


INTRODUCTION
As the global population continues to age, the incidence of end-stage kidney disease (ESKD) among older adults has increased in many countries [1,2]. Most of them require kidney replacement therapy (KRT), such as dialysis or kidney transplantation. However, older adults are generally not considered suitable candidates for kidney transplantation, resulting in a gradual increase in the number of older patients undergoing dialysis. According to the Korean Renal Data System (KORDS), patients aged ≥ 65 years have accounted for more than half of the total dialysis population in Korea since 2018 [3]. Older patients undergoing dialysis have a high prevalence of adverse clinical outcomes. From 2013 to 2023, hospitalization rates were the highest among individuals aged ≥ 75 years, and all-cause mortality increased in this group while it declined in younger populations [4]. These trends highlight the growing importance of individualized management strategies for older adults undergoing dialysis.
Physiological age with well-preserved physical function is likely more clinically relevant than chronological age or longevity for quality of life in older patients [5]. Collectively, frailty, malnutrition, and multimorbidity are used to define the physiological age of older adults. In older adults requiring dialysis, these age-related conditions can influence the choice of dialysis modality and lead to changes in dialysis prescriptions as well as often result in patients requiring assistance with treatment implementation. Therefore, physicians play a key role in supporting older patients in making decisions about dialysis initiation and modalities and establishing treatment strategies tailored to patients’ clinical status. This review addresses clinical considerations in dialysis decision-making and proposes optimal treatment strategies tailored to the unique needs of older patients with chronic kidney disease (CKD). This review focuses primarily on issues related to dialysis therapy in the treatment management of older adults with ESKD, with the exception of kidney transplantation.
INITIATION OF DIALYSIS THERAPY IN OLDER PATIENTS
Decision to initiate dialysis therapy
In general, dialysis improves both the quality of life and survival of patients with advanced CKD compared to conservative management [6,7]. However, several studies have found that the survival benefit of dialysis over conservative management tends to disappear in patients aged > 80 years [6,7]. Early mortality within the first 120 days after hemodialysis (HD) initiation remains higher in older patients than in younger patients [8]. In older adults with limited life expectancy, dialysis may not offer a survival benefit and could be potentially harmful. In this context, conservative kidney management (CKM), in which supportive care and symptom- focused treatment are provided without dialysis, may be an alternative for older adults with limited life expectancy [9]. Therefore, whether CKM or dialysis is more appropriate for older patients with limited life expectancy who require KRT must be determined.
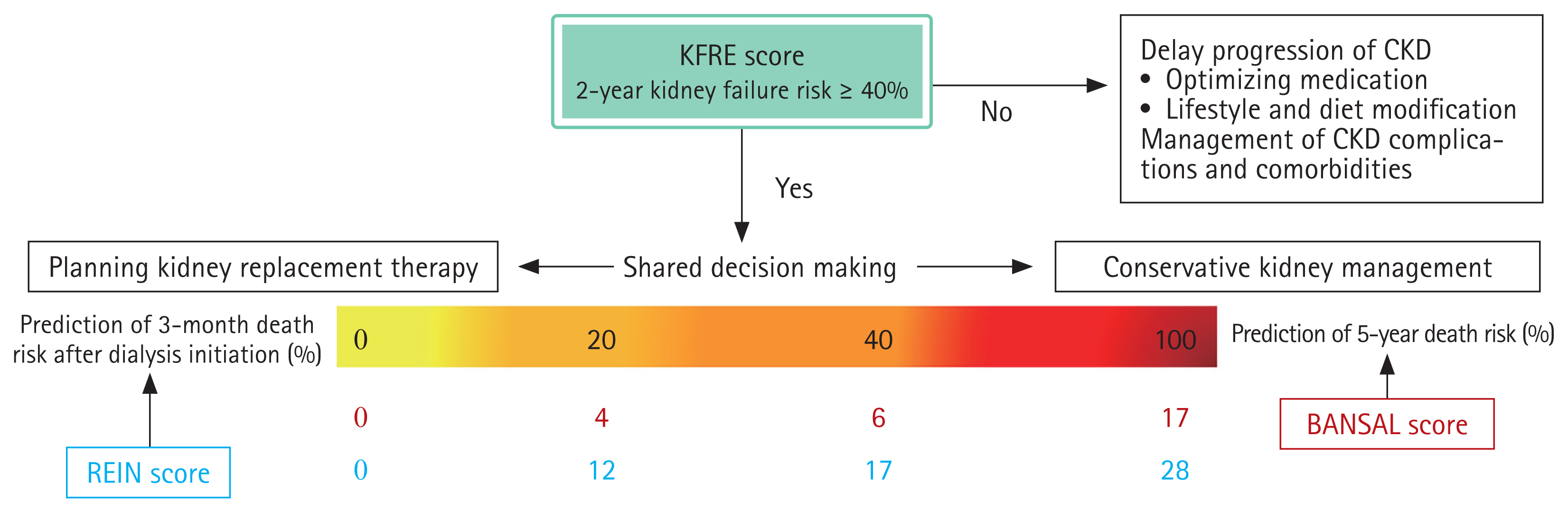
Prediction tools and scoring systems can help guide risk stratification for mortality and progression to ESKD in older patients with CKD stages 3b–5 and support individualized decision-making for KRT initiation. In 2017, the European Renal Best Practice (ERBP) guidelines recommended a stepwise approach using validated tools to estimate kidney failure and mortality risks (Fig. 1, Supplementary Table 1) [10]. This framework advises physicians to assess both the 5-year mortality risk using Bansal scores and the risk of progression to kidney failure using the Kidney Failure Risk Equation (KFRE) [11,12]. When the mortality risk is high, CKM is generally considered more appropriate than KRT. Conversely, a high KFRE score combined with a low mortality risk may support early preparation for KRT, whereas a low KFRE score favors continued nephroprotective care without immediate KRT. When patients are expected to initiate KRT within 3–6 months, their Renal Epidemiology and Information Network scores can be used to estimate short-term mortality after dialysis initiation, helping physicians and patients more accurately weigh the potential benefits and burdens of dialysis [13]. However, these models and guidelines were developed based on European cohorts and have not been specifically adapted for use in Korean clinical settings. To address this issue, To address this issue, the Korean Society of Geriatric Nephrology recently developed a 6-month mortality prediction model for patients aged ≥70 years requiring HD, using data from a multicenter retrospective cohort including 16 institutions in Korea [14]. Further development of prediction models based on Korean data could improve clinical decision-making and support dialysis planning tailored to the older Korean population.
The preferences of older patients and their caregivers are important when deciding whether to initiate dialysis. Although dialysis is a vital life-sustaining therapy, it can cause burdens and adverse effects, such as fatigue, repeated needle punctures, frequent hospitalizations, and high maintenance costs [15]. Some older patients with advanced CKD prioritize their care goals and values over longevity and prefer CKM to avoid complications. In addition, caregivers of older patients, who are usually family members, play a key role in the decision-making process for dialysis because they share patients’ physical, psychological, and financial burdens [16]. They provide practical support for peritoneal dialysis (PD), assist with transportation to HD units, and often act as primary decision-makers for older patients with cognitive impairment. Therefore, shared decision-making (SDM) involving patients, caregivers, and healthcare providers is essential throughout the course of treatment from the initiation of dialysis to its maintenance and withdrawal. SDM can help close medical information gaps among patients, caregivers, and clinicians, support patient-centered decisions, and promote patients’ decisional autonomy [17].
Timing of dialysis initiation
Age is a well-established risk factor for unplanned dialysis because older patients tend to delay decisions regarding dialysis initiation and fail to achieve mature vascular access (VA) [18]. Unplanned dialysis initiation in older adults is associated with higher mortality and hospitalization risks [19,20]. Therefore, accurate prediction of progression to kidney failure and timely initiation of dialysis are essential for older patients.
Accurate assessment of kidney function in older patients is essential to determine the optimal timing of dialysis. However, serum creatinine levels and uremic symptoms may not be reliable indicators of kidney failure in this population. Serum creatinine has inherent limitations as a marker of glomerular filtration because non-glomerular filtration rate (GFR) determinants, such as muscle mass, tubular secretion, and dietary intake, influence its accuracy. In older patients with frailty and sarcopenia, estimated GFR (eGFR) is over-estimated due to reduced muscle mass and low creatinine levels. Given these limitations, the 2024 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines recommend using the combined creatinine-cystatin C equation (eGFRcr-cys) in clinical situations in which creatinine generation is reduced due to low muscle mass or creatinine secretion or extrarenal elimination is altered by specific medications [21]. Therefore, the eGFRcr-cys equation is recommended for assessing kidney function in older adults.
The KDIGO 2024 clinical practice guidelines recommend that decisions regarding dialysis initiation be based on a composite assessment of uremic symptoms and signs, quality of life, preferences, kidney function, and laboratory abnormalities [21]. The guidelines emphasize that clinical circumstances that require dialysis initiation typically occur when eGFR falls between 5 and 10 mL/min/1.73 m2. However, the decision should primarily be guided by clinical signs, symptoms, and overall patient condition rather than eGFR alone. Assessment of uremic symptoms in older patients is particularly challenging. Symptoms such as cognitive impairment, fatigue, anorexia, and pruritus are often subjective and nonspecific in this population. Furthermore, these symptoms can overlap with comorbidities commonly observed in older adults, including cardiovascular disease, neurocognitive disorders, and psychiatric conditions, making true uremic manifestations difficult to distinguish. Therefore, careful clinical observation and differentiation of uremic signs and symptoms from those related to other comorbidities are essential when considering dialysis initiation in older adults.
Selection of dialysis modality
HD and PD have no absolute contraindications, except when VA cannot be established or the peritoneal membrane is nonfunctional in older patients. In general, dialysis modality selection is based on comorbidities, occupational and lifestyle factors, and the need to preserve residual kidney function (RKF). In older adults, additional factors such as functional impairment, multiple comorbidities, and familial support should be considered because they may further influence the advantages and disadvantages of each modality.
The advantages of PD include RKF preservation, feasibility of home-based dialysis, and improved cardiovascular stability. However, functional impairments associated with frailty and aging may increase the risk of peritonitis, particularly in relation to malnutrition and difficulties in performing PD procedures [22,23]. Poor performance status often prevents older adults from performing PD independently; thus, they require caregiver assistance. Regarding HD, patients benefit from prompt medical attention from physicians and can maintain social relationships through regular hospital visits. However, HD requires patients and their caregivers to spend additional time and financial costs on transportation to dialysis facilities. Moreover, older adults, especially those with cardiovascular disease or impaired immune function, are vulnerable to intradialytic hypotension (IDH) and dialysis-related bloodstream infections.
In older patients with ESKD, the effects of dialysis modality on mortality risk must be considered when making appropriate treatment decisions [24]. A recent meta-analysis revealed that PD has a higher mortality rate than HD in patients aged ≥ 60 years, particularly among those with diabetes, comorbidities, or prolonged dialysis duration. However, the difference in mortality risk between the two modalities appears to have diminished in studies conducted after 2010 [25]. Furthermore, a nationwide retrospective cohort study using data from the Korean National Health Insurance Service demonstrated that PD was associated with higher mortality rates than HD between 2004 and 2015 [26]. However, between 2012 and 2015, the mortality rate of PD became comparable to that of HD, regardless of age ≥ 65 years, diabetes status, or comorbidity burden. This improvement may be attributable to advancements in PD solutions and techniques and improvements in the management of cardiovascular complications.
In Korea, HD centers are unevenly distributed between urban and rural areas, and a substantial proportion of older patients live in rural areas. These patients often face a high risk of falls during transportation to HD facilities. Therefore, in older patients with a favorable physiological status who do not have diabetes or other major comorbidities, PD can be a practical and appropriate treatment strategy, particularly in Korean healthcare settings. Thus, an assisted PD system that provides a model of care in which trained healthcare personnel or caregivers support patients in performing PD at home needs to be established to increase PD adoption [27].
STRATEGIES FOR HEMODIALYSIS MANAGEMENT IN OLDER PATIENTS
Selection of vascular access
Arteriovenous fistula (AVF) is generally preferred over other types of VA because of its lower risks of complications, infection, and mortality, as well as superior patency compared to arteriovenous graft (AVG) [28,29]. Trends in VA creation have shifted from the “fistula-first” approach outlined in the 2006 Kidney Disease Outcomes Quality Initiative (KDO-QI) guidelines to the “patient-first” approach in the updated 2019 guidelines [30]. The 2019 KDOQI guidelines recommend the use of a long-term central venous catheter (CVC) or AVG over AVF in patients with limited life expectancy or restricted vascular anatomy. Older adults frequently present with poor vascular anatomy and multiple comorbidities that contribute to reduced life expectancy. The 2023 KORDS showed that among older patients in Korea, the proportion of AVF tended to decrease with age, whereas those of AVG and CVC increased [4].
AVF is the preferred type of VA because of its superior long-term patency and lower complication rates. However, AVF requires a longer maturation period and is associated with a higher primary failure risk [31]. The high prevalence of diabetes, peripheral vascular disease, and anatomic restrictions makes older patients particularly vulnerable to primary failure of AVF [32]. The high risk of maturation failure may increase the likelihood of death before successful AVF use in older patients with limited life expectancy. In contrast, a CVC-only strategy enables prompt dialysis initiation and avoids unnecessary procedures related to arteriovenous (AV) access (Table 1). Furthermore, AVG allows for early cannulation to ensure timely dialysis initiation and serves as a catheter-sparing option [33,34]. Therefore, CVC and AVG may be more suitable than AVF for older patients with a limited life expectancy who are at high risk for AVF failure.
Patients undergoing HD with CVC have poorer survival rates than those with other AV access [33,35,36]. However, a selection bias may be present in older patients. Older adults often remain dependent on CVCs without transitioning to AV access owing to their short life expectancy and multiple comorbidities. Thus, their lower survival rates may not be entirely attributable to CVC use [37]. A retrospective study from the Korean insurance claims data found that the mortality rate between AVF and AVG was not significantly different in patients aged ≥85 years [29]. Therefore, when treating older patients, nephrologists and vascular surgeons should take a patient-centered approach rather than strictly follow the “fistula-first” strategy in older patients.
Incremental hemodialysis
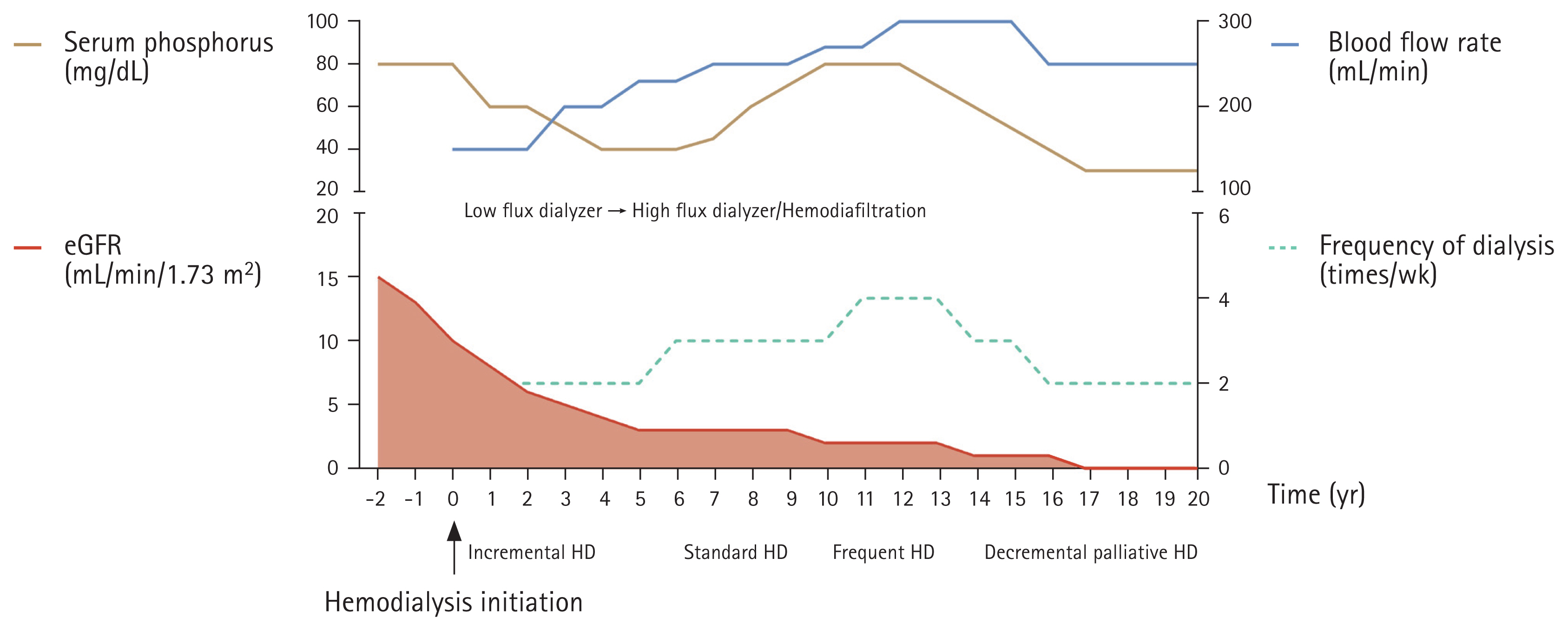
Almost all patients undergoing HD follow a standard thrice-weekly schedule from the start, whereas those undergoing PD typically adjust dialysis doses incrementally based on a decline in RKF [38]. RKF gradually declines after dialysis initiation, regardless of modality; therefore, an approach similar to “incremental HD” can be applied to PD. In incremental HD, dialysis starts at a reduced dose, such as twice-weekly or three hours per session, and gradually increases to the standard thrice-weekly, four hours per session, to compensate for progressive RKF loss (Fig. 2) [39]. Furthermore, the prescriptions of the size of dialyzer membrane, dialysate volume, and blood flow rate can be adjusted over time to maintain dialysis adequacy.
The incremental HD strategy may be suitable for older patients with low dietary intake and interdialytic weight gain (IDWG) because preserved RKF can compensate for skipped or shortened dialysis sessions. An incremental approach allows older patients to adjust gradually to the dialysis procedure and its associated complications, such as post-dialysis fatigue and muscle cramps. Furthermore, it reduces the frequency of hospital visits, thereby alleviating the burden on both patients and their caregivers, particularly for patients without a nearby HD facility.
Two pilot randomized controlled trials (RCTs) reported that incremental HD preserves RKF and reduces hospitalization rates without deteriorating metabolic derangements or increasing mortality compared with standard thrice-weekly HD in incident patients with RKF undergoing HD [40,41]. However, these studies did not specifically focus on older patients. In Korea, a pragmatic RCT has been underway since November 2021 to compare clinical outcomes, including mortality, hospitalization, and quality of life, between incremental HD with an initial twice-weekly schedule and conventional thrice-weekly HD in incident HD patients aged ≥ 60 years [42]. The findings from this and other ongoing RCTs are expected to support the clinical benefits and feasibility of an individualized approach to incremental HD in older patients (Table 2) [43–47].
Timely adjustments to the HD dose according to the patient’s decline in RKF are essential to prevent underdialysis. This requires regular assessment of RKF through urea clearance and other biomarkers, close monitoring of nutritional and fluid status, ongoing evaluation of patient adherence to dialysis schedules, and proactive patient education, especially for older adults, on the risks of underdialysis and the need for dose escalation [39].
Prescription of hemodialysis
Dry weight is defined as the lowest post-dialysis body weight tolerated without signs of hypovolemia [48]. The high prevalence of cardiovascular disease and autonomic dysfunction indicates that older patients are vulnerable to circulatory stress and volume changes during HD. Inappropriate titration of dry weight can increase the risk of IDH [48,49], which is associated with adverse outcomes, including post-dialysis fatigue, dialysis interruption, RKF decline, multi-organ ischemia, and mortality [50–52]. Recurrent IDH can also lead to cerebral hypoperfusion and worsening cognitive impairment in older patients [53,54]. Common strategies to prevent IDH include limiting IDWG and optimizing the target dry weight [48]. Dietary restriction is a feasible approach for reducing IDWG at the patient level. However, the risk of malnutrition must be carefully considered when treating older patients. Physicians should avoid setting the dry weight excessively low without properly assessing volume status. Instead, careful evaluation of fluid balance and individualized dry weight adjustment are essential, particularly when managing comorbidities in older patients.
HD adequacy is typically assessed based on urea clearance, expressed as Kt/V, which reflects the removal of small solutes. Clinical guidelines recommend a target single-pool (sp) Kt/V greater than 1.4, with a minimum delivered spKt/V of 1.2 [55]. However, age-related changes in body composition should be considered when interpreting Kt/V in older patients. Older adults often have lower muscle mass relative to total body mass than younger people, making their actual fluid volume smaller than the estimated distribution volume and leading to the potential underestimation of Kt/V. Consequently, older patients may receive unnecessarily high dialysis doses, increasing their exposure to HD-related materials and the risk of adverse events without clear clinical benefits [56,57]. A recent Korean study found that achieving a Kt/V greater than 1.4 did not provide additional survival benefits in patients aged ≥ 85 years [58]. In older patients undergoing HD, survival is closely associated with systolic blood pressure, mineral metabolism, nutritional status, and cardiovascular comorbidities [59]. Therefore, the adequacy of HD in older patients should be assessed through a comprehensive evaluation of clinical parameters, in addition to urea clearance.
Middle molecule clearance is another important indicator of HD adequacy. High-flux dialyzers and hemodiafiltration (HDF) provide superior clearance of middle molecules compared to low-flux dialyzers [60]. However, low-flux dialyzers are often preferred in older patients because they can achieve Kt/V targets while minimizing mineral and nutrient loss [61]. The accumulation of middle molecules can lead to adverse clinical outcomes such as dialysis-related amyloidosis and cardiovascular mortality [62,63]. Several studies have demonstrated the clinical advantages of high-flux HD and HDF in older patients. Huang et al. [64] found that high-flux HD had a lower risk of cardiovascular mortality compared with low-flux HD in older patients. A recent RCT showed that high-dose HDF with a convection volume of at least 23 L per session provides a survival benefit over high-flux HD, but only in patients aged ≥ 65 years [65]. Another RCT that included patients aged ≥ 65 years demonstrated that HDF was associated with a lower risk of asymptomatic IDH compared with high-flux HD, although health-related quality of life, morbidity, and mortality were similar between groups [66]. Therefore, when prescribing HD for older patients, nephrologists should prioritize comprehensive clinical benefits beyond laboratory targets for dialysis adequacy. Accordingly, high-flux HD and HDF may be favorable treatment options.
STRATEGIES FOR PERITONEAL DIALYSIS MANAGEMENT IN OLDER PATIENTS
Incremental peritoneal dialysis
Many centers have adopted incremental PD as an initial PD strategy since its introduction in the 1990s [67,68]. In incremental PD, the initial PD dose is lower than the standard full dose, but achieves target clearance with the support of RKF. Then, the dose is progressively increased as RKF declines [69]. For example, an incremental approach to continuous ambulatory peritoneal dialysis begins with three 1.5-L exchanges per day, with a gradual increase to the standard four 2-L exchanges as RKF declines. In automated peritoneal dialysis (APD) using a cycler, treatment starts with three 1.5- L nighttime exchanges, without daytime dwell. As RKF deteriorates, the dwell volume can be increased or daytime dwell can be added. In addition, PD can be prescribed for fewer than seven days per week by incorporating “PD holidays” during which dialysis is not performed (Table 3).
Incremental PD offers several advantages over standard full-dose PD, including better RKF preservation, reduced glucose exposure, and lower peritonitis risk [70]. Compared with standard PD, incremental PD is associated with superior technique survival, defined as a lower likelihood of transfer from PD to HD because of complications such as peritonitis, catheter dysfunction, or peritoneal membrane failure [71]. The 2020 International Society of Peritoneal Dialysis (ISPD) guidelines recommend modifying PD prescriptions to minimize the treatment burden on frail and older patients [72]. Incremental PD supports this strategy by requiring fewer PD exchanges and shorter dwell times during the early treatment phase. Thus, it enables older patients to gradually adapt to life with PD and offers them greater flexibility in daily life.
The 2020 ISPD guidelines highlight a paradigm shift from traditional adequacy targets based solely on small solute clearance to a goal-directed, person-centered approach to PD [72]. This approach emphasizes a comprehensive assessment that includes not only solute clearance but also laboratory parameters, nutritional status, and health-related quality of life. Therefore, alternative PD strategies, such as decremental PD and low-clearance non-incremental PD, may be appropriate for older patients. Decremental PD gradually reduces the volume and number of exchanges in response to changes in the patient’s clinical condition, taking an approach opposite to that of incremental PD. This strategy may be suitable for older patients who only require relief from uremic symptoms and are not aiming for specific clearance targets due to life expectancy or intractable illnesses. Low-clearance non-incremental PD delivers a lower dose than standard full-dose PD during the early phase. Unlike in incremental PD, the dose is not increased because the initial prescription meets low metabolic demands, particularly in older patients with low muscle mass and poor dietary intake.
Assisted peritoneal dialysis
Functional dependence has frequently been a barrier to PD eligibility for older patients. Decreased vision, reduced hand coordination, and cognitive dysfunction can interfere with the precise handling of PD equipment, potentially leading to adverse clinical outcomes [73,74]. Assisted PD, which involves support from family members, nurses, or paid caregivers, has allowed many older patients to become eligible for PD [75]. These caregivers assist patients by lifting dialysate bags, connecting and disconnecting them from the cycler, providing exit site care, and performing basic physical assessments [76].
Assisted PD is associated with favorable clinical outcomes in older patients. Advanced age has consistently been identified as a risk factor for peritonitis, likely because of multiple comorbidities and cognitive or functional impairments [22,23,73]. A retrospective analysis of the French PD registry demonstrated that nurse-assisted PD could reduce the risk of peritonitis in patients aged ≥ 75 years [77]. Another study from the same cohort revealed a significant association between nurse-assisted PD and lower risk of transfer to HD due to inadequate dialysis or infection than self-care PD [78]. Compared with patients who performed self-care PD, those receiving nurse-assisted PD were significantly older, with a median age of 80 years, and had a higher comorbidity index [78]. Therefore, assisted PD is an effective strategy to improve PD accessibility for older patients with functional dependence because it supports the proper manipulation of PD equipment and precise implementation of dialysis regimens prescribed by physicians.
Several strategies could promote the wider adoption of assisted PD in older patients. Stepwise and planned dialysis initiation can help start assisted PD in a timely manner, thereby preventing urgent HD via CVC and the subsequent transition to long-term HD [79]. Early identification of assistance needs and selection of assistance in advance during the initial assessment for PD eligibility can help establish PD as a practical and feasible option for older patients. Furthermore, APD or incremental PD strategies can reduce caregiver burden and barriers to PD entry. After PD initiation, regular assessment of changes in barriers to PD and timely adjustments to assistance are essential to sustain assisted PD. Patients may require additional assistance as their functional capacity declines with age or during acute illness. However, some patients regain independence after initiating dialysis and can transition from assisted to self-care PD. The 2024 ISPD position paper emphasizes that assisted PD should be recognized as a standard modality for patients with functional limitations, especially older patients [27]. The position paper further highlights the importance of implementing adaptable service models tailored to local resources, such as nurse-led or family-supported PD. These recommendations aim to enhance access to PD and reduce reliance on hospital-based HD services. Assisted PD programs, which include funding mechanisms and a stable supply of assistance, are provided by national or regional healthcare systems in many European countries [80,81]. However, in Korea, assistance is largely dependent on family members without financial support or systematic supervision, which may lead to difficulties in maintaining assisted PD. Therefore, establishing financial support through reimbursement policies, structured assisted PD programs, and standardized assistant training at the national level will be the key to expanding assisted PD among older patients in Korea.
STRATEGIES FOR MANAGING GERIATRIC SYNDROMES IN OLDER PATIENTS
Geriatric syndrome is a multifaceted clinical condition characterized by physical frailty, malnutrition, multiple comorbidities, and cognitive impairment associated with aging. With the growing number of older patients in this population, the prevalence of geriatric syndrome among patients with ESKD is increasing [82]. Most older patients with ESKD have two or more geriatric impairments that are often interrelated [83]. A comprehensive geriatric assessment should be implemented using a multidisciplinary approach involving nutritionists, physiatrists, psychiatrists, and neurologists to improve clinical outcomes in this population [84]. In this section, we discuss the clinical significance of frailty and nutrition, which are the two key components of geriatric syndrome, and propose strategies to improve outcomes in older patients undergoing dialysis.
Frailty
Frailty is a state of reduced ability to recover from physical or medical stress, leading to adverse clinical outcomes [85]. It is more prevalent in patients undergoing dialysis than in the general population [86]. A pre-existing uremic environment and metabolic disturbances during the pre-dialysis period activate inflammatory pathways and contribute to the development of sarcopenia [87]. Older patients often continue to experience frailty even after initiating dialysis because of nutritional losses during dialysis and frequent hospitalization related to comorbidities [88,89]. Frailty remains an under-recognized but important risk factor for adverse clinical outcomes in this population, including all-cause mortality and hospitalization [90,91].
Frailty assessments include indicators such as unintentional weight loss, self-reported exhaustion, low physical activity, and poor physical performance (Table 4) [90–96]. These assessments should be integrated into every step of the dialysis planning process for older adults. Frailty is a risk factor for death before dialysis initiation and during the course of dialysis in older patients with advanced CKD. Therefore, CKM may be considered a reasonable alternative to dialysis in patients with significant frailty [97]. When older patients decide to initiate dialysis, frailty assessments can help evaluate their physical function and predict the need for additional support. Individualized strategies should be developed to support dialysis based on the type and severity of functional impairment. For example, caregivers may be required to accompany patients who are unable to transfer themselves to HD centers or to support assisted PD in patients with impaired precise handling of PD or cognitive dysfunction. When establishing VA in older patients who opt for HD, frailty increases the risk of AVF maturation failure in addition to factors such as advanced age and comorbidities [98]. In such cases, CVC or AVG may be considered as VA alternatives.
Physical activity interventions can mitigate frailty, improve muscular strength and cardiovascular function, and reduce hospitalization in patients receiving dialysis [99–101]. The 2017 ERBP Clinical Practice Guidelines recommend structured and individualized exercise programs for older patients with advanced CKD, including those undergoing dialysis [10]. Exercise programs tailored to patients’ functional capacities and personal preferences can provide feasible and safe exercise training for older patients undergoing dialysis. In particular, intradialytic exercise during HD sessions can potentially enhance safety, improve adherence under the supervision of healthcare professionals, and transform sedentary dialysis time into opportunities for health promotion [99]. Similarly, for patients undergoing PD, the 2022 recommendations of the Global Renal Exercise Network and ISPD advocate the incorporation of home-based aerobic and resistance exercises, such as walking, cycling, and resistance band training, into daily routines to help prevent frailty and maintain functional independence [102].
Nutrition
Protein-energy wasting (PEW) refers to a form of malnutrition in patients with CKD characterized by an imbalance in protein metabolism, in which catabolism exceeds anabolism, leading to reduced nutritional biomarkers, body mass, and muscle mass [103,104]. The high prevalence of PEW in older patients undergoing dialysis may be attributable to nutritional loss during dialysis, chronic inflammation, inadequate dietary intake associated with aging, and multiple comorbidities [105,106].
Laboratory parameters, dietary records, and body composition measurements can be used to assess the nutritional status of older patients undergoing dialysis [105]. However, changes in body composition in this population present a significant challenge for the accurate assessments of nutritional status. Dilution caused by volume overload can affect nutritional biochemical parameters, such as serum albumin and prealbumin levels. In patients receiving PD, aging and chronic exposure to peritoneal dialysate glucose contribute to an increased proportion of body fat and reduced muscle mass as part of overall body composition. Anthropometric parameters, such as calf circumference, skinfold thickness, and waist circumference, may provide more accurate nutritional assessments than body mass index or total body weight because they better reflect muscle and fat mass. Composite nutritional indices that incorporate both subjective and objective aspects, such as Subjective Global Assessment and Malnutrition Inflammation Scores, can provide a comprehensive approach for evaluating nutritional status [107,108]. Furthermore, body composition analysis using technical devices such as bioelectrical impedance analysis or dual-energy X-ray absorptiometry may support more objective and quantitative assessments of patients undergoing dialysis [107].
Adequate dietary intake is essential for protein synthesis and regarded as a key nutritional intervention. The 2020 KDOQI guidelines for nutrition in CKD recommend 1.0–1.2 g/kg/day of protein and 25–35 kcal/kg/day of energy intake for patients undergoing dialysis, considering increased nutritional loss and catabolism associated with dialysis [107]. When these targets cannot be achieved through dietary intake alone, nutritional supplementation, such as oral, enteral, or intradialytic parenteral nutrition, should be considered [109]. A protein-rich diet contains high phosphate levels, which are associated with increased vascular calcification and mortality risks in patients undergoing dialysis [110]. However, strict phosphorus restrictions can increase the risk of malnutrition, which is particularly detrimental in older patients. Therefore, adequate protein intake combined with phosphate binders can be a practical strategy for maintaining nutritional status while controlling phosphorus levels [111].
Several age-related factors, such as cognitive dysfunction, depression, social deprivation, and functional disorders of the gastrointestinal tract, contribute to suboptimal dietary intake in older patients undergoing dialysis. Psychological and social support should be integrated into a multidisciplinary approach to enhance the effectiveness of dietary interventions. Physicians should perform comprehensive assessments and implement multifaceted strategies to improve the nutritional status of this population.
CONCLUSION
In older patients with advanced CKD, the aging process substantially affects clinical outcomes throughout the trajectory of dialysis from initiation to long-term maintenance. Age-related factors should be carefully considered when determining the timing of dialysis initiation, selecting an appropriate modality, and adjusting dialysis prescriptions. Dialysis management in older patients must evolve toward a more individualized approach, with treatment decisions guided by patient-centered goals, such as quality of life and functional preservation, rather than focusing only on biochemical treatment targets. A multidisciplinary approach and regular reassessments are essential for providing appropriate care to this vulnerable population.
SDM involving nephrologists, other healthcare professionals, patients, and caregivers should be integrated throughout the course of dialysis for older patients with ESKD. In addition, developing clinical guidelines tailored to older adults undergoing dialysis, expanding access to home-based dialysis and conservative care options, and investing in assisted dialysis infrastructure could help provide more effective and individualized care. Future research should establish standardized strategies that incorporate geriatric assessments to ensure high-quality personalized dialysis in the growing older adult population.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement table 1
Supplement table 1 Print
Print





