


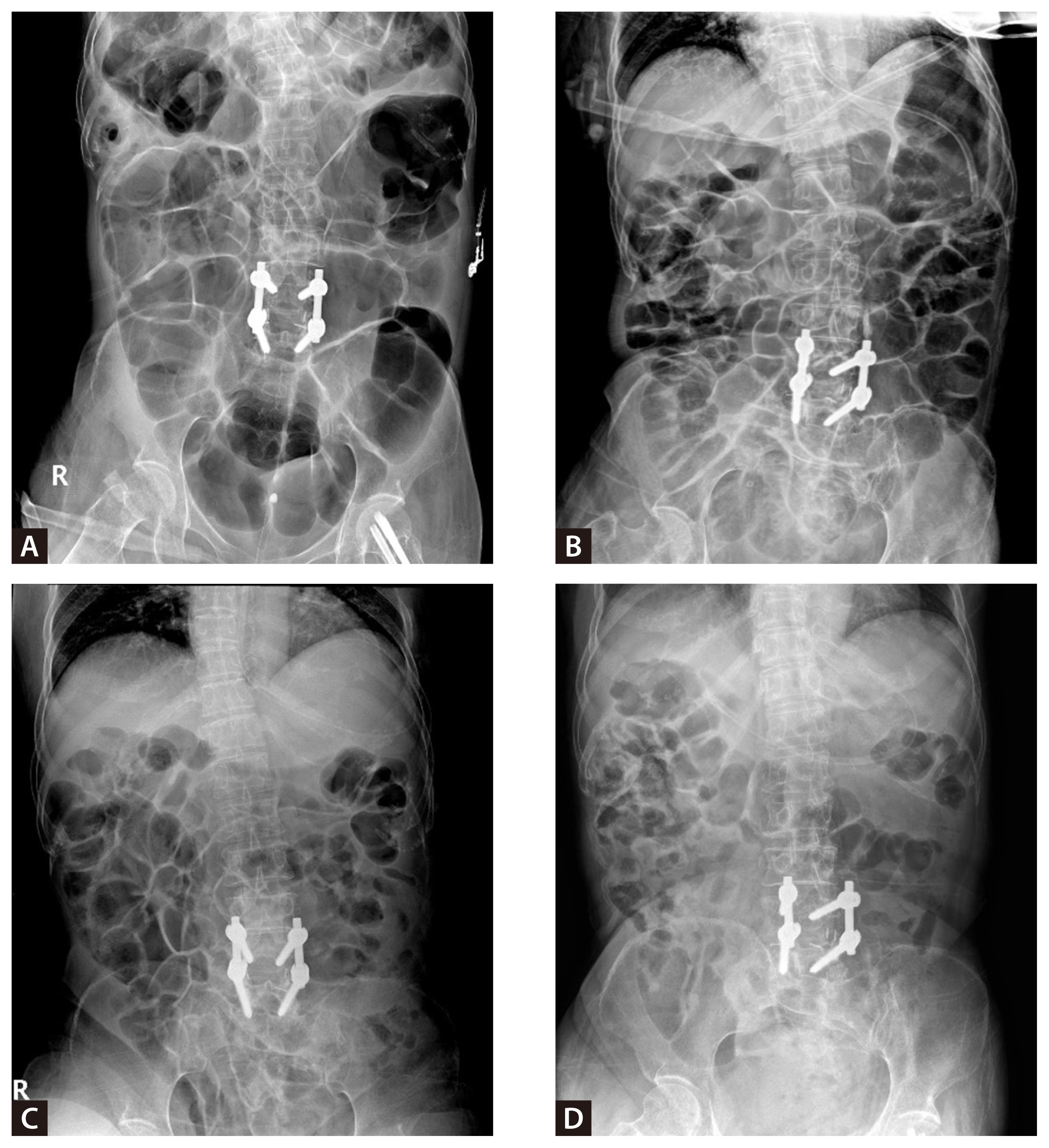
A 59-year-old, chronically bedbound woman with cerebral palsy was admitted to a long-term care facility with fever and abdominal distension. Examination revealed marked abdominal distension without peritoneal signs, and imaging revealed severe diffuse colonic distension without mechanical obstruction (Fig. 1A). Conservative management included bowel rest, rectal and nasogastric decompression, and intravenous fluid and metoclopramide administration. Empiric metronidazole for suspected Clostridioides difficile was discontinued after a negative assay, whereas piperacillin-tazobactam was administered for urinary tract infection (days 3–10).
Despite five days of therapy, there was no clinical or radiographic improvement; tense distension and decreased bowel sounds persisted, with serial radiographs showing diffuse dilatation consistent with colonic pseudo-obstruction (Fig. 1B). After ≥72 hours of failed conservative therapy, fecal microbiota transplantation (FMT) was performed on day 6. Bowel preparation was not feasible because of severe colonic distention despite rectal enema attempts. To optimize luminal distribution, FMT was administered via colonoscopy (100 mL into the transverse colon) and duodenoscopy (150 mL into the duodenum) (Fig. 2).
Clinical improvement was rapid. Bowel sounds recovered within 24 hours, allowing resumption of enteral nutrition. Normal defecation commenced within four days, allowing rectal tube removal. Follow-up radiographs demonstrated near-complete resolution of the colonic dilatation with minimal residual gas (Fig. 1D).
This case demonstrates FMT efficacy for refractory colonic pseudo-obstruction without C. difficile infection. Previous reports on acute and chronic intestinal pseudo-obstruction have suggested that FMT reduces intestinal bacterial overgrowth and improves motility [1,2] . A recent review framed colonic pseudo-obstruction as a dysbiosis-associated disorder that supports microbiome-targeted therapy [3] . Moreover, a randomized trial demonstrated that capsule FMT improved symptoms and microbial diversity compared to a placebo [4] . Overall, these findings support FMT as a promising therapeutic option if conservative measures fail to treat colonic pseudo-obstruction.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





