


INTRODUCTION
CrohnŌĆÖs disease (CD) is a chronic inflammatory gastrointestinal disorder characterized by a progressive and destructive course, leading to irreversible bowel damage and significantly impacting the patientŌĆÖs quality of life. Numerous studies have documented a shift in disease behavior over time, transitioning from initial inflammatory lesions to stricturing or fistulizing lesions that may ultimately necessitate bowel resection surgery [1ŌĆō3]. However, due to recent advancements in CD treatment, including biologics like tumor necrosis factor (TNF) antagonists, clinical outcomes have significantly improved, with reduced morbidity, hospitalization rates, and surgical interventions [4ŌĆō7].
Despite significant advances in CD treatment, uncertainties persist regarding the optimal treatment strategies, with the management of ileocecal CD being one of the most critical issues [8]. Localized ileocecal CD, characterized by disease activity confined to the terminal ileum < 30 cm with or without cecal involvement, accounts for 25ŌĆō30% of CD patients. It can be managed through either surgical or medical treatment [9,10]. Patients with inflammatory CD localized to the ileocecal area, without imminent obstruction, generally exhibit a favorable response to medical treatment, including corticosteroids. However, a significant proportion of these patients may still require surgical intervention at some point during the course of the disease, despite receiving medical treatments [11ŌĆō13]. Long-term studies have demonstrated that when a patient undergoes surgery for CD, there is a 50ŌĆō70% probability that they will not require any further surgical interventions [11,14ŌĆō16]. These findings have led to discussions regarding the advantages of early surgery compared to delayed surgery. Surgical intervention has proven to be an effective treatment strategy, providing a swift restoration of quality of life. While there is a growing interest in early surgery for ileocecal CD and several studies have been conducted [17ŌĆō19], it remains uncertain whether significant differences exist in the long-term efficacy, quality of life, and financial burdens between patients undergoing medical treatment and those opting for surgical intervention [20]. Currently, there is a lack of conclusive evidence supporting a specific strategy, and the existing guidelines primarily recommend considering surgery for ileocecal CD in cases of obstruction or when medical treatments are ineffective [21,22]. Also, there are notable distinctions in the clinical presentation and progression of CD between Eastern and Western populations, with a higher prevalence of patients in the East experiencing complicated disease [23ŌĆō25]. Additionally, there exist variations in treatment approaches between Asia and Western countries [26]. However, there is currently a dearth of data specifically focusing on Asian patients with ileocecal CD. Therefore, the objective of our study was to evaluate the long-term outcomes following primary medical versus surgical management in Asian patients newly diagnosed with ileocecal CD in the current era.
METHODS
Study population
From the cohort of patients diagnosed with CD between 1980 and 2013 and registered at Severance Hospital, we identified and included newly diagnosed ileocecal CD patients for this study. This hospital-based cohort has been enrolling patients with inflammatory bowel disease since 2006. Patients diagnosed with ileocecal CD before this time provided retrospective informed consent after their diagnosis. Meanwhile, patients diagnosed after 2006 were enrolled prospectively and provided informed consent upon diagnosis for inclusion in the entire CD cohort. Patients with a follow-up duration of less than 6 months were excluded. The assignment of patients to either the medical or surgical remission group was determined based on the initial management strategy that led to clinical remission, as decided by the treating physicians. The study was approved by the Institutional Review Board of Severance Hospital (IRB No. 4-2012-0302). Written informed consent was obtained from all patients. Patient confidentiality was maintained in accordance with guidelines from the Korean Ministry of Health, Welfare, and Family Affairs.
Definitions
Patients were diagnosed with CD based on internationally accepted criteria [9,27]. The diagnosis of CD involved evaluating various factors, including clinical presentation, endoscopic findings or surgical observations, radiology, histology, and/or serology. CD patients were classified based on the Montreal classification system, considering factors such as age at diagnosis, disease behavior, and location [28]. The extent of disease and possible strictures were assessed using endoscopic, radiological, and surgical findings. Ileocecal CD was defined as disease activity confined to the terminal ileum, with or without cecal involvement [9,28]. Stricturing disease was defined as the presence of persistent luminal narrowing accompanied by prestenotic dilatation or obstructive signs/symptoms, without evidence of penetrating disease [28]. Penetrating disease was defined as the presence of intra-abdominal fistulas, inflammatory masses, and/or abscesses [28]. Clinical remission was defined as a CrohnŌĆÖs Disease Activity Index (CDAI) < 150 without disease-related symptoms [9]. The medical remission group was defined as patients who initially received medication-based treatment and achieved their first remission through medication. The surgical remission group was defined as patients who achieved their first remission within three months after the diagnosis through ileocecal resection for ileocecal CD. Patients who were initially treated with medications but failed to achieve clinical remission and later achieved their first remission through surgery after three months were categorized as the ŌĆ£cross-overŌĆØ group and ultimately classified as part of the surgical remission group. Clinical relapse was defined as a relapse of symptoms with a CDAI score exceeding 150.
Outcome measures
The primary outcome was the cumulative relapse rate after initial remission induced by medical or surgical intervention. The secondary outcome was the cumulative rates of CD-related hospitalization and surgery following remission induced by medical or surgical means.
Statistical analysis
Baseline patient characteristics are presented as median (range) or number (%) as appropriate. The MannŌĆōWhitney test and FisherŌĆÖs exact test were used to compare characteristics between the two groups, as appropriate. Maintenance of clinical remission was estimated using the KaplanŌĆōMeier method, and the median time to relapse with its 95% confidence interval (CI) was reported. The log-rank test was employed to assess and compare the differences between the two groups.
Predictors of clinical relapse were evaluated through univariate and multivariable Cox regression analyses. Variables with p < 0.05 in the univariate analysis were included in the multivariable Cox regression analysis to identify independent predictors of relapse. Adjusted hazard ratios (HRs) and 95% CIs for the variables were also calculated. All analyses were conducted using SPSS 20.0 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
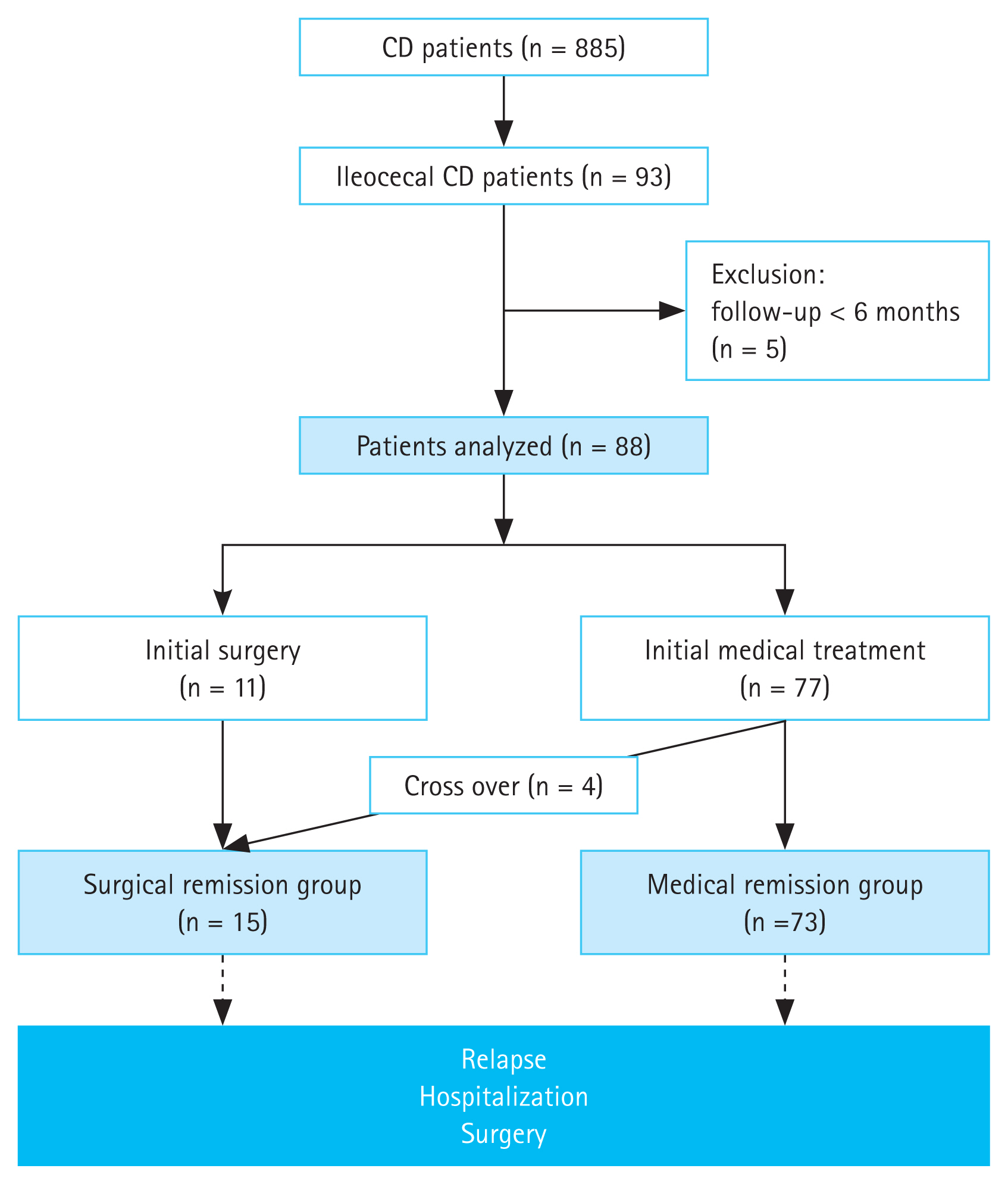
In Figure 1, a flowchart outlines the studyŌĆÖs process. Among 885 CD patients diagnosed and registered at Severance Hospital from 1980 to 2013, 93 (10.5%) were identified as having ileocecal CD. Exclusion criteria eliminated 5 patients with a follow-up period of less than 6 months. Among the remaining 88 analyzed patients with ileocecal CD, 77 initially received medical treatment, while 11 opted for surgery. Of those initially treated medically, four failed to achieve clinical remission and eventually underwent surgery, resulting in 15 patients in the surgical remission group and 73 in the medical remission group (Fig. 1). Initial steroid usage was observed in 14 (19.2%) patients in the medical remission group and 2 (13.3%) patients in the surgical remission group.
Baseline characteristics were comparable between the two groups, except that 53 patients (72.6%) in the medical remission group had inflammatory disease, while 12 patients (80.0%) in the surgical remission group exhibited stricturing or penetrating disease phenotype (p < 0.001) (Table 1).
Overall outcomes of ileocecal CD
The overall median follow-up duration after diagnosis was 6.6 years (interquartile range, 3.1ŌĆō9.9 yr). Within the medical remission group, the median follow-up time was 6.7 years (range, 0.7ŌĆō19.3 yr), while in the surgical remission group, it was 5.8 years (range, 0.7ŌĆō11.7 yr).
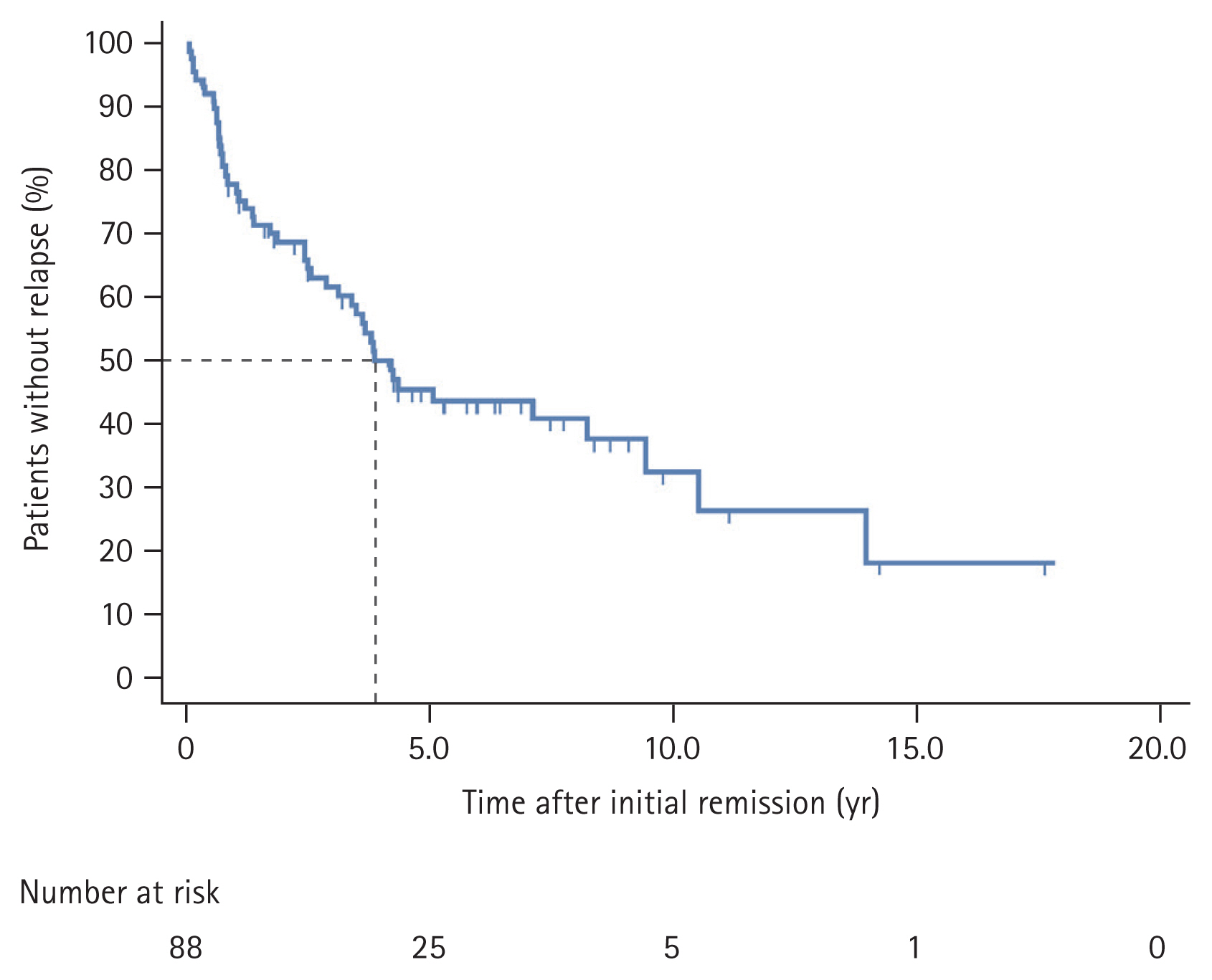
During a median follow-up of 6.6 years, clinical relapse occurred in 48 (54.5%) patients. The cumulative probability of a disease course free from clinical relapse after the first remission in overall ileocecal CD patients is presented in Figure 2. The clinical relapse rates at five and 10 years were 55.5% and 68.7%, respectively. The median time to relapse was 3.9 years (95% CI, 3.1ŌĆō4.7).
Comparison of outcomes between two groups
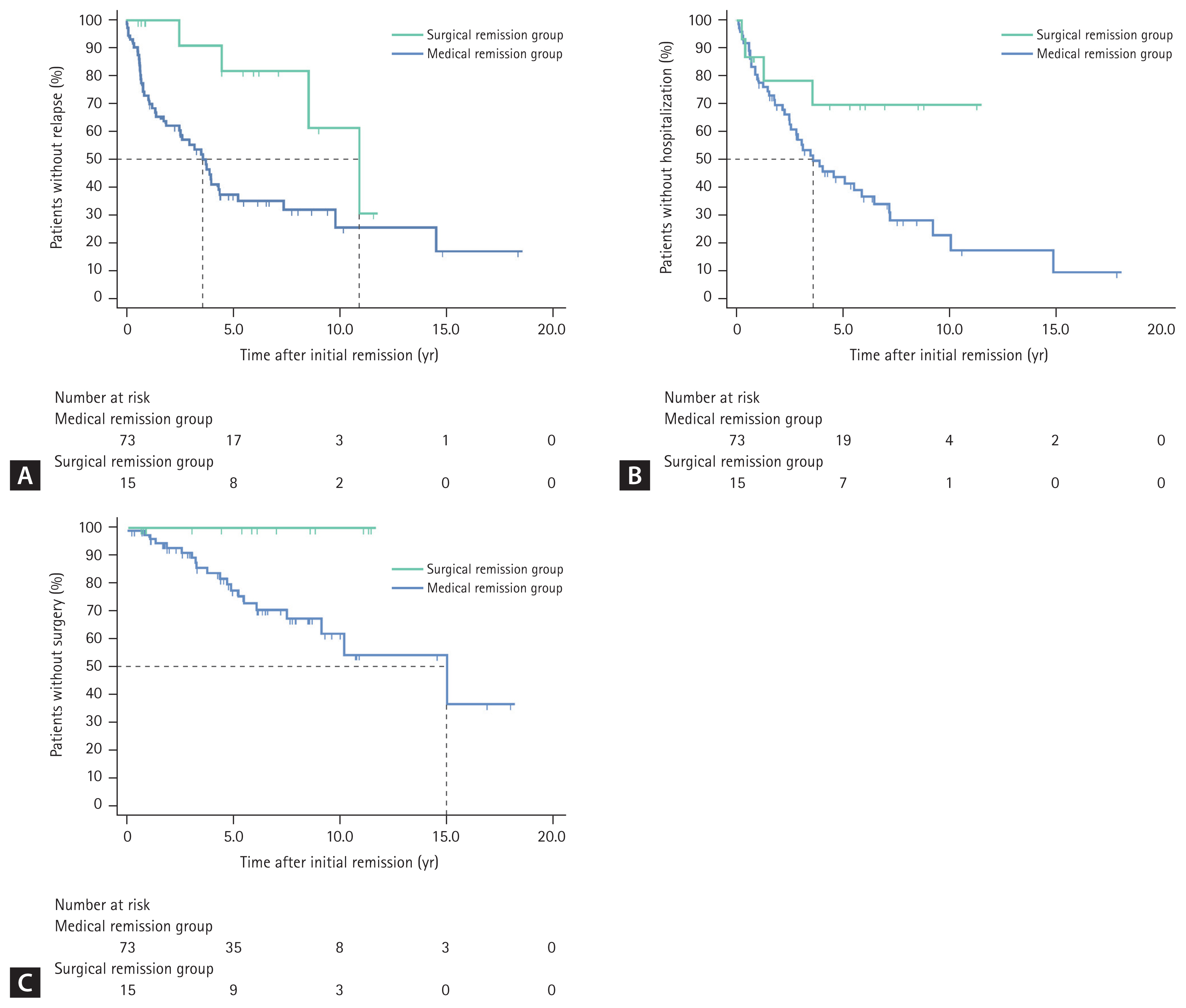
Table 2 presents the patient characteristics during the follow-up period in the two groups. In the surgical remission group, 13 out of 15 patients received postoperative prophylaxis for relapse (9 with mesalamine and 4 with azathioprine). Within the medical remission group, 20 out of 73 patients (27.4%) underwent surgery during the follow-up period. The cumulative probabilities of remaining free from clinical relapse, hospitalization, and surgery after achieving remission were analyzed using the KaplanŌĆōMeier curve (Fig. 3). A significant reduction in cumulative relapse rate was observed in the surgically induced remission group. At five years, the clinical relapse rate was 62.6% in the medical remission group, compared to 18.2% in the surgical remission group. Similarly, at 10 years, the rates were 74.4% and 38.6%, respectively. The median time to clinical relapse after initial remission was 3.7 years (95% CI, 2.6ŌĆō4.7) in the medical remission group and 10.7 years (95% CI, 7.2ŌĆō14.3) in the surgical remission group (p = 0.017) (Fig. 3A).
The cumulative hospitalization rate after the first remission was lower in the surgical remission group (Fig. 3B). At five years, the post-remission hospitalization rate was 57% in the medical remission group and 30.7% in the surgical remission group. Similarly, at 10 years, the rates were 78% and 30.7%, respectively (p = 0.054). The median time to hospitalization was 3.6 years (95% CI, 2.3ŌĆō5.0) in the medical remission group. Meanwhile, there were no instances of repeated resection after the initial surgical remission strategy, in contrast to CD-related surgery rates of 23% and 39% at five and 10 years, respectively, following initial medical treatment (p = 0.037) (Fig. 3C).
The cumulative use of immunomodulators or biologics did not differ between the two groups (p = 0.908 for immunomodulators and 0.888 for biologics) (Supplementary Fig. 1). In the surgical remission group, the use of immunomodulators to prevent post-surgical relapse was also accounted for within the category of immunomodulator usage. At five years, immunomodulators were used in 33.4% and 42.2% of the medical and surgical remission groups, respectively. Similarly, at 10 years, the rates were 63.1% and 61.5% for the medical and surgical remission groups, respectively. The median time to use of immunomodulators after initial remission was 7.7 years (95% CI, 4.5ŌĆō10.9) in the medical remission group and 8.4 years (95% CI, 1.5ŌĆō15.3) in the surgical remission group (p = 0.908) (Supplementary Fig. 1A). Regarding the cumulative use of biologics, they were noted in 3.5% at five years and 12.0% at 10 years in the medical remission group. Importantly, only one case utilized a biologic agent (anti-TNF) after 10.8 years in the surgical remission group (Supplementary Fig. 1B).
The results of both univariate and multivariable Cox regression analyses, examining potential predictors of clinical relapse, are presented in Table 3. Alongside age at diagnosis (adjusted HR, 0.94; 95% CI, 0.91ŌĆō0.98) and time to achieve first remission (adjusted HR, 1.04; 95% CI, 1.00ŌĆō1.07), the surgical remission group (adjusted HR 0.31; 95% CI, 0.10ŌĆō0.94) was identified as an independent negative predictor of clinical relapse (p = 0.039).
DISCUSSION
There are several noteworthy findings in this hospital-based cohort study, focusing on long-term follow-up of patients with ileocecal CD in a real-world setting. Overall, the outcomes for ileocecal CD were remarkably positive, with 44.5% of patients remaining symptom-free five years after achieving their first remission. Surgically induced remission exhibited significant advantages, including prolonged remission maintenance and a lower rate of clinical relapse compared to remission induced by medications. Specifically, achieving clinical remission through surgery was associated with a 69% lower risk of clinical relapse compared to medication-induced remission. These findings emphasize the favorable outcomes and benefits of surgical intervention in managing ileocecal CD.
Surgery has traditionally been viewed as a last resort treatment for CD due to potential complications or the possibility of repeated resections and short bowel syndrome. Post-operative relapse occurs in 44ŌĆō55% of patients within 10 years, requiring additional intestinal resection in 15ŌĆō50% of cases [12,29ŌĆō31]. However, surgery can be a viable alternative to long-term medical treatment for localized ileocecal CD. This is supported by evidence showing a significant cumulative probability of surgery in ileocecal CD, reaching up to 90% after 15 years [11ŌĆō13]. Long-term studies have demonstrated that once a patient undergoes surgery, there is a 50ŌĆō70% chance that they will not require any further surgeries in the future [11,14ŌĆō16]. In a study involving 181 patients who underwent ileocecal resection, only 30.9% of them required repeat resection during a median follow-up period of 14.3 years [14]. Another study, involving 139 patients with ileocecal resection, reported that 52% of them experienced disease relapse, but only 35% required additional resection after a median follow-up period of 16.4 years [11].
While long-term follow-up studies have been conducted on the clinical course of patients with ileocecal CD after surgery, there is a lack of studies focusing on the long-term outcomes of medical management. The potential long-term benefits of primary surgery compared to medical treatment, including efficacy, quality of life, and cost-effectiveness, remain uncertain. Consistent with the recommendations for general CD, current guidelines suggest considering surgery for ileocecal CD in cases involving complications, inadequate response to medical management, or medication intolerance [21,22].
Several studies investigating the potential benefits of early surgery in the treatment of ileocecal CD have focused on comparing initial surgery with surgery performed at a later stage, considering the timing of the surgical intervention [32ŌĆō35]. They demonstrated that early surgery in CD is not only safe but also associated with better clinical outcomes. Furthermore, several studies have directly compared surgery with medical treatment as the initial therapy for ileocecal CD [17ŌĆō19,36]. A randomized controlled trial (LIR!C trial) compared laparoscopic ileocecal resection versus infliximab therapy in non-stricturing and immunomodulator-refractory ileocecal CD [17]. It showed that ileocecal resection is a cost-effective treatment option with comparable quality of life to infliximab at 12 months [17,37]. Furthermore, in a retrospective long-term follow-up of the LIR!C trial with a median follow-up of 63.5 months, 26% (18 out of 69) of patients initiated anti-TNF therapy after the initial resection, while 48% (31 out of 65) of patients initially treated with infliximab underwent CD-related resection. Additionally, a recent population-based cohort study from Denmark found that primary ileocecal resection was associated with a 33% lower composite outcome (hospitalization, systemic steroid exposure, CD-related surgery, and perianal CD) compared to using anti-TNF as the initial treatment [19].
Our study is distinct from previous studies in a few ways. The national insurance system limitations led to the exclusion of anti-TNF therapy as an initial treatment for CD. Consequently, our primary medical treatment group mainly consisted of individuals using corticosteroids and immunomodulators, with only one exception who was refractory to conventional treatment. This factor may have contributed to the higher relapse rates observed in the medical remission group. Additionally, our cohort included a relatively higher proportion of patients with complicated CD (36.3%) compared to the non-stricturing cases in the LIR!C trial. However, it is important to note that our study specifically enrolled patients with newly diagnosed ileocecal CD, and most patients in the medical remission group were not refractory to medications. This suggests the potential for favorable outcomes with medical treatment in our cohort. Furthermore, as our data reflect real-world outcomes, the surgical remission group had a significantly higher proportion of patients with complicated CD compared to the medical remission group (80% vs. 27.4%, p < 0.001). Despite this, the surgical remission group exhibited fewer relapses and, similar to the LIR!C trial, no cases requiring additional surgery during the follow-up period, which adds further significance to these findings.
Early surgery in ileocecal CD offers several advantages. Firstly, it results in an improvement in the quality of life compared to prolonged disease activity and long-term medical treatment [38,39]. Secondly, performing resection early, before the development of intestinal failure, reduces post-operative morbidity and the extent of resection [14,40]. Importantly, early surgery does not increase the re-operation rate for recurrent disease and may prolong clinical remission when compared to surgery performed later in the course of the disease [11,14,32,40,41]. Also, from the patientŌĆÖs perspective, surgery is considered a viable and acceptable option [42]. However, it is important to consider the potential complications of surgery. In cases where inflammation can be effectively controlled with medications, a strategy of primary medical management followed by surgery can minimize the extent of resection and reduce complications. Therefore, it is necessary to identify the specific CD phenotype and patient characteristics associated with the benefits of early surgery. Moreover, given patientsŌĆÖ reluctance towards surgery, the importance of shared decision-making should be emphasized.
This study has notable strengths. Firstly, it is a real-world cohort study that closely followed patients with ileocecal CD for a median duration of 6.6 years to evaluate long-term outcomes after achieving remission through medical or surgical management. Secondly, as the first Asian study comparing medical and surgical approaches as initial treatments for achieving remission in ileocecal CD, our study specifically includes Asian patients with more complicated CD. Thirdly, our study establishes the index date as the date of achieving clinical remission, enabling precise evaluation of remission duration and facilitating comparisons of relapse rates.
Our study has several limitations as well. Firstly, the sample size was limited, and there was an uneven distribution between the surgical and medical treatment groups, with a larger number of participants in the medical treatment group. Secondly, the surgical intervention group had a significantly higher proportion of patients with complications. A randomized study or a propensity score matched analysis with a larger sample size is warranted. Thirdly, treatment decisions were based on individual physician judgment, introducing potential variability. Lastly, we did not conduct comparisons regarding quality of life and cost.
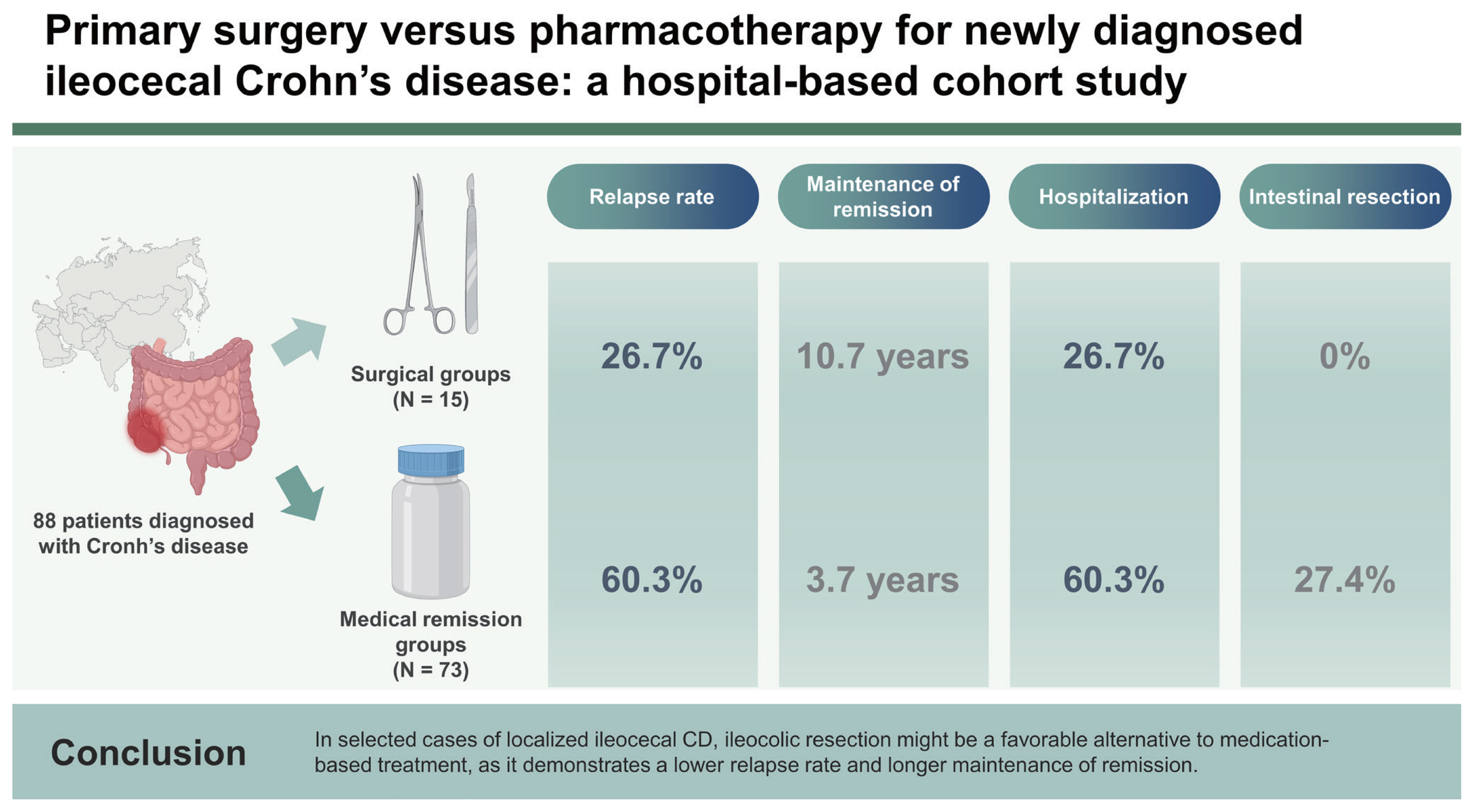
In conclusion, our study compared the long-term outcomes of primary ileocecal resection and medical management-induced remission in newly diagnosed ileocecal CD patients in a real-world setting. The results showed that surgery for achieving clinical remission resulted in a 69% lower risk of relapse compared to medication-induced remission over a 6.6-year follow-up period. Furthermore, surgically induced remission was associated with a significantly longer duration of maintaining remission compared to medication-induced remission.
These findings suggest that primary ileocecal resection could be a favorable initial treatment approach for certain patient subsets with ileocecal CD, including Asian patients. Further research is needed to investigate and identify the specific phenotype of CD and patient characteristics associated with the benefits of early surgical intervention.
KEY MESSAGE
1. The optimal timing and benefits of primary surgery compared to medical treatment in ileocecal CD remain uncertain.
2. This real-world cohort study of an Asian population with long-term follow-up found that surgically induced remission prolonged remission maintenance and reduced the risk of clinical relapse by 69% compared to medication-induced remission.
3. Primary ileocecal resection may be a favorable initial treatment for specific subsets of ileocecal CD patients, particularly Asian patients. Further research is warranted to identify the specific CD phenotype and patient characteristics that benefit from early surgical intervention.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





