


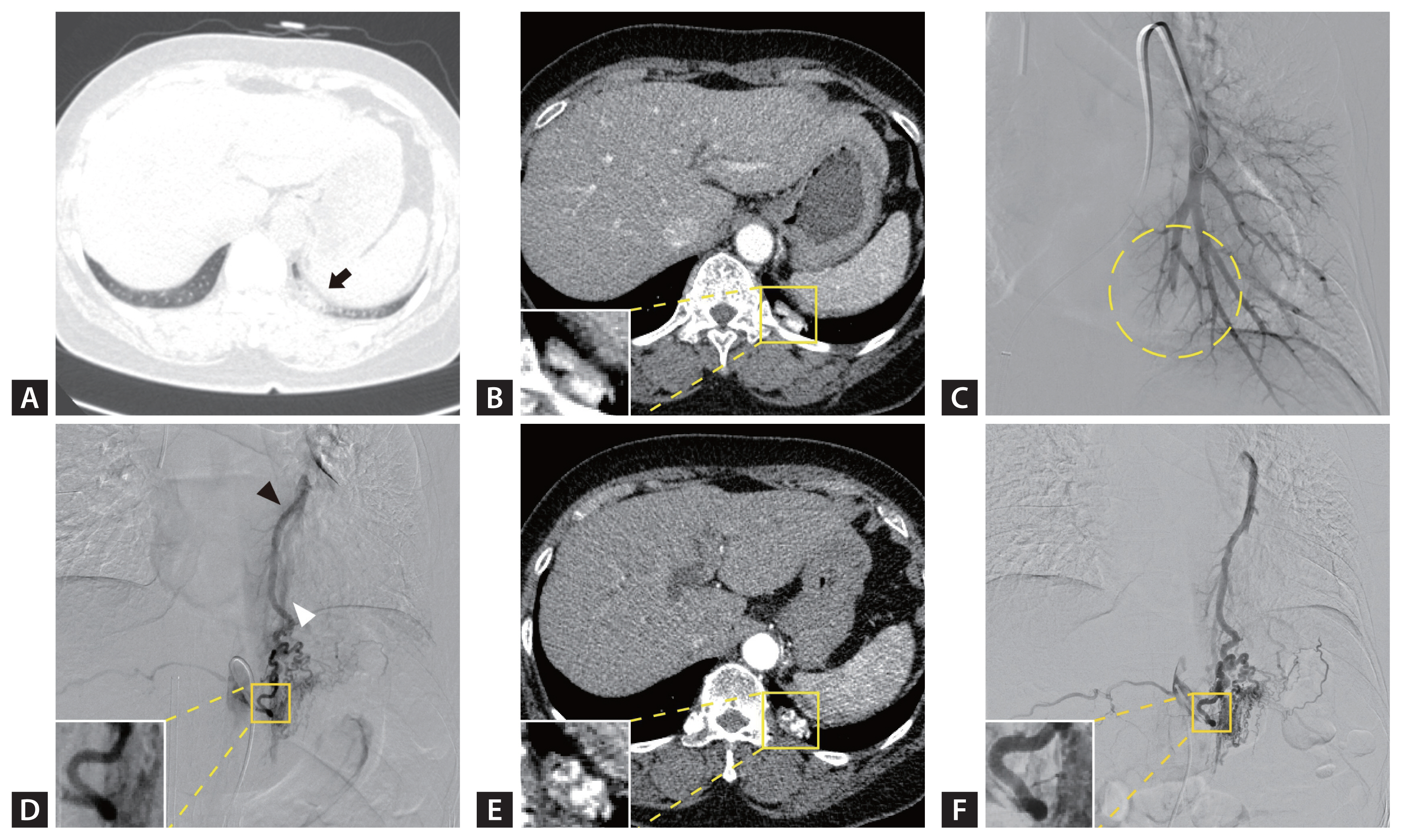
A 60-year-old woman was referred to our hospital for the evaluation of a 2.2 cm-sized focal consolidation with an air bronchogram sign incidentally detected by non-enhanced chest computed tomography (CT) (Fig. 1A). The patientŌĆÖs medical history, physical findings, and laboratory test results were unremarkable. Contrast-enhanced CT showed a well-enhanced vascular structure (Fig. 1B). Pulmonary arteriography revealed a cut-off sign in the left pulmonary artery (Fig. 1C). Aortography revealed a dilated vascular structure from the left inferior phrenic artery (IPA), and selective angiography confirmed a fistula between the left IPA and left pulmonary vessels (Fig. 1D). Because there were no apparent symptoms, the patient was discharged and scheduled for outpatient follow-up. However, she did not visit for 49 months until she was referred for persistent lesions. Contrast-enhanced CT revealed engorgement of the left IPA with a fistula (Fig. 1E), and selective angiography revealed dilatation of the feeding artery with more prominent collateral vessels (Fig. 1F). Based on these findings, transcatheter embolization of the left IPA was successfully performed. Systemic artery-to-pulmonary vessel fistula (SAPVF) is a rare vascular anomaly for which the disease course is unclear. Although most patients are asymptomatic [1], they can develop life-threatening conditions, such as hemoptysis and pulmonary hypertension [2]. Our case highlights that SAPVF can manifest as a growing chronic consolidative lesion with an air bronchogram, possibly due to dilatation of the pulmonary vessels.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




 |
 |