


A 65-year-old male visited the emergency department and presented as anterior ST-elevation myocardial infarction (STEMI). Coronary angiography (CAG) showed severe stenosis (90%) in the proximal-to-mid segment of the left anterior descending artery as the culprit lesion. Despite severe tortuous the lesion, two drug-eluting stents (DES) (Synergy, 3.5 × 38 mm and 2.75 × 38 mm) were successfully implanted. Intravascular ultrasound (IVUS) was performed pre-optimization to assess stent apposition; however, catheter entrapment occurred at the proximal stent distal site during IVUS probe withdrawal. Forced extraction resulted in stent deformation with partial strut stripping, confirmed by repeat angiography. To address this complication, an additional stent (Synergy, 3.0 × 12 mm) was deployed (Fig. 1).
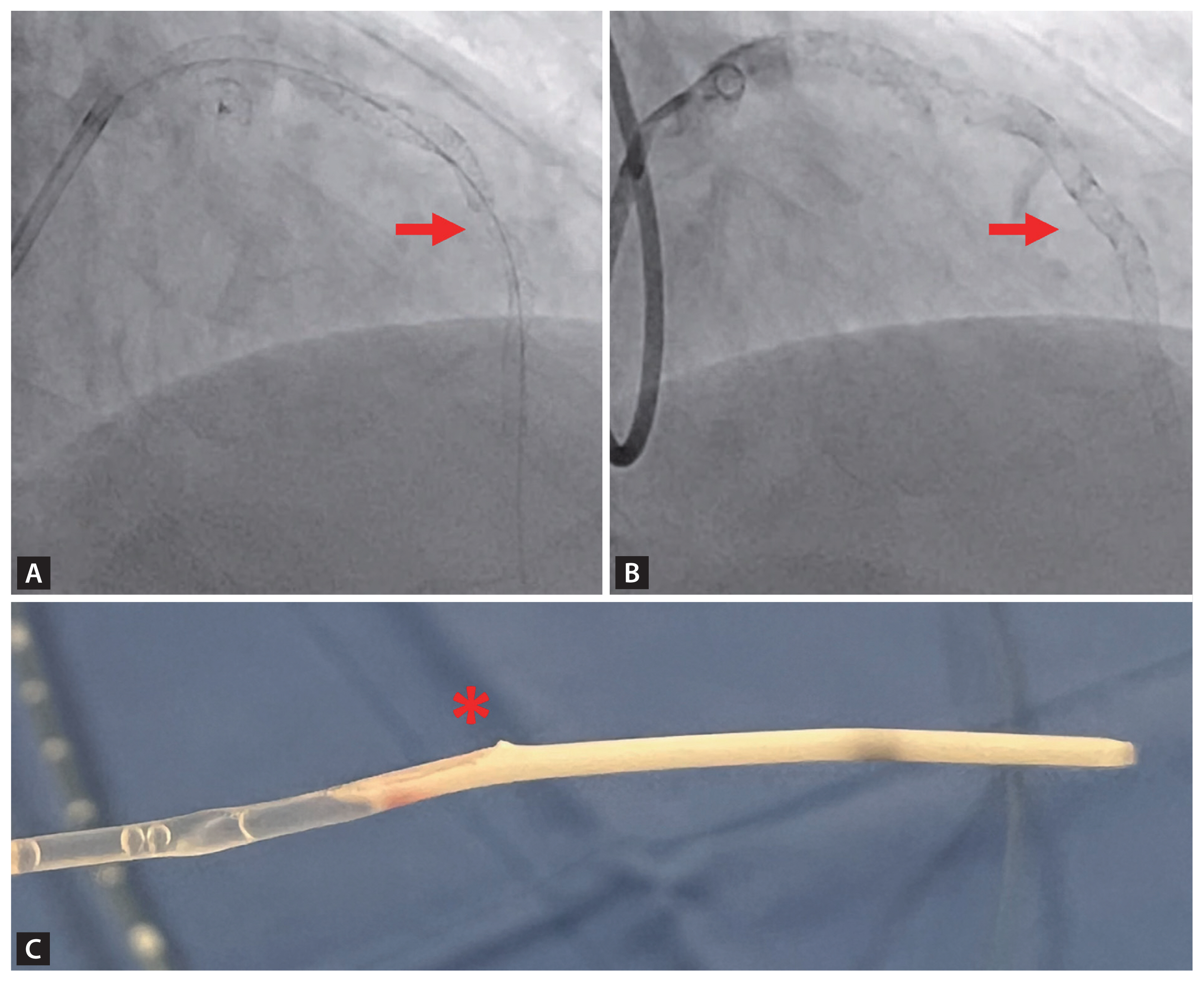
A few days later, a 64-year-old male presented as inferolateral STEMI. CAG revealed thrombotic occlusion in the proximal left circumflex artery. Primary percutaneous coronary intervention was performed with DES (Synergy Megatron, 4.0 × 28 mm). During post-stent IVUS evaluation, catheter entrapment occurred at the stent’s distal edge upon withdrawal attempts. This time, the cut-and-inserting wire technique was employed: a guidewire was advanced through the empty space after removing optic fiber in an attempt to retrieve the trapped catheter (Fig. 2). This approach successfully extricated the device without stent displacement or vascular injury. Final angiography confirmed that coronary flow was restored with no residual stenosis.
In both cases, catheter entrapment occurred at angulated stent segments within tortuous coronary anatomy during IVUS evaluation performed prior to post-dilation. The shared mechanism involved strut malapposition at bend points, where the IVUS catheter’s exit port became anchored between under-expanded struts. A critical divergence emerged in management:
Case 1: Forcible withdrawal induced stent deformation, necessitating additional stenting.
Case 2: The cut-and-inserting wire technique facilitated atraumatic retrieval.
Catheter entrapment is a rare complication [1]. Major risk factors include stent under-expansion, tortuous anatomy, and small stent diameter [1]. Through these two cases, the importance of adequate post-dilation before IVUS assessment in PCI for small and tortuous lesions was underscored.
Informed consent was obtained from patients.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





