


INTRODUCTION
Adverse drug reactions (ADRs) account for 3ŌĆō6% of all hospital admissions and occur in 10ŌĆō15% of hospitalized patients, contributing to increased morbidity, prolonged hospitalization, and mortality. Most ADRs are type A reactions, whichare predictable and dose-dependent, based on the drugŌĆÖs pharmacological properties. In contrast, drug hypersensitivity reactions (DHRs) are type B reactions that are unpredictable, dose-independent, and comprise approximately 6ŌĆō10% of all ADRs [1]. Although less common, DHRs are clinically important because they can occur with minimal drug exposure, are prone to recurrence upon reexposure, and may present with severe manifestations such as anaphylaxis or severe cutaneous adverse reactions (SCARs). Therefore, early recognition and accurate diagnosis of DHRs are crucial for the management of patients with ADRs.
Several studies have examined the epidemiology of ADRs; however, many did not differentiate subtypes, such as hypersensitivity reactions, and diagnoses were often made in the emergency department (ED) without subsequent confirmation by an allergist. Consequently, the true incidence and clinical features of DHRs in real-world settings remain unclear [2]. In particular, while most medications are prescribed in outpatient settings, it is challenging to monitor adverse events that occur post-prescription, making the comprehensive evaluation of DHRs outside hospital settings challenging.
Although EDs are not dedicated outpatient settings, they can serve as important sites for the initial evaluation of drug-related adverse events that occur outside the hospital, particularly in acute presentations where temporal relationships are more apparent [3,4]. This is especially relevant when patients present soon after drug exposure, which allows clinicians to assess causality with fewer confounding factors.
Although previous studies have examined drug-related adverse events in the ED, one study focused on ADRs in general [5], while others addressed DHRs without allergist confirmation, raising concerns about diagnostic accuracy [6ŌĆō9]. Given the broad clinical spectrum of DHRs, specialized evaluation using skin tests, serum-specific immunoglobulin E (IgE) assays, or drug provocation tests are often required; otherwise, both over- and underdiagnosis may occur [10]. Referral to allergists is therefore recommended; however, no study has investigated post-ED evaluation to confirm or refine the initial diagnosis.
To address this gap, this study aimed to investigate the clinical features of DHRs identified in the ED of a university hospital in Korea. By incorporating follow-up evaluations performed by allergists, this study sought to improve the diagnostic accuracy and provide a more comprehensive understanding of drug hypersensitivity in real-world practice.
METHODS
Study design and case selection
This retrospective study used data from the Voluntary Adverse Drug Reaction Reporting System at Hallym University Dongtan Sacred Heart Hospital in Hwaseong, South Korea. This institutional system enables spontaneous reporting of suspected ADRs via an electronic case report form (e-CRF). Two allergy specialists (Choi and Chung) reviewed all reports of ADRs submitted by the ED over three years (January 2021 to December 2023).
Among these, only cases with a causal relationship categorized as possible, probable, or certain according to the World Health OrganizationŌĆōUppsala Monitoring Centre criteria were included in the analysis [11].
All drug hypersensitivity cases reported during the study period were included, and a priori sample size calculation was not applicable. Data on demographics, clinical manifestations, causative drugs, reaction severity, ED management, and follow-up visits to allergy specialists were collected retrospectively using the e-CRF and the hospitalŌĆÖs electronic medical records. Patients with missing or incomplete data were excluded from analyses requiring relevant information, and no data imputation was performed.
This study was approved by the Institutional Review Board of Hallym University Dongtan Sacred Heart Hospital (IRB no. HDT 2023-07-010-001). As this was a retrospective chart review study, informed consent was not required.
Definition and classification of variables
Hypersensitivity reactions were further categorized by temporal onset. Reactions occurring within 1 hour after drug administration were defined as immediate, while those occurring later than 1 hour were defined as delayed.
The severity of anaphylaxis was graded according to BrownŌĆÖs classification in 2004 as follows: mild (skin and subcutaneous involvement such as erythema, urticaria, periorbital edema, or angioedema), moderate (respiratory, cardiovascular, or gastrointestinal involvement such as dyspnea, stridor, wheeze, nausea, vomiting, dizziness, diaphoresis, chest or throat tightness, or abdominal pain), and severe (hypoxia, hypotension, or neurologic compromise, defined as cyanosis, SpO2 Ōēż 92%, or systolic blood pressure < 90 mmHg, confusion, collapse, loss of consciousness, incontinence) [12].
Underlying comorbidities included myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular accident or transient ischemic attack, dementia, chronic obstructive pulmonary disease, connective tissue disease, peptic ulcer disease, chronic liver disease, diabetes (uncomplicated or with chronic complications), hemiplegia, chronic kidney disease, and malignancy.
Information regarding demographic characteristics (age, sex), history of allergic diseases (asthma, allergic rhinitis, atopic dermatitis, food allergy, chronic urticaria, and drug allergy), and clinical features of the hypersensitivity event (organ-specific symptoms including cutaneous, respiratory, cardiovascular, neurologic, and gastrointestinal systems) was retrospectively collected using electronic medical records and case report forms.
A history of drug allergy was defined as any previous allergic reaction to a medication prior to the index ED visit. Recurrent reactions were defined as hypersensitivity events occurring after reexposure to the same drug or to a structurally or functionally related drug, thereby encompassing potential cross-reactivity, and were separately classified as recurrent reactions due to known culprit drugs.
Finally, culprit drug identification was assessed by integrating clinical history with the results of serum-specific IgE testing, skin testing, and drug provocation testing, as detailed in the Results section.
Statistical analysis
Continuous variables were presented as mean ┬▒ standard deviation, while categorical variables were presented as frequencies and percentages. Continuous variables were compared using the StudentŌĆÖs t-test, and categorical variables were compared using the chi-squared test or the Fisher exact test, as appropriate. Univariate logistic regression was conducted to identify factors associated with allergist visits or culprit drug identification, and results were reported as odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was set at p < 0.05. All statistical analyses were performed using the R software version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Clinical characteristics of the study patients with immediate- and delayed-type reactions
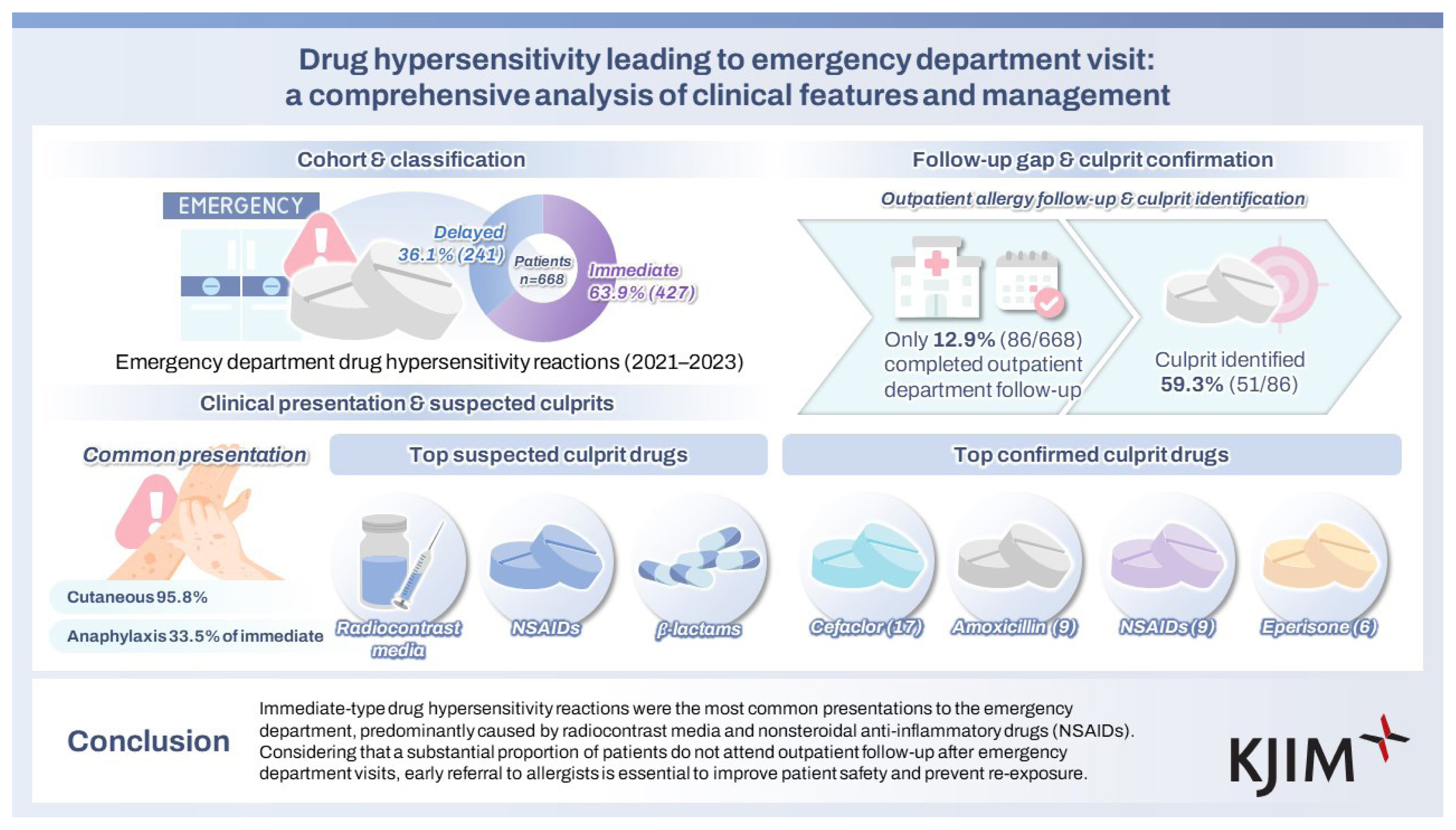
A total of 668 patients with suspected DHRs were included in the analysis, of which 427 (63.9%) were classified as immediate-type and 241 (36.1%) as delayed-type reactions. Table 1 presents the clinical characteristics of the study patients and compares immediate- and delayed-type reactions. Demographic characteristics, including age, sex, and comorbidity prevalence, were comparable between immediate- and delayed-type reactions. The prevalence of allergic diseases, history of food or drug allergies, and recurrent reactions due to known culprit drugs also showed no significant differences between the groups.
Cutaneous manifestations were the most common organ-specific symptoms observed in 95.8% of patients. Compared to the immediate-type group, the delayed-type group had a significantly higher frequency of cutaneous involvement (98.3% vs. 94.4%, p = 0.024), particularly erythema (76.8% vs. 63.7%, p = 0.001) and itching (62.7% vs. 50.1%, p = 0.002). Respiratory symptoms were more frequent in the immediate-type group (34.4% vs. 21.2%, p < 0.001), including dyspnea (28.6% vs. 17.4%, p = 0.002). Cardiovascular involvement, although not significantly different overall (9.6% vs. 6.2%, p = 0.171), was associated with a higher rate of hypotension in the immediate-type group (7.5% vs. 3.3%, p = 0.044). Neurological symptoms were more commonly reported in the immediate-type group (9.6% vs. 3.3%, p = 0.005), with dizziness being significantly more frequent (7.0% vs. 0.8%, p = 0.001). Gastrointestinal symptoms were more common in the immediate-type group (9.1% vs. 5.0%, p = 0.073), and abdominal pain was significantly more common (4.0% vs. 0.8%, p = 0.035).
In the delayed-type group (n = 241), skin eruptions were overwhelmingly consistent with maculopapular eruption (MPE). SCARs were rare, with only one case clinically suspected as StevensŌĆōJohnson syndrome (SJS, 1/241, 0.4% of delayed; 1/668, 0.1% overall).
Causative drugs of the DHRs in this study
The distribution of culprit drugs by reaction type is summarized in Supplementary Table 1. The most frequently implicated drug classes are radiocontrast media, nonsteroidal anti-inflammatory drugs (NSAIDs), and ╬▓-lactam antibiotics. Radiocontrast media, almost exclusively iodinated contrast media (ICM) with a single case of gadolinium-based contrast agent (GBCA), were significantly more common in immediate-type reactions than in delayed-type reactions (22.5% vs. 12.4%, p < 0.001). ╬▓-lactam antibiotics also showed a significant difference, with a higher frequency in immediate-type reactions (6.3% vs. 5.8%, p = 0.004). Fluoroquinolones, within the ŌĆ£other antibioticsŌĆØ category, were observed more often in immediate-type reactions (64.3% vs. 9.1%, p = 0.012), suggesting a notable pattern despite their lower overall frequency. Reactions involving multiple suspected drugs accounted for nearly half of all cases (50.5%), with higher proportions observed in delayed-type reactions (60.2% vs. 45.0%), without statistical significance.
Clinical characteristics of immediate-type reactions: anaphylaxis vs. non-anaphylaxis
Among the 427 patients with immediate-type reactions, 143 (33.5%) met the criteria for anaphylaxis. Table 2 compares the clinical characteristics of anaphylactic and non-anaphylactic reactions.
Patients with anaphylaxis were significantly older than those without anaphylaxis (45.6 ┬▒ 16.5 yr vs. 42.1 ┬▒ 17.2 yr, p = 0.041). Although the distribution across age categories showed only a borderline difference (p = 0.054), the proportion of anaphylactic cases was higher among patients aged Ōēź 60 years. Sex distribution and presence of underlying comorbidities were comparable between the two groups. Patients with anaphylaxis had a higher prevalence of allergic diseases (47.6% vs. 35.2%, p = 0.018), including asthma (4.9% vs. 0.7%, p < 0.001), allergic rhinitis (11.2% vs. 3.2%, p < 0.001), and food allergies (8.4% vs. 5.6%, p = 0.021). The proportion of recurrent reactions due to known drugs did not differ significantly between the groups (18.9% vs. 16.0%, p = 0.482).
According to the Brown severity classification, none of the cases were categorized as mild. Most cases were classified as moderate (84 cases, 58.7%), while 59 cases (41.3%) were classified as severe anaphylaxis. Among the 143 patients with anaphylaxis, serum tryptase was measured in 43 cases, with a mean level of 17.0 ┬▒ 16.1 ng/mL. Elevated tryptase levels (> 11.4 ng/mL) were found in 22 patients (51.2%). The treatment patterns in the ED differed markedly. Patients with anaphylaxis were more likely to receive corticosteroids (88.1% vs. 60.9%, p < 0.001), inhaled ╬▓-agonists (11.9% vs. 1.1%, p < 0.001), and epinephrine (45.5% vs. 2.8%, p < 0.001). The use of H1- and H2-antihistamines did not differ significantly between the groups.
Radiocontrast media and NSAIDs have been frequently reported in patients with immediate-type reactions. Among these, in patients with anaphylaxis, the most common single drug culprit was NSAIDs in 21 patients (14.7%), with ketorolac accounting for four cases (2.8%), followed by cimetropium bromide in seven patients (4.9%), and cefaclor in six patients (4.2%). Reactions involving multiple suspected drugs were observed in 97 patients (67.8%), most of whom were involved in regimens containing NSAIDs (Supplementary Table 1).
Comparison of drug hypersensitivity patients with and without outpatient follow-up after an ED visit
Table 3 provides a comparison of patients with drug hypersensitivity with and without outpatient follow-up after an ED visit. Among 668 patients with DHRs, 86 (12.9%) underwent outpatient follow-up after their ED visit. Patients who returned for follow-up were more likely to have experienced anaphylaxis (45.3% vs. 17.9%; OR 3.81, 95% CI 2.37ŌĆō6.13, p < 0.001), and to have allergic comorbidities such as asthma (OR 5.41, 95% CI 1.69ŌĆō17.34, p = 0.005), allergic rhinitis (OR 9.52, 95% CI 4.45ŌĆō20.36, p < 0.001), food allergy (OR 3.97, 95% CI 1.80ŌĆō8.75, p < 0.001), and chronic urticaria (OR 29.65, 95% CI 5.69ŌĆō154.45, p < 0.001).
Patients with follow-up visits also showed a higher prevalence of respiratory (44.2% vs. 27.5%; OR 2.09, 95% CI 1.31ŌĆō3.32, p = 0.002), cardiovascular (22.1% vs. 6.4%; OR 4.18, 95% CI 2.27ŌĆō7.68, p < 0.001), neurologic (16.3% vs. 6.0%; OR 3.04, 95% CI 1.56ŌĆō5.92, p = 0.001), and gastrointestinal symptoms (15.1% vs. 6.5%; OR 2.55, 95% CI 1.30ŌĆō5.01, p = 0.007), particularly dyspnea, hypotension, dizziness, and abdominal pain. Cutaneous symptoms, such as erythema and itching, were more common among patients without follow-up.
Among those with outpatient visits, 54.7% underwent drug provocation testing with a test positivity rate of 19.1%. Specific IgE measurements and skin tests were performed in 43.0% and 41.9% of patients, respectively, with positivity rates of 62.1% and 66.7%, respectively. Patch testing to the suspected drug was performed in 3 patients (3.5%), with a positivity rate of 33.3%. A drug safety card was issued to 72.1% of patients who received outpatient evaluation.
Comparison of outpatient follow-up patients with and without identified culprit drugs
Among the 86 patients who returned for outpatient follow-up, the culprit drug was successfully identified in 51 cases (59.3%). Patients taking identified culprit drugs were more likely to have experienced immediate-type reactions (82.4% vs. 48.6%, p = 0.002) and anaphylaxis (56.9% vs. 28.6%, p = 0.018) than those who did not. Although not statistically significant, a higher proportion of patients with identified culprits had a history of drug allergy (33.3% vs. 20.0%) and recurrent reactions to known drugs (26.5% vs. 11.4%).
The distribution of organ-specific symptoms, including cutaneous, respiratory, cardiovascular, neurological, and gastrointestinal manifestations, did not differ significantly between the groups.
Among the 86 patients who underwent outpatient follow-up, most were exposed to multiple suspected drugs rather than a single agent (70.6% vs. 29.4% in the identified group; 77.1% vs. 22.9% in the unidentified group). Among patients with multiple suspected drugs, the most common combination was NSAIDs and ╬▓-lactams, which were more frequently observed in the culprit-identified group (61.1% vs. 29.6%, p = 0.054). Among 36 patients with multiple suspected drugs, the NSAID + ╬▓-lactam combination (n = 22) yielded 11 cases with cefaclor, four with amoxicillin, and two with NSAIDs as confirmed culprits; the remaining cases were attributed to other drugs. In the NSAID + muscle relaxant group (n = 7), two cases were confirmed as NSAIDs and one as eperisone, with the others due to different drugs. Overall, 20 patients (55.6%) received a confirmed culprit drug included in the initially suspected combination.
Diagnostic evaluation differed between the groups: patients with identified culprit drugs were more likely to have undergone drug provocation tests (66.7% vs. 37.1%, p = 0.013), and their serum-specific IgE testing showed a significantly higher positivity rate (76.9% vs. 27.3%, p = 0.004). Drug safety cards were issued more frequently in this group (90.2% vs. 45.7%, p = 0.001). Detailed comparisons between the groups are provided in Supplementary Table 2. Notably, most patients without an identified culprit drug either declined provocation testing or did not return for outpatient evaluation.
Among the 86 patients who returned for outpatient follow-up, 51 (59.3%) ultimately had the culprit drug identified. Culprit identification was most commonly achieved with cefaclor (n = 17), amoxicillin/amoxicillin-clavulanate (n = 9), NSAIDs (n = 9), and eperisone (n = 6). Among the nine NSAID-related cases, two were classified as single NSAID-induced urticaria/angioedema/anaphylaxis (SNIUAA): one case was attributed to acetaminophen alone, and one case to acetylsalicylic acid alone. The remaining seven cases were classified as NSAID-induced urticaria/angioedema/anaphylaxis (NIUAA); five patients showed cross-reactive hypersensitivity to multiple NSAIDs, and two patients additionally reacted to celecoxib, indicating broad cross-intolerance. The diagnostic methods varied, including combinations of clinical history, ImmunoCAP testing, skin testing, and drug provocation testing. Detailed information regarding the diagnostic strategies is presented in Table 4.
DISCUSSION
This single-center retrospective study characterized DHRs presenting to the ED and evaluated culprit drug identification through allergy outpatient follow-ups. Among the 668 patients, 63.9% had immediate-type reactions and 36.1% had delayed-type reactions. Cutaneous manifestations were common in both immediate- and delayed-type reactions; however, respiratory, cardiovascular, and neurological symptoms were more frequently observed in immediate-type reactions. Of the 427 patients with immediate-type reactions, 33.5% met the criteria for anaphylaxis, which was associated with a higher prevalence of underlying allergic diseases and an epinephrine administration rate of 45.5%. Radiocontrast media, NSAIDs, and ╬▓-lactams are the most common culprit drug classes, with reactions involving multiple suspected drugs occurring frequently. Only 12.9% of patients had outpatient follow-up, but among those who did, 59.3% had a confirmed culprit drug, most commonly cefaclor, amoxicillin/amoxicillin-clavulanate, NSAIDs, or eperisone. In patients with multiple suspected drugs, the NSAID plus ╬▓-lactam combination was the most common, with more than half having the culprit drug within this combination. Building on these methodological strengths, several notable findings emerged in our cohort.
Previous large-scale studies in Spain and Croatia identified ╬▓-lactam antibiotics as the most common culprits of ED visits in DHRs [6,8]. However, these studies relied mainly on ED records or diagnoses without allergist confirmation, limiting the diagnostic accuracy. Follow-up rates were also low, with < 10% in one Lebanese study [7] and as low as 2.3% in a pediatric ED series from Australia [13], and confirmatory testing was rarely performed.
In contrast, our study directly linked ED cases to allergist evaluation, enabling a definitive diagnosis through a multimodal approach that included medical history, ImmunoCAP, skin testing, and drug provocation testing. By analyzing both immediate- and delayed-type reactions, we also compared phenotypes, including anaphylaxis and non-anaphylaxis, and assessed diagnostic yield across multiple drug exposures. Taken together, these features allow us to identify several notable findings. First, radiocontrast media were the leading culprit in our cohort, likely reflecting their high utilization in KoreaŌĆÖs diagnostic and therapeutic settings, with national surveillance data showing more than a tenfold rise in related ADR reports between 2009 and 2019 [14]. Second, the unexpectedly high proportion of delayed reactions suggests that such events can be sufficiently severe or distressing to prompt ED visits, underscoring the underrecognized clinical burden [15]. We further delineated delayed phenotypes, showing that most delayed ED presentations manifested as MPE, whereas SCAR was uncommon and limited to a single case clinically suspected of SJS. This distribution is consistent with the expectation that benign exanthems predominate in ED-identified delayed reactions, while true SCARs are infrequent but high-stakes and warrant targeted evaluation and early referral. Third, among anaphylactic patients, comorbid asthma and allergic rhinitis were more prevalent, consistent with known risk factors [16,17], and elevated serum tryptase (Ōēź 11.4 ng/mL) was significantly more frequent, supporting its diagnostic value [18,19]. Fourth, although the epinephrine administration rate of 45.5% in anaphylaxis exceeded that reported in some previous studies [13, 20], this rate primarily reflects administration in Brown grade 3 cases and may therefore not indicate underuse. Nevertheless, this underscores the ongoing need for education on timely recognition and administration in clinical practice [21]. Finally, the high confirmation rate of culprit diagnoses among follow-up patients, an observation not reported in prior ED studies, demonstrates the clinical value of post-ED allergy evaluation for securing accurate diagnoses and preventing reexposure. This study underscores the need to strengthen the continuum of care for patients presenting to the ED with DHRs. First, establishing a direct pathway for allergy specialist assessment, either during the ED visit or through structured referral and appointment systems at discharge, could improve diagnostic accuracy and patient safety. Second, preventive strategies should focus on high-risk drugs, such as radiocontrast media, NSAIDs, and ╬▓-lactam antibiotics, with particular attention to patients exposed to multiple agents, where standardized diagnostic algorithms could facilitate culprit identification. Third, greater awareness of delayed-type reactions is warranted, as these account for a substantial proportion of ED presentations and can significantly affect patient well-being. Finally, improving adherence to guideline-recommended epinephrine use for anaphylaxis will require targeted clinician education and streamlined protocols to ensure its timely administration.
This study has several limitations. First, as this was a single-center and single-nationality retrospective study, the generalizability of the findings is limited, and there is potential for selection and information bias. Second, the proportion of patients who underwent outpatient follow-up after their ED visit was low, potentially leading to an underestimation of the actual confirmation rate. Some patients who did not attend follow-up might have still had their culprit drug identified if evaluated. Third, specific clinical outcomes and severity assessments relied on medical records, which may have been subject to inaccuracies or incomplete documentation. Fourth, we classified reaction timing as immediate (Ōēż 1 h) and delayed (> 1 h), a simplified scheme compared with the commonly used classifications of immediate, accelerated (1ŌĆō72 h), and delayed (> 72 h). This difference should be considered when compared to other studies. Fifth, owing to limited clinical information and incomplete outpatient follow-up, all NSAID hypersensitivity reactions could not be accurately classified into established subtypes. Nevertheless, among the nine patients who were fully evaluated in the outpatient clinic, seven were classified as NIUAA and two as SNIUAA. These findings underscore the importance of structured outpatient follow-up and comprehensive evaluation to identify the exact causative drug, which not only ensures the safe and appropriate use of medications in affected patients but also prevents unnecessary avoidance of the entire NSAID class, as illustrated by the two cases of NIUAA. Although cross-reactivity is primarily attributed to nonselective cyclooxygenase-1 inhibition, cross-intolerance has also been reported in a minority of patients exposed to selective cyclooxygenase-2 inhibitors, such as celecoxib. In a Korean cohort, the overall celecoxib cross-reaction rate was 10.3%, with particularly high rates of aspirin-exacerbated chronic urticaria (17.4%) and aspirin-exacerbated chronic urticaria (8.7%) [22]. The two celecoxib-reactive cases in our study likely fell within this small but clinically relevant exception category. Sixth, because the radiocontrast media in this study were predominantly ICM, with only one GBCA case, the distribution largely reflects the specific agents used at our center and may not be generalizable to other institutions or populations. Finally, owing to the retrospective observational design, causal relationships cannot be firmly established, and potential confounding factors cannot be ruled out.
In conclusion, this study is the first to provide a comprehensive analysis of patients presenting to the ED with DHRs, including the outcomes of culprit drug identification during outpatient follow-up. Both immediate- and delayed-type reactions were frequent, and radiocontrast media emerged as the most common culprit. The high confirmation rate among patients who attended follow-up emphasizes the importance of early referral to allergy specialists in the ED. Our findings highlight several priorities: preemptive risk assessment for high-risk drugs, standardized diagnostic procedures for patients with multiple drug exposures, greater recognition of delayed reactions, and improved adherence to epinephrine use for anaphylaxis. Future multicenter prospective studies are needed to validate these strategies and to establish a structured ED-based drug allergy management system.
KEY MESSAGE
1. Emergency departmentŌĆōdiagnosed drug hypersensitivity reactions were predominantly immediate-type reactions, most commonly triggered by radiocontrast media, NSAIDs, and ╬▓-lactams.
2. Anaphylaxis occurred in one-third of immediate-type reactions and was significantly associated with allergic comorbidities.
3. Despite ED diagnosis, outpatient allergy follow-up rates were low; however, more than half of the evaluated patients had a confirmed culprit drug, underscoring the importance of early referral to allergists to prevent reexposure and improve patient safety.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print





