


A 61-year-old male was admitted to our hospital following the sudden onset of visual disturbance and hearing difficulty. He experienced an explosive chronic cough that developed after the ocular and auditory symptoms. The cough was refractory to treatment and worsened over several months.
Upon admission, his vital signs were blood pressure 130/70 mmHg, heart rate 109/min, respiratory rate 26/min, and body temperature 37.1°C. Laboratory tests revealed unremarkable serum and urine protein electrophoresis results, except erythrocyte sedimentation rate 73 mm/hr, C-reactive protein 4.27 mg/dL (reference range 0–0.5). Tests for infectious conditions, including blood, sputum, urine, and bronchial washing fluid cultures; tuberculosis interferon-gamma release assay; and serologic tests for bacterial, viral, protozoal, and parasitic agents, were all negative, except for a positive Treponema pallidum hemagglutination assay. Serologic tests for systemic autoimmune diseases and auto-antibodies were negative (Table 1).
Ocular examinations identified panuveitis excluding endophthalmitis, while auditory tests confirmed luetic sensorineural hearing loss. Despite a normal venereal disease research laboratory test, brain MRI/magnetic resonance angiography revealed only small vessel disease without other abnormalities. A cerebrospinal fluid test revealed unremarkable.
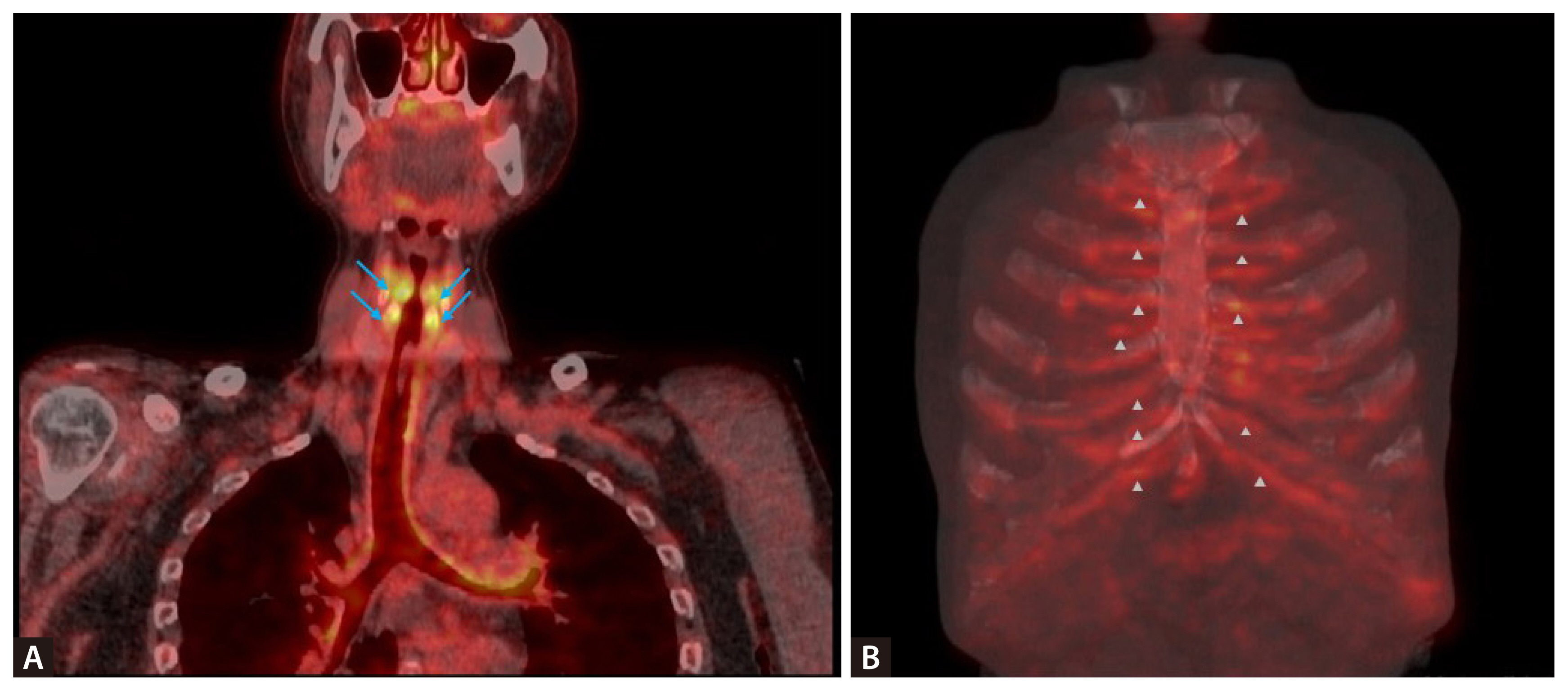
To evaluate potential underlying conditions, including lymphoproliferative diseases, malignancies, vasculopathies and hidden infection foci, a positron emission tomography-computed tomography (PET-CT) scan revealed an increased fluorine-18 fluorodeoxyglucose (18-F-FDG) uptake in costal cartilage (Fig. 1B), laryngeal cartilages (Fig. 1A), and tracheal ring cartilage (Fig. 1A), suggesting chondritis.
The patient was diagnosed with relapsing polychondritis, the underlying cause of his intractable chronic cough, alongside panuveitis/endophthalmitis and acute sensorineural hearing loss.
The patient is closely followed at the outpatient department and is currently on methotrexate 12.5 mg weekly, PD 7.5 mg daily, azathioprine 50 mg twice daily, and mycophenolate mofetil 1,000 mg twice daily.
This report details a case of relapsing polychondritis [1], a rare cause of chronic cough without nasal or ear involvement, accompanied by acute uveitis and sensorineural hearing loss.
The study was approved by the Institutional Review Board (IRB) of Yeungnam University Medical Center (IRB No: YUMC 2025-02-030). The IRB waived the requirement for written informed consent from the patient.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





