


A 52-year-old man was referred to the nephrology department following a health examination showing decreased renal function with proteinuria. He had no significant underlying disease except for intermittent analgesic use for back pain. Initial laboratory findings were as follows: Na+-K+-Cl--, 139-3.6-109 mmol/L; HCO3- 21mmol/L; blood urea nitrogen/creatinine, 11/1.75 mg/dL; protein/albumin, 7.0/4.4 g/dL; calcium, 9.1 mg/dL; uric acid, 1.6 mg/dL; phosphorus, 1.2 mg/dL; glucose, 79 mg/dL; HbA1c, 5.2 %.
Urinalysis revealed 3+ proteinuria 3+ glucose, with a spot urine protein/creatinine ratio of 10.5 g/g. These results indicated normal anion gap acidosis, normoglycemic glycosuria, hypophosphatemia, and hypouricemia, consistent with Fanconi syndrome (FS).
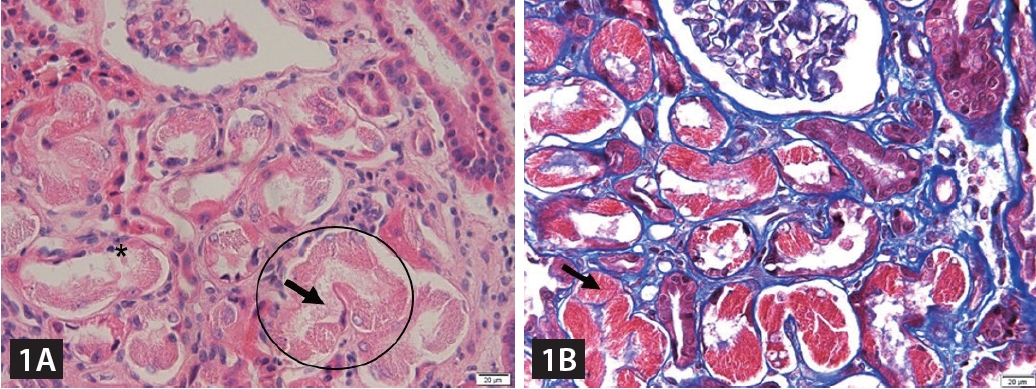
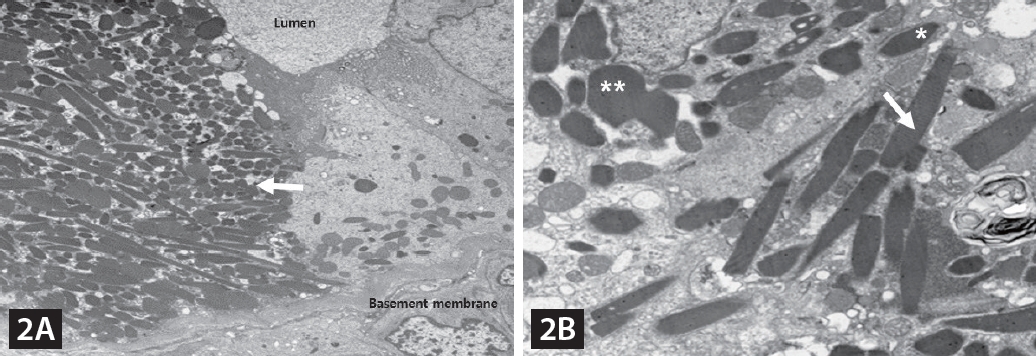
Additional blood and urine tests and kidney biopsy were performed to determine the potential causes of renal insufficiency with FS. Urine protein electrophoresis revealed an M-spike in the beta-globulin region, whereas serum immunoglobulin electrophoresis revealed an abnormal sedimentation line in the kappa region. The free kappa/lambda ratio was elevated to 1,133.86. The kidney biopsy showed abundant granular/elongated, and weakly eosinophilic crystals in the proximal tubular cell cytoplasm and the tubular lumen (Fig. 1). Ultrastructural examination clearly demonstrated electron-dense crystals with various shapes, ranging from rhomboid to pentagonal and elongated (Fig. 2). The bone marrow biopsy included 18% plasma cells, leading to the definitive diagnosis of multiple myeloma, light chain disease, kappa type.
FS is commonly caused by genetic disorders, exposure to heavy metals, or medications, but it can rarely present as a latent manifestation of light chain disease. The crystalline inclusions produced by light chains can lead to cytotoxicity in proximal tubular epithelial cells, resulting in proximal tubulopathy, whereas crystal-laden phagocytes can lead to tubular atrophy and interstitial fibrosis through tissue injury, as shown here. In patients with proximal tubulopathy accompanied by renal insufficiency and proteinuria, multiple myeloma, particularly light chain disease, should be considered in the differential diagnosis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





