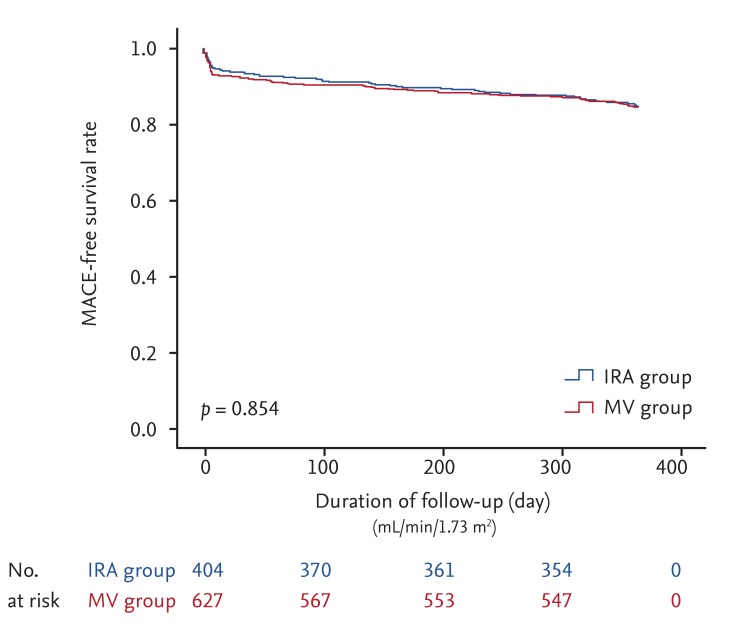
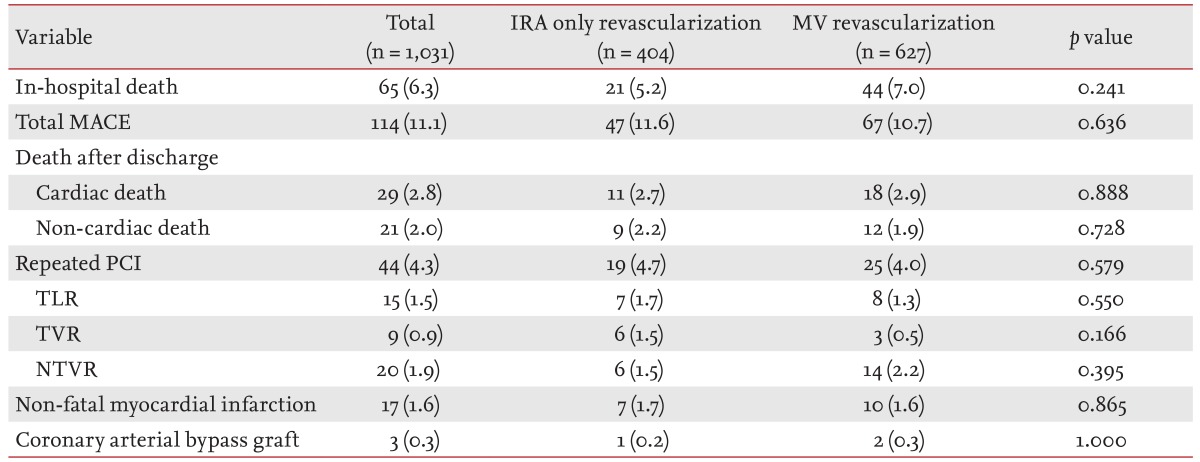
There was a significant difference in the incidence of total complications, the in-hospital death rate, and the cumulative incidence of MACE during a mean follow-up period of 12 months between the two groups. Consistently with this, a Kaplan-Meier curve for 12-month MACE-free survival showed no significant differences between the groups (Fig. 2). Similarly, there was no difference in the incidence of each individual MACE during 12-month follow-up. For patients who needed a repeat PCI, the re-infarction rate of the target vessel, reflected by the incidence of TLR and TVR, or non-target vessel did not differ between the two groups (Table 8).
We also performed multivariate logistic regression analysis after controlling for factors that showed significant differences at baseline between the IRA group and the MV group. Similar to the above results, none of the factors increased the incidence of MACE significantly (Table 9). In addition, similar results were obtained in a comparison of propensity-matched patients between the two groups (Table 6).
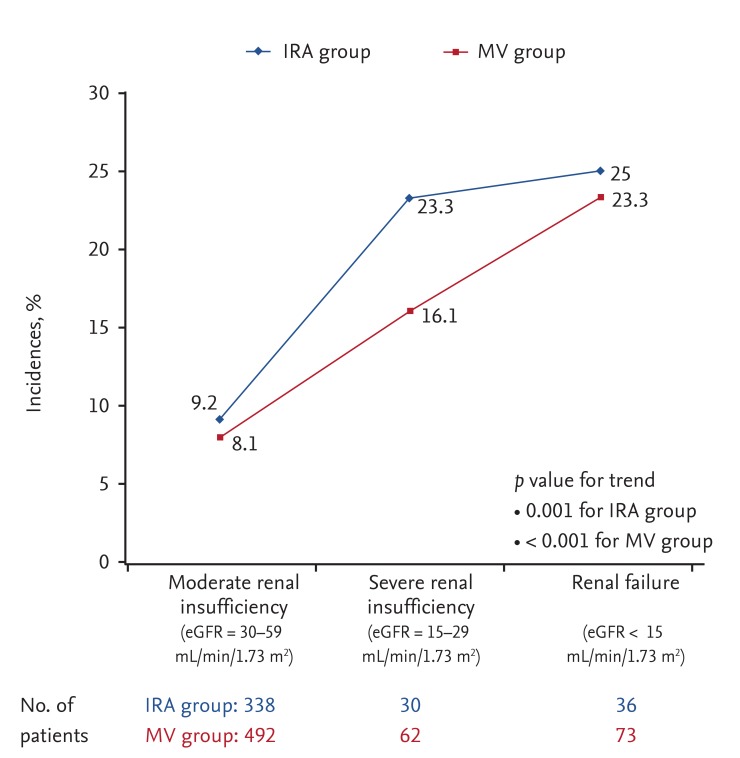
When patients were divided into three groups according to their eGFR to define whether there is a relationship between renal function and the incidence of MACE, there was a negative correlation between eGFR and the incidence of MACE in each group (Fig. 3).
Finally, patients who experienced cardiogenic shock at presentation were analyzed. Similar to the above findings, the 12-month MACE rate was higher in patients with cardiogenic shock than the rest of the enrolled patients, but there were no significant differences between the two groups (Table 7).
DISCUSSION
The results of the current study showed that MV revascularization did not reduce the 12-month MACE rate, including repeated PCI. Furthermore, it was associated with a significantly higher incidence of complications after PCI, consistently with previous studies that did not consider renal function [17, 18, 19, 20]. The current study provides novel insight because it considered only patients with impaired renal function using the results of PCI performed by a variety of cardiologists in many medical centers around Korea. MV disease is present in 40% to 65% of patients presenting with STEMI who undergo primary PCI, and is associated with adverse prognosis [21, 22]. The 2013 ACCF-AHA guidelines for STEMI recommend that PCI should be performed in a non-infarct artery at a time of separate from primary PCI in patients who have spontaneous symptoms of myocardial ischemia as a class I indication, and in patients with intermediate- or high-risk findings on noninvasive testing as a class IIa indication [23]. Consistently with these recommendations, Hannan et al. [24] compared 538 patients undergoing staged MV PCI within 60 days of primary PCI with propensity-matched individuals who underwent IRA-only revascularization, and the results showed that MV revascularization was associated with a lower mortality rate at 1 year (1.3% in MV revascularization vs. 3.3% in IRA-only revascularization, p = 0.04). However, many studies that compared the benefits and risks of IRA-only revascularization and MV revascularization were non-randomized, and few studies have targeted patients with renal insufficiency.
Narrowing of arterial lumen in patients with renal insufficiency, particularly CKD, is highly complex, and these patients exhibit different pathogenic processes than do individuals with normal renal function; therefore, some "beneficial" treatments have no definite clinical benefit, similar to statins in individuals with end-stage renal disease [25, 26, 27]. In the current results, worse renal function was strongly correlated with worse prognosis, as reflected in incidence of MACE, although it was also correlated with higher complication rates after PCI. Together with other difficulties related to medical treatment (uncontrolled blood pressure, difficulties adjusting levels of serum electrolytes, etc.) physicians fear medical treatment failure and want to secure the patency of the coronary arteries using PCI whenever possible. In addition, one prior study that assessed the different outcomes with IRA-only revascularization and MV revascularization based on Korean Acute Myocardial Infarction Registry (KAMIR, a prior version of KorMI) demonstrated that MV revascularization had protective effects for repeated PCI in non-target vessels, regardless of renal function. The authors suggested that MV revascularization allows a more complete treatment of other potentially unstable plaques that are formed by inflammatory reactions involving not only the culprit lesion but also the entire coronary tree [28, 29]. However, the current study showed different results; no beneficial effect of MV revasculariztion, although when we analyzed our entire population set (n = 16,383), regardless of their renal function, we found similar propensity as the previous study we described above (data not shown).
The observation that more complications occurred in the MV group suggests that more manipulation of the coronary arteries and increased mechanical revascularization do not guarantee a better in-hospital outcome. However, the finding that the 12-month cumulative incidence of MACE was comparable between the two groups, suggests that complications might be overcome using intensive post-PCI care without causing long-term complications.
Study limitations
If data regarding the elapsed time and dose of contrast media used during CAG were available, we might be able to better understand the relationship between these parameters and the incidence of complications; however, this information was unavailable. In addition, we were able to only assess patients' baseline renal function, but follow-up renal function; therefore, the data did not differentiate patients with only acute kidney injury from those with CKD.
In some cases at one medical center that participated in KorMI (the authors' institution), the reasons for MV revascularization rather than IRA-only revascularization were as follows: persistent symptoms after IRA-only revascularization, and lack of full recovery from hemodynamic instability after the first PCI. In contrast, IRA-only revascularization was preferred in other cases in which the lesion in a non-IRA vessel caused a chronic total occlusion with rich collateral flow that did not lead to a clinical problem. However, the choice of IRA-only revascularization or MV revascularization was made according to individual circumstances; therefore, cases could not be sorted concisely.
MV revascularization is defined as revascularization of two or more coronary arteries during index hospitalization. Since it consists of both one-staged MV revascularization and multiple-staged MV revascularization during one index hospitalization, some parts of MV group can be considered as 'early repeated PCI.'
In conclusion, despite the limitations to this study mentioned above, mainly due to its retrospective nature, these results suggest that MV revascularization is not superior to IRA-only revascularization in patients that presented with acute MI with MV disease and renal insufficiency because of the higher risk of complications after PCI and equivalent outcomes after PCI.
KEY MESSAGE
Multivessel (MV) revascularization failed to show better clinical outcome compared with infarct-related artery (IRA)-only revascularization in patients with acute myocardial infarction (MI) with MV disease and renal insufficiency.
MV revascularization was associated with higher complication rates than IRA-only revascularization in patients with acute MI with MV disease and renal insufficiency.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





