


INTRODUCTION
The stomach and esophagus may be the origin of chest pain that's clinically indistinguishable from the pain of myocardial ischemia. About 20% to 39% of patients who undergo coronary angiography to investigate their chest pain are found to have normal coronary arteries1). If these patients were to be diagnosed with microvascular angina or cardiac syndrome X from the positive results of the cardiac stress tests, it would be confusing as to whether the real cause of the chest pain originated from cardiac disease or from other causes. The aim of this study was to clarify the identification of gastro-esophageal diseases in the patients with typical chest pain and who have a normal coronary angiogram.
MATERIALS AND METHODS
We retrospectively studied all the consecutive patients who were referred for routine evaluation of their ischemic heart disease at Keimyung Univeristy, Dongsan Medial Center, Daegu, Korea, from January 2001 to June 2004; these patients all had typical chest pain, a normal coronary angiogram and they underwent gastro-esophageal studies; upper endoscopy, Bernstein's test and esophageal manometry. A total of 121 patients (mean age: 56.0┬▒8.9 years, age range: 34 to 76; 42 males) were enrolled into this study.
RESULTS
Of the total 121 patients, 107 (88.4%) of them clinically presented with stable angina. Cardiac stress testing was performed in 82 (67.8%) of the 121 patients, and this testing included an exercise electrocardiogram, a stress echocardiogram or a radionuclide myocardial scan. Positive ischemic results were observed in 52 (63.4%) of the 82 patients. The coronary angiographic results were normal in all the enrolled patients and we had to perform three gastro-esophageal studies in order to find a possible clinical clue as to the cause of the chest pain.
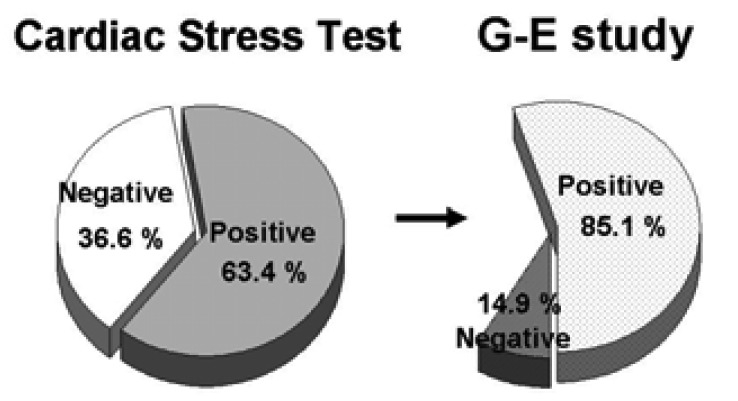
The results of the upper endoscopy studies were normal in 77 patients (63.8%); 18 patients (14.8%) had erosive gastritis and 16 patients (13.2%) had reflux esophagitis according to the Los Angeles classifciation2). Gastric ulcer was found in 4 patients (3.3%) and duodenal ulcer was found in 5 (4.1%). One case with stomach cancer was detected during the endoscopy. Thus, 36.2% of all the patients exhibited abnormal findings on the upper endoscopy. The esophageal provocation test used in this study was the acid perfusion test, as has been described by Bernstein and Baker3). The test results were considered positive only if two repeated infusions evoked pain. Positive results were observed for 68 patients (56.2%). In 59 (86.8%) of those 68 patients in which non-erosive reflux disease was noted, the upper endoscopy showed a normal gastro-esophageal junction. Esophageal motility monitoring was performed using stationary manometry (Synectics Medical AB, Sweden). The catheter was inserted into the patient's nose and placed into the esophagus. The results of the esophageal manometry were normal in 86 patients. A nutcracker esophagus was defined as having a high amplitude contraction in which the diagnostic threshold was more than 160 mmHg over a 6 second duration4). According to this criterion, 27 patients (22.3%) were diagnosed with nutcracker esophagus. A hypertensive lower esophageal sphincter was defined as having a lower esophageal sphincter tone of more than 45 mmHg: this was observed in 3 patients (2.5%). The other abnormal results of the manometric findings were described as being non-specific esophageal motility disorders and these were observed in 5 (4.1%) patients (Figure 1). At least one abnormal result out of the three gastro-esophageal studies was observed in 103 (84.9%) of all the patients we analyzed. Among the 52 patients who exhibited positive results on the cardiac stress test, 46 (85.1%) patients had more than one abnormal finding on the gastro-esophageal studies (Figure 2).
DISCUSSION
Due to the recent rapid advancement in cardiovascular procedures such as pressure wires, Doppler guidewires, intravascular ultrasound, optical coherence tomography and etc., many cardiologists aggressively perform functional and/or imaging studies to determine the cardiac cause of the chest pain for patients with normal coronary angiograms. Those expensive studies are frequently found to be of no value at all. Of those patients who present in ambulatory care for the first time with chest pain, a cardiac etiology is ultimately found in only 11% to 39%5, 6). Many of the non-cardiac origins of chest pain have been studied, and it's certain that gastro-esophageal disease can not always explain the cause of chest pain in the patients with a normal coronary angiogram. However, before performing any invasive cardiac studies, consideration should be given that the chest pain might originate from a non-cardiac cause, and such causes as gastro-esophageal disease or psychiatric disorders should be taken into account.
Several types of esophageal diseases like nonspecific esophageal motility disorder and diffuse esophageal spasm have not recently been accepted as causes of angina-like chest pain7). Our study had a limitation similar to the previous reports in that not all the patients who had a normal coronary angiogram underwent those three studies that were mentioned about. We could not exclude that a selection bias occurred in this study. According to the prescribed limitations, our data might have overestimated the incidence of gastro-esophageal disease. However, the 52 patients who had positive results on the cardiac stress test with a normal coronary angiogram had symptoms that clinically corresponded to microvascular angina or cardiac syndrome X8, 9). When the patients were diagnosed with those two diseases, antianginal medications such as calcium channel blockers, beta-blockers, nitrates or antidepressants like imipramine were used10). Unfortunately, the response to those regimens up till now has been rather disappointing. We believed that this poor response might be related to misdiagnosis of the real mechanism of the chest pain. Thus, before making those diagnoses, other studies should be performed to rule out the various diseases that could be causing the chest pain. In our presented data, 46 (85.1%) of 52 patients had abnormal findings from the cardiac stress test and the gastro-esophageal studies. Those overlapping results mean that the chest pain could have originated from multiple causes, or the chest pain might have been an innocent bystander, regardless of the positive results on both tests. Thus, careful clinical follow-up and correlating the symptoms to the medical management should be performed. According to our study, in spite of any existing evidence of microvascular angina or cardiac syndrome X, it would be more advisable to perform gastro-esophageal studies to adequately manage the patients who present with chest pain.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





