


INTRODUCTION
Antimicrobial stewardship is a coordinated intervention designed to guide optimal antibiotic use in terms of the antibiotics regimen, dosing, administration route, and treatment duration [1]. Among its goals are improvement of clinical outcomes, minimization of harms such as microbial resistance and Clostridioides difficile infection, and reductions in antimicrobial consumption, cost, and adverse events. The core elements of an antimicrobial stewardship program (ASP) consist of leadership commitment, an operating system, actionable measures, tracking and reporting systems, and educational programs [2]. Interventional activities are concerned with auditing and feedback, antimicrobial restriction, authorization of antibiotic selection, dosing, treatment duration, and administration route, all of which should be based on evidence-supported guidelines. Biomarkers can serve as an objective indicator of the efficacy of these activities. This review examines the biomarkers available for antimicrobial stewardship from a physicianŌĆÖs perspective.
BIOMARKERS IN INFECTIOUS DISEASES
Biomarkers (or biological markers) are objective indicators of normal biological and pathologic processes or treatment responses [3]. They serve as diagnostic tools, support disease staging, indicate disease prognosis, predict clinical responses, and aid the monitoring of various diseases. In infectious diseases, biomarkers are used to facilitate earlier diagnoses, identify pathogens, optimize antibiotics, assess treatment responses, monitor disease progression, and stratify patients according to prognosis and risk [3,4]. Infectious disease biomarkers are divided into host-response biomarkers and pathogen-specific biomarkers. Host-response biomarkers can aid in the decision to initiate or discontinue antibiotics in patients with infectious diseases. Reducing unnecessary antibiotic exposure and overall antibiotic use can in turn reduce the duration of hospital stay, adverse events, and overall hospitalization costs.
Host-response biomarkers include procalcitonin (PCT) and C-reactive protein (CRP). PCT is a precursor of calcitonin, the hormone produced by parafollicular cells in the thyroid and by neuroendocrine cells in the lungs and intestines [5]. PCT production is upregulated hours after an increase in the levels of proinflammatory markers, including tumor necrosis factor-alpha, interleukin (IL)-1, and IL-6 [6]. PCT is widely used as a biomarker in diagnosing and predicting bacterial infections, including pneumonia and sepsis, and in measuring disease severity [6ŌĆō8]. CRP, an acute-phase reactant, is synthesized primarily by hepatocytes in response to IL-6 [9]. Increased levels of CRP occur in bacterial and other infections, as well as noninfectious causes of inflammation, and may reflect infection severity [10]. As a biomarker, CRP is used in diagnostic settings, to evaluate disease severity, and to predict outcomes of bacterial infections, including pneumonia and sepsis [11,12].
Pathogen-specific biomarkers specify the causative infectious organisms and thus support the selection of narrow-spectrum antibiotics to target the causative strain. Reducing the use of broad-spectrum antibiotics can help prevent colonization by multidrug-resistant organisms and lower the risk of adverse antibiotic effects, thereby reducing the length of hospital stays and medical costs. The classic pathogen-specific biomarkers consisted of direct antigen tests but they have largely been replaced by microbial nucleic acid methods.
BIOMARKERS IN ANTIMICROBIAL STEWARDSHIP GUIDELINES
Several guidelines refer to the role of biomarkers in antimicrobial stewardship. According to the Society for Healthcare Epidemiology of America guideline, biomarkers can be used for antibiotic discontinuation, and PCT can be used in patients in the intensive care unit (ICU) with bacterial infection or sepsis [1,13]. Japan proposed a PCT-guided algorithm as an indicator in antimicrobial stewardship [14] to evaluate whether patients with respiratory infections and sepsis should be admitted to the ICU or undergo PCT testing during the initial clinical assessment. The results showed that antibiotics can be started or stopped based on a PCT cut-off of 0.25 outside the ICU and 0.5 for sepsis.
Korea developed the first guideline for antimicrobial stewardship in 2021 [15]. The guideline states that biomarkers can be used to discontinue antibiotics. Subsequent guideline suggests a consensus algorithm for PCT use in clinical antimicrobial stewardship [16], in which antibiotics can be started or stopped based on PCT levels when an infectious disease is suspected. The cut-off for PCT is 0.5 ╬╝g/L in patients with sepsis and 0.25 ╬╝g/L in those with respiratory tract infections.
BIOMARKERS INFORMING ANTIBIOTIC USE AND DISCONTINUATION
Many patients in the ICU or wards, as well as those in outpatient settings, are suspected of having infectious diseases. Biomarkers can help determine when to start antibiotics in patients with acute respiratory infection, acute heart failure (HF), acute exacerbation of chronic obstructive pulmonary disease (COPD), acute pancreatitis (AP), pneumonia, or sepsis. Several biomarker studies have provided a reference for antimicrobial stewardship. The findings of randomized controlled trials (RCTs) evaluating the roles of PCT and CRP in antibiotic stewardship are summarized in Tables 1 and 2, respectively.
When to start antibiotics in patients with suspected bacterial infection
Sepsis: PCT
The PRORATA trial recommends measuring PCT levels at the start of antibiotics administration and 6ŌĆō12 hours after withholding antibiotics in ICU patients with sepsis. Antibiotics should be started in patients with PCT levels Ōēź 0.5 ╬╝g/L, with a strong recommendation for starting antibiotics in those with PCT levels Ōēź 1.0 ╬╝g/L [17]. For patients in the PRORATA trial, the PCT-guided group had significantly lower rates of antibiotic use than the control group (11.6 vs. 14.3 days; absolute difference = 2.7 days; 95% confidence interval [CI] 1.4ŌĆō4.1; p < 0.0001), but there was no statistically significant difference in mortality, either at 28 days (20.4% vs. 21.2%; absolute difference = 0.8%; 90% CI ŌłÆ4.6 to 6.2) or 60 days (26.1% vs. 30.0%; absolute difference = 3.8%; 90% CI ŌłÆ2.1 to 9.7).
A Belgian RCT evaluated the effectiveness of PCT-guided antibiotic treatment [18], with PCT levels measured in patients with suspected sepsis who were admitted to the ICU and started on antibiotics at a PCT Ōēź 0.5 ╬╝g/L. In the PCT-guided group, there was a higher likelihood of withholding antibiotics than in the non-PCT-guided group (46% vs. 32.7%, p = 0.15). The duration of antibiotic administration in the PCT-guided group did not differ from that in the control group (62.6% vs. 57.7%, p = 0.11), and there was no difference in antibiotic consumption between groups. The area under the receiving operating curve (AUROC) of the PCT level to differentiate infection was 0.69. However, biomarker-related studies examining when to start antibiotics in patients with suspected sepsis are limited. Overall, PCT-induced antibiotic use in sepsis was shown to significantly reduce antibiotic use but there were no improvements in clinical outcomes, including mortality.
Lower respiratory tract infection (LRTI): PCT and CRP
In the ProHOSP study, PCT was measured in patients with suspected LRTI to determine whether to administer antibiotics [19]. The PCT-guided algorithm recommended starting antibiotics in those with PCT levels > 0.25 ╬╝g/L measured within 1 hour of admission. The effectiveness of PCT-guided treatment was evaluated in patients with community-acquired pneumonia (CAP), COPD exacerbation, or acute bronchitis, in addition to the overall population. The duration of antibiotic exposure was lower in all PCT-tested patients than in non-tested patients (5.7 vs. 8.7 days; relative change, ŌłÆ34.8%; 95% CI ŌłÆ40.3% to ŌłÆ28.7%) and all subgroups. Antibiotic-related adverse events were also rarer in the PCT group. Clinical outcomes, including death, ICU admissions, and recurrence, did not differ between the two groups.
The proCAP study measured PCT before antibiotics were started in patients hospitalized with CAP and compared the results with those obtained in the usual-practice group [20]. Antibiotics were considered for patients with a PCT level Ōēź 0.25 ╬╝g/L at the time of diagnosis. If antibiotics were not administered, PCT levels were measured again after 6ŌĆō12 hours. The rate of antibiotic prescription was 85% in the PCT-guided group and 99% in the usual-practice group (p < 0.001). The clinical success rates of the two groups were similar (84% vs. 82%, p = 0.65).
A Chinese RCT evaluated PCT-guided treatment in patients with suspected CAP and recommended starting antibiotics for those with PCT levels > 0.25 ╬╝g/L [21]. If antibiotics were not started, PCT testing was repeated after 6ŌĆō12 hours. The rate of antibiotics prescription on admission was 84.4% in the PCT group, which was significantly lower than in the control group (97.5%, p = 0.004). The 4-week treatment success rate did not differ between the two groups (85.2% vs. 88.9%; absolute difference, ŌłÆ3.7; 95% CI ŌłÆ14.1 to 6.7).
Several studies have used CRP point-of-care testing (POCT) to assess the effects of prescribing antibiotics in patients with suspected respiratory tract infections in primary care settings. The IMPAC3T study in the Netherlands evaluated the effectiveness of providing general practitioners with training in communication skills and CRP POCT to aid antibiotic prescriptions [22]. The antibiotic prescription rate for suspected LRTI was significantly lower in the group trained in communication skills than in the group without training (27% vs. 54%, p < 0.01). It was also significantly lower in the group trained in CRP POCT than in the nontrained group (31% vs. 53%, p = 0.02). The GRACE (Genomics to Combat Resistance Against Antibiotics in Community-acquired LRTI in Europe) consortium evaluated the effectiveness of CRP POCT and enhanced communication skills in primary care settings [23]. Training in CRP POCT significantly reduced antibiotic prescriptions compared to the control (33% vs. 48%; adjusted risk ratio [RR], 0.54; 95% CI 0.42ŌĆō0.69). The combination of CRP POCT and enhanced communication skills resulted in significantly lower prescription rates (RR, 0.53; 95% CI 0.36ŌĆō0.74; p < 0.0001). A meta-analysis showed that CRP POCT applied to antibiotic prescriptions in primary care patients with suspected acute respiratory infection significantly reduced antibiotic prescriptions compared to controls (397 vs. 516 prescriptions per 1,000; RR, 0.77; 95% CI 0.69ŌĆō0.86).
CRP was also evaluated when LRTI was suspected in nursing home residents. The UPCARE study of nursing home populations in the Netherlands reported the effectiveness of CRP POCT when LRTI was suspected [24]. The CRP-guided group had a significantly lower antibiotic prescription rate than the control group (53.5% vs. 82.3%; hazard ratio [HR], 4.93; 95% CI 1.91ŌĆō12.73). Clinical outcomes, including the 3-week complete recovery rate, all-cause mortality, and hospitalization rates, did not differ between the groups.
Overall, PCT-guided antibiotic use reduces antibiotic exposure and antibiotic-related adverse events in patients with CAP, exacerbated COPD, or acute bronchitis. It does not improve clinical outcomes compared with controls. Similarly, CRP testing in ASPs reduces the overall number of antibiotic prescriptions but does not alter clinical outcomes, including mortality.
COVID-19: PCT and CRP
COVID-19 guidelines do not address the use of biomarkers in antibiotic stewardship, nor does The National Institute for Health and Care Excellence recommend the routine use of PCT for antibiotic stewardship in COVID-19 patients [25].
In a multicenter observational study performed in the Netherlands, PCT-guided antibiotic treatment significantly reduced antibiotic prescriptions in patients with COVID-19 [26]. Among patients admitted with COVID-19, antibiotics were considered in the PCT-guided group when the PCT level measured within 24 hours after admission was Ōēź 0.25 ╬╝g/L. The rates of 1-week antibiotic administration (26.8% vs. 44.7%, p < 0.001) and total antibiotic administration (35.2% vs. 54.5%, p < 0.001) were lower in the PCT-guided group than in the usual care group. The rates of 30-day mortality, 90-day mortality, hospital stay, and ICU admission also differed between the two groups.
In the UK, ASPs include the measurement of PCT in patients admitted to the hospital with SARS-CoV-2, with antibiotic discontinuation considered in those with a PCT level < 0.25 ng/L [27]. PCT contributed to antibiotics discontinuation in 32% of patients and reduced the antibiotic prescription rate from 70% to 36.5%. A retrospective cohort study also performed in the UK evaluated the effectiveness of antimicrobial stewardship and recommended antibiotic discontinuation in COVID-19 patients with a PCT level Ōēż 0.25 ng/mL measured within 48 hours of hospitalization [28]. In the PCT-negative group, the median duration of antibiotic use was shorter than in the PCT-positive group (2 vs. 5 days, p < 0.001), as was the defined daily dose (DDD) (0.14 vs. 0.37, p < 0.001). Patients in the PCT-negative group were three times less likely to be treated with carbapenem than were those in the PCT-positive group. The PCT-negative group had lower rates of mortality (28% vs. 36%, p = 0.021) and ICU admission (9% vs. 19%, p = 0.007) than the PCT-positive group.
In a single-center retrospective study performed in the UK, PCT was evaluated according to the presence or absence of secondary bacterial infection in patients with COVID-19 who were admitted to the ICU [29]. Median PCT levels did not differ between patients with and without secondary bacterial infection (0.18 vs. 0.235, p > 0.05). Median CRP and white blood cell (WBC) levels also did not differ between these groups.
A retrospective study performed in Belgium, which enrolled patients with COVID-19 who had been admitted to the ICU, examined the association of PCT measured within 48 hours of hospital admission with bacterial co-infection [30]. The AUROC for PCT as a predictor of bacterial co-infection was 0.68 but that for 30-day mortality was 0.77, with significant differences between survivors and non-survivors. PCT was shown to be a biomarker of COVID-19 severity rather than bacterial co-infection. In other studies, PCT was associated with COVID-19 severity, disease progression, and mortality, regardless of bacterial co-infection [31ŌĆō33]. Measuring PCT levels in patients with COVID-19 may help determine whether antibiotics should be initiated for bacterial co-infection, but the levels may also be elevated in patients with severe COVID-19. Clinical decisions should therefore be based on clinical features or other biomarkers.
No RCT has evaluated the role of CRP alone in antimicrobial stewardship. A retrospective study reported AUROC values for CRP and PCT of 0.86 (p < 0.001) and 0.88 (p < 0.001), respectively, in predicting secondary bacterial infection in patients with COVID-19 [34]. Another study of COVID-19 patients suggested that PCT levels should be measured heterogeneously in those with high CRP values. In the PCT < 0.5 ng/mL group, a low CRP had a negative predictive value and predicted hospital admission in 97.6% of cases. CRP determination in this setting can be used as a supplementary biomarker to PCT [35].
PCT and CRP may not be increased in COVID-19 patients treated with dexamethasone and tocilizumab, even in those with a secondary bacterial infection [36]. PCT is an indicator of infection severity; it cannot be used to discriminate between bacterial and viral infections. Overall, PCT-guided antibiotics in COVID-19 patients can result in a decrease in antibiotic use. While PCT has limited accuracy in diagnosing bacterial co-infection in COVID-19 patients, bacterial co-infection can be diagnosed by measuring CRP in combination with PCT.
Exacerbation of COPD/asthma: PCT and CRP
Antibiotics are frequently prescribed to treat exacerbated COPD or asthma, as the symptoms are similar to those of pneumonia. A multinational RCT evaluated the role of PCT in the decision to start antibiotics in patients with exacerbated COPD [37]. Antibiotics were recommended for those with PCT levels > 0.25 ╬╝g/L, with a repeat PCT measurement performed after 6ŌĆō24 hours if antibiotics were withheld. The PCT-guided group had a significantly lower rate of antibiotic prescriptions than the group receiving standard therapy (40% vs. 72%, p < 0.0001). Neither clinical outcomes nor an improvement in the forced expiratory volume in one second at 14 days and 6 months differed between the two groups.
A Swiss RCT evaluated the effectiveness of PCT-guided antibiotic administration in patients with suspected LRTI in a COPD subgroup [38]. In the PCT-guided group, administered antibiotics if their PCT level was Ōēź 0.25 ╬╝g/L, the antibiotic prescription rate was significantly lower than in the standard-of-care group (38% vs. 87%, p = 0.001). COPD exacerbation and hospital readmission rates did not differ between the two groups. A meta-analysis evaluated the effectiveness of PCT-guided antibiotic administration (both antibiotic initiation and discontinuation) in patients with exacerbated COPD [39]. The results showed a lower antibiotic prescription rate (RR, 0.56; 95% CI 0.43ŌĆō0.73) among patients with PCT guidance but no difference in clinical outcomes, including hospital stay, exacerbation of the recurrence rate, and mortality, compared to the control group.
A multicenter RCT performed in the UK evaluated the effectiveness of measuring CRP POCT in patients with exacerbated COPD. Antibiotics were administered to those with CRP levels Ōēź 20 mg/L [40]. The CRP-guided group had a lower antibiotic prescription rate than the control group (57.0% vs. 77.4%; adjusted odds ratio [OR], 0.31; 95% CI, 0.20ŌĆō0.47). The total Clinical COPD Questionnaire score at 2 weeks was also lower in the CRP-guided group (ŌłÆ0.19 points; 90% CI, ŌłÆ0.33 to ŌłÆ0.05). A prospective observational study performed in the UK measured PCT and CRP levels in patients with exacerbated COPD or asthma and suspected pneumonia [41]. The AUROCs of CRP and PCT for distinguishing pneumonia from COPD exacerbation were 0.96 and 0.93, respectively. At a CRP cut-off for starting antibiotics of > 48 mg/L, the sensitivity for pneumonia diagnosis was 91%, and the specificity was 93%. Overall, PCT- and CRP-guided antibiotic use reduced overall antibiotic exposure, without differences in hospital stay, recurrent exacerbation, or mortality, in patients with COPD/asthma exacerbation.
Acute HF: PCT
Patients with acute HF may show symptoms and X-ray abnormalities similar to those of patients with pneumonia. Biomarkers can help determine whether antibiotics, which are commonly misused in acute HF, are warranted. The BACH trial evaluated the role of biomarkers in differentiating between pneumonia and noninfectious diseases, such as COPD and acute HF, in patients who visited the hospital with dyspnea [42]. The AUROC for diagnosing pneumonia based on PCT alone was 0.723 (p < 0.0001), which was higher than that of WBCs (0.69). When PCT and clinical signals, including X-ray findings, were evaluated together, the AUROC for the diagnosis of pneumonia increased to 0.863. Among patients with acute HF and a PCT level > 0.21 ng/mL, 5.1% were diagnosed with pneumonia, and 33% required antibiotic treatment during follow-up. Antibiotics were not administered to 32% of the patients with a PCT > 0.5 ng/mL, which indicates limitations of diagnosing bacterial co-infection in patients with acute HF based solely on biomarkers such as PCT.
In the large cohort of HF patients in the PROTECT study, the characteristics of those with a PCT > 0.2 ng/mL (high-PCT) or < 0.2 ng/mL (low-PCT) were compared with those of patients with acute HF and bacterial infection [43]. In the high-PCT group, there was a statistically significant association of a high PCT level with lower serum albumin and hemoglobin levels, and with higher WBC, CRP, and blood urea nitrogen levels, suggesting an association of a high PCT level with bacterial infections in patients with HF. Despite the similar severity of HF between the two groups, the high PCT group had a higher 30-day all-cause mortality risk (HR, 2.3; 95% CI 1.3ŌĆō4.2; p = 0.005). Overall, PCT was shown to have limited accuracy for diagnosing bacterial infection in patients with acute HF, given that it can also increase with increasing overall mortality.
Infective endocarditis (IE): PCT and CRP
A prospective cohort study performed in Switzerland evaluated the roles of PCT and CRP as diagnostic biomarkers in patients with suspected IE [44]. The AUROCs for PCT and CRP in the diagnosis of IE were 0.856 and 0.657, respectively. When the PCT cutoff for IE diagnosis was set to 2.3 ng/mL, the sensitivity was 81%, and the specificity was 85%. The study also included infections other than IE. However, PCT was highest in patients with IE (median, 6.56 ng/mL), followed by non-IE bacterial infection (median, 1.06 ng/mL) and viral infection (median, 0.07 ng/mL). The median PCT value in patients with IE caused by Staphylococcus aureus was higher than that in patients with S. aureus sepsis (median, 4.81 vs. 1.06 ng/mL; p = 0.021).
In a meta-analysis of the roles of PCT and CRP in diagnosing patients with suspected IE [45], the AUROCs of PCT and CRP for the diagnosis of IE were 0.71 and 0.80, respectively, indicating a higher accuracy of CRP than PCT. The PCT cut-off values in several studies were 0.19ŌĆō0.64 ng/mL, and the CRP cut-off value was 10.6 mg/L. The role of biomarkers in the diagnosis of IE is thus limited, and the cut-off values that distinguish bacterial IE from nonbacterial endocarditis remain poorly defined. Overall, PCT and CRP have no clear role as biomarkers in the diagnosis of IE, although the levels of both biomarkers tend to be higher in patients with IE than in those with other bacterial infections.
Acute coronary syndrome (ACS)/cardiac arrest: PCT
The role of biomarkers in distinguishing bacterial co-infection in patients with acute myocardial infarction or cardiac arrest is limited. PCT was measured in patients with ACS and cardiogenic shock. Virtually all patients with cardiogenic shock, 33% of those with ST-elevation myocardial infarction, and 8% of those with non-ST elevation myocardial infarction/unstable angina had PCT levels > 0.5 ng/mL [46]. In another study, the PCT levels of patients with ACS without complications were mostly < 0.5 ╬╝g/L, but they increased to 5.24 ╬╝g/L in patients with cardiac arrest, cardiogenic shock, or concomitant bacterial infection, suggesting an elevated PCT during systemic inflammatory responses [47]. Several studies have examined the role of biomarkers in differentiating bacterial infection from cardiovascular disorders in patients with dyspnea, but the evidence supporting their use remains limited [48]. Further research is warranted to determine the role of biomarkers in patients with ACS/cardiac arrest.
Acute pancreatitis: PCT
The proCAP study was an RCT conducted in the UK that evaluated the effectiveness of a PCT-guided algorithm recommending antibiotic administration for patients with AP and PCT levels Ōēź 1.0 ng/mL [49]. The algorithm also recommended discontinuation of antibiotics for those with PCT levels < 1.0 ng/mL on days 4 and 7 after admission. The PCT-guided algorithm reduced antibiotic prescriptions compared to the usual care group (45% vs. 63%; risk difference [RD], ŌłÆ15.6%; 95% CI ŌłÆ27.0 to ŌłÆ4.2; p = 0.0071). All-cause mortality and hospital-acquired infection rates did not differ between the two groups.
Another study, conducted in Singapore, evaluated the effectiveness of PCT-based guidelines in patients with AP [50]. The guidelines recommended measuring PCT in patients with severe AP and starting antibiotics in those with PCT levels Ōēź 0.5 ng/L. If PCT decreased every other day, antibiotics were recommended for 10ŌĆō14 days. The PCT-guided group had a significantly shorter antibiotic duration than the standard-of-care group (3.3 vs. 6.3 days, p < 0.001), while clinical outcomes, including 30-day mortality, were similar. A meta-analysis indicated that PCT can aid in the diagnosis of severe AP, but not bacterial co-infection, in patients with AP (AUC, 0.89; sensitivity, 0.80; specificity, 0.84) [51]. Overall, PCT-guided antibiotic use in AP patients significantly reduced antibiotic use, with no improvement in clinical outcomes, including mortality.
When to stop antibiotic administration
Sepsis: PCT, CRP, and presepsin
The PRORATA trial recommended stopping antibiotics if PCT levels decrease from their peak concentration by Ōēź 80% or are < 0.5 ╬╝g/L [17]. PCT-guided treatment at antibiotic initiation and discontinuation in acutely ill patients in the ICU reduced the duration of antibiotic administration. However, the 28- and 60-day mortality rates did not significantly differ compared to the control group. The SAPS trial recommended measuring PCT daily and stopping antibiotics in patients with a PCT level Ōēż 0.5 ╬╝g/L or Ōēż 20% decrease compared to the baseline [52]. The duration of antibiotic administration was shorter in the PCT-guided group than in the standard-of-care group (6 vs. 7 days, p = 0.0001).
The PROGRESS trial recommended stopping antibiotics in sepsis patients with PCT levels Ōēż 0.5 ╬╝g/L or with a Ōēź 80% reduction after treatment day 5 [53]. In that study, PCT-guided antibiotic cessation shortened the antibiotic treatment duration compared to the control group (5 vs. 7 days, p < 0.001), with better results in the former with respect to infection-associated adverse events (7.2% vs. 15.3%, p = 0.045), 28-day mortality (15.2% vs. 28.2%, p = 0.02), and hospitalization costs.
In a multicenter RCT performed in the Netherlands, PCT was measured daily in critically ill patients with suspected sepsis who were started on antibiotics. Antibiotic treatment was discontinued if PCT levels were Ōēż 0.5 ╬╝g/L or decreased by 80% from their peak level [54]. In the PCT-guided group, antibiotic use was shortened compared to the standard-of-care group, from 7 to 5 days, and median antibiotic consumption was reduced from 9.3 to 7.5 DDDs. The 28-day mortality rate was lower in the PCT-guided group than in the standard-of-care group (20% vs. 27%, p = 0.0122). CRP and PCT were measured in that study, and no significant differences in CRP levels were found between the two groups.
In the SISPCT trial, a PCT-guided algorithm was applied in patients with severe sepsis or septic shock [55]. PCT was measured at baseline and on days 4, 7, 10, and 14. Antibiotic discontinuation was recommended in patients with PCT levels Ōēż 1.0 on day 7 and in those with a > 50% decrease on day 4. The duration of antibiotic administration in the PCT-guided group did not differ from that in the control group at day 7, but antibiotic exposure in the former was reduced by 4.5%. The 28-day mortality rate did not differ significantly between the two groups (25.6% vs. 28.2%, p = 0.34).
An RCT conducted in Germany evaluated the effectiveness of PCT-guided antibiotic therapy in patients with sepsis admitted to surgical ICUs [56]. Antibiotic discontinuation was recommended when the PCT level, measured upon the improvement of clinical symptoms, was < 1 ng/mL or had decreased by 25ŌĆō35% from the initial level over 3 days. The duration of antibiotic administration was shorter in the PCT-guided group than in the standard-of-care group (5.9 vs. 7.9 days, p < 0.001). Neither the daily Sequential Organ Failure Assessment (SOFA) score nor the CRP or IL-6 levels differed significantly between the two groups.
A meta-analysis of 15 studies found that PCT-guided antibiotic management in critically ill patients reduced antibiotic use by 1.26 days and short-term mortality by 13% [57]. A prospective cohort study conducted in Canada evaluated an ASP, including a biomarker-guided clinical decision support system [58]. PCT was measured daily in ICU patients with sepsis who were receiving antibiotic treatment. Antibiotics were discontinued in those with a PCT level < 0.25 ng/mL or a 90% decrease from the baseline level. Antibiotics were continued if the PCT level was > 1 ng/mL or increased over time. The PCT-guided antibiotic management system reduced overall antibiotic use by 7.3% (p = 0.010), with no difference in hospital mobility, clinical outcome, or length of ICU stay compared to the control.
A Brazilian RCT of ICU patients receiving antibiotic treatment for sepsis evaluated the effectiveness of an algorithm for stopping antibiotics if the baseline CRP level on day 3 or 5 was < 35 mg/L or there was a > 50% decrease in the CRP level [59]. The duration of antibiotic use was 1 day shorter in the CRP-guided group than in the control group (6 vs. 7 days, p = 0.011) whereas the 28-day mortality rate (28.1% vs. 22.7%, p = 0.480) and ICU mortality rate (18.8% vs. 18.2%, p = 0.933) were not significantly different.
Another multicenter RCT study conducted in Brazil compared PCT- and CRP-guided antibiotic treatment at the time of antibiotic discontinuation in patients with sepsis [60]. Antibiotic discontinuation was recommended on treatment day 4 or 5 in those with PCT levels < 0.1 ng/mL and a 90% decrease from baseline, as well as CRP levels of < 25 mg/L or a 50% decrease from baseline. The median duration of antibiotic therapy was shorter in the CRP group than in the PCT group (6 vs. 7 days, respectively, p = 0.06), with no differences in 28-day mortality (33.3% vs. 32.7%, respectively, p = 1.000) or hospital mortality (46.7% vs. 42.9%, respectively, p = 0.836).
An Egyptian RCT compared the decision to discontinue antibiotics in patients with sepsis who were admitted to the ICU based on PCT versus CRP levels on days 4 and 7 [61]. The cut-off for antibiotic discontinuation was a PCT level < 0.5 ng/mL or a Ōēź 80ŌĆō90% decrease from baseline, and a CRP level < 8.7 mg/L or a Ōēź 50% decrease from baseline. The antibiotic discontinuation rate on day 4 was 6% in the CRP-guided group and 23% in the PCT-guided group (p = 0.07), and the antibiotics saving after antibiotic discontinuation on day 4 was 6 days in the CRP group and 30 days in the PCT group (p = 0.005). The 28-day mortality rate was 65.2% in the CRP-guided group and 34.8% in the PCT-guided group (p = 0.063).
Presepsin, a novel biomarker in antimicrobial stewardship, is a soluble form of CD14 with a broad-spectrum affinity for the innate immune system that has been shown to support pathogen recognition [62,63]. Presepsin levels begin to increase 2 hours after infection and peak 3 hours later, suggesting a role for presepsin as an early biomarker for sepsis diagnosis [64]. A multicenter prospective cohort trial conducted in China evaluated the effectiveness of presepsin for antibiotic discontinuation in patients with sepsis [65]. Presepsin levels were measured at baseline and every other day. In the presepsin-guided group, discontinuing antibiotics was recommended in patients with presepsin levels < 350 pg/mL or a Ōēź 80% decrease from the peak level measured twice consecutively. The number of days without antibiotics was higher in the presepsin-guided group than in the control group (14.64 vs. 11.00 days, p < 0.001), with no difference in mortality between the two groups either at 28 days (17.7% vs. 18.2%, p = 0.868) or 90 days (19.9% vs. 19.5%, p = 0.891).
Overall, PCT- and CRP-guided antibiotic discontinuation reduces overall antibiotic exposure without improving clinical outcomes such as mortality. Presepsin-induced antibiotic discontinuity was shown to reduce overall antibiotic use but also did not impact clinical outcomes, including mortality.
LRTI: PCT and IL-1╬▓/IL-8
The above-mentioned ProHOSP study also evaluated the effect of PCT-guided antibiotic management on antibiotic discontinuation in patients with LRTI [19]. PCT was measured on days 3, 5, and 7 of antibiotic treatment. Antibiotics were discontinued in patients with PCT levels Ōēż 0.25 ╬╝g/L or a Ōēź 80% decrease from the peak level. The PCT-guided group had significantly reduced antibiotic use compared to the control group. There were no differences in mortality compared to the CAP, exacerbated COPD, and acute bronchitis subgroups.
The ProCAP study also evaluated the PCT-guided clinical decision to discontinue antibiotics in patients with CAP [20]. PCT was measured on days 4, 6, and 8, with antibiotic discontinuation recommended in patients with PCT levels < 0.25 ╬╝g/L or a 10% decrease in the baseline PCT level Ōēź 10 ╬╝g/L. The median duration of antibiotic use was 7 days shorter in the PCT-guided group than in the control group (5 vs. 12 days, p < 0.001). In subgroup analysis, the duration of antibiotic use in the PCT-guided group was significantly shorter in patients with mild CAP, severe CAP, or nonbacterial CAP (all p < 0.001). The clinical success rates were similar between the PCT-guided and control groups (84% vs. 82%, p = 0.65).
In the Chinese RCT discussed above, PCT-guided clinical decision-making regarding the discontinuation of antibiotics was evaluated in patients with CAP [21]. PCT was measured on days 3, 6, and 8, and antibiotics were discontinued in patients with PCT levels < 0.25╬╝g/L. The total antibiotic exposure risk was 1.8 times higher, and the median duration of antibiotic use was 2 days longer, in the control group than in the PCT-guided group. Four-week clinical outcomes were similar between the two groups.
The ProVAP study evaluated the role of PCT in patients with ventilator-associated pneumonia (VAP) [66]. The recommendations called for a discontinuation of antibiotics in patients with PCT levels < 0.5 ╬╝g/L or a decrease from baseline of > 80% at 72 hours after treatment initiation. PCT was measured daily for 10 days in VAP patients maintained on antibiotics. The PCT-guided group had significantly more antibiotic-free days (13 vs. 9.5 days, p = 0.049) and a 27% decrease in the overall duration of antibiotic treatment compared to the control group (10 vs. 15 days, p = 0.038). Mechanical ventilation-free days, ICU-free days, length of hospital stay, and 28-day mortality did not differ significantly between the two groups.
The effectiveness of PCT-guided treatment in terms of the discontinuation of antibiotics was evaluated in a Japanese RCT that included patients with aspiration pneumonia [67]. PCT was measured on days 3, 5, and 7 after antibiotics were started, with discontinuation of antibiotics in patients with PCT levels Ōēż 0.5 ng/mL or a > 90% decrease from peak levels. The PCT-guided group had a median reduction of antibiotic duration of 3 days compared to the control group (5 vs. 8 days, p < 0.001). Clinical outcomes, including pneumonia relapse (21% vs. 23%, p = 0.80) and in-hospital death rates (10% vs. 21%, p = 0.26), were not significantly different between the two groups.
The VAPrapid2 study evaluated the effectiveness of IL-1╬▓/IL-8-guided treatment in patients with VAP [68], following a study that identified IL-1╬▓/IL-8 as a VAP marker [69]. Antibiotic discontinuation was recommended for patients whose IL-1╬▓/IL-8 levels, measured in bronchiolar lavage fluid, were below the cutoff. There was no difference in antibiotic-free days or clinical outcomes, including SOFA score and mortality, between the IL-1╬▓/IL-8-guided group and the control group. However, the low compliance rate of the IL-1╬▓/IL-8 induction group may have been a limitation. Further studies are needed to explore this relationship.
Overall, PCT-guided antibiotic discontinuation reduces overall antibiotic use in patients with CAP, exacerbated COPD, acute bronchitis, VAP, or aspiration pneumonia, without affecting clinical outcomes including mortality.
Febrile neutropenia: PCT
The ProfenC study evaluated the effect of PCT antimicrobial stewardship in children receiving cancer chemotherapy without bone marrow recovery and with a low-risk of febrile neutropenia [70]. Antibiotic cessation was recommended in those with PCT levels < 0.25 ng/mL, measured 48 hours after antibiotic use. PCT-based clinical decision-making significantly reduced antibiotic use (3 vs. 7 days, p < 0.001), with no differences in treatment failure compared to the control group.
REAL-WORLD DATA
Different results may be obtained in real-world clinical practice than in clinical trials. A study in Switzerland thus applied the ProHOSP study algorithm to actual clinical practice [19,71], in which there were more patients with renal disease, cancer, or immunosuppression. Pneumonia severity and CAP rates were higher among real-world patients than in the ProHOSP cohort. The median duration of antibiotic use following the application of PCT-guided antimicrobial stewardship in the real-world group was 6 days, which was 2 days longer than in the PCT group from the ProHOSP study (p = 0.08) and 1 day shorter than in the control group (p < 0.048). Adverse events, including mortality, ICU admission, recurrence, and disease-specific complications, were similar to those of the ProHOSP study (all p > 0.05).
According to a before-and-after analysis of PCT-guided antibacterial management conducted in Germany, PCT-guided ASP reduced antibiotic use density in the surgical ICU by 21.2% (1,005 in 2010 vs. 791.9 DDDs in 2012) [72]. However, while the use of aminoglycosides, cephalosporins, and quinolones decreased, carbapenem use slightly increased, suggesting a limited impact of PCT-guided ASP on antibiotic selection.
A study conducted in the USA evaluated the cost-effectiveness of applying the PRORATA studyŌĆÖs PCT-guided algorithm to patients with suspected bacterial infection or sepsis who were hospitalized in the medical ICU [17,73]. PCT-guided antibiotic treatment significantly reduced antibiotic duration and hospital costs to $45 per patient and increased the quality-adjusted life-years by 0.0001. The economic advantage of biomarkers was exemplified by a total annual hospital cost saving of $8,480.
In another study conducted in the USA, based on the Premier Healthcare Database, 78% of 933,591 adult patients with sepsis underwent biomarker testing [74]. The PCT group had more severe illness and more antibiotic exposure than the other biomarker groups. Patients who had been PCT-tested twice or more had higher hospital costs than those not tested for biomarkers. However, the groups tested for PCT once (OR, 0.88; 95% CI 0.85ŌĆō0.91) or at least twice (OR, 0.64; 95% CI 0.85ŌĆō0.91) had a lower risk of death than the group not tested for biomarkers. CRP and lactate testing did not result in a difference in the OR. Consecutive PCT testing was associated with decreased mortality, but it did not reduce hospital costs.
Thus, the use of biomarkers for antimicrobial stewardship in real-world patients with sepsis and LRTI can reduce the duration of antibiotic use without worsening outcomes. However, issues related to antibiotic choice and medical costs remain controversial.
PHYSICIANSŌĆÖ PERSPECTIVES
Currently, biomarkers are used in ASP to determine when to start antibiotics in patients with suspected bacterial infections and when to stop antibiotics in treated patients. There is sufficient evidence from ASPs that PCT testing can be used alone. CRP testing has limitations with respect to informing the decision for antibiotic initiation or discontinuation when used alone, but it can be effective when combined with PCT.
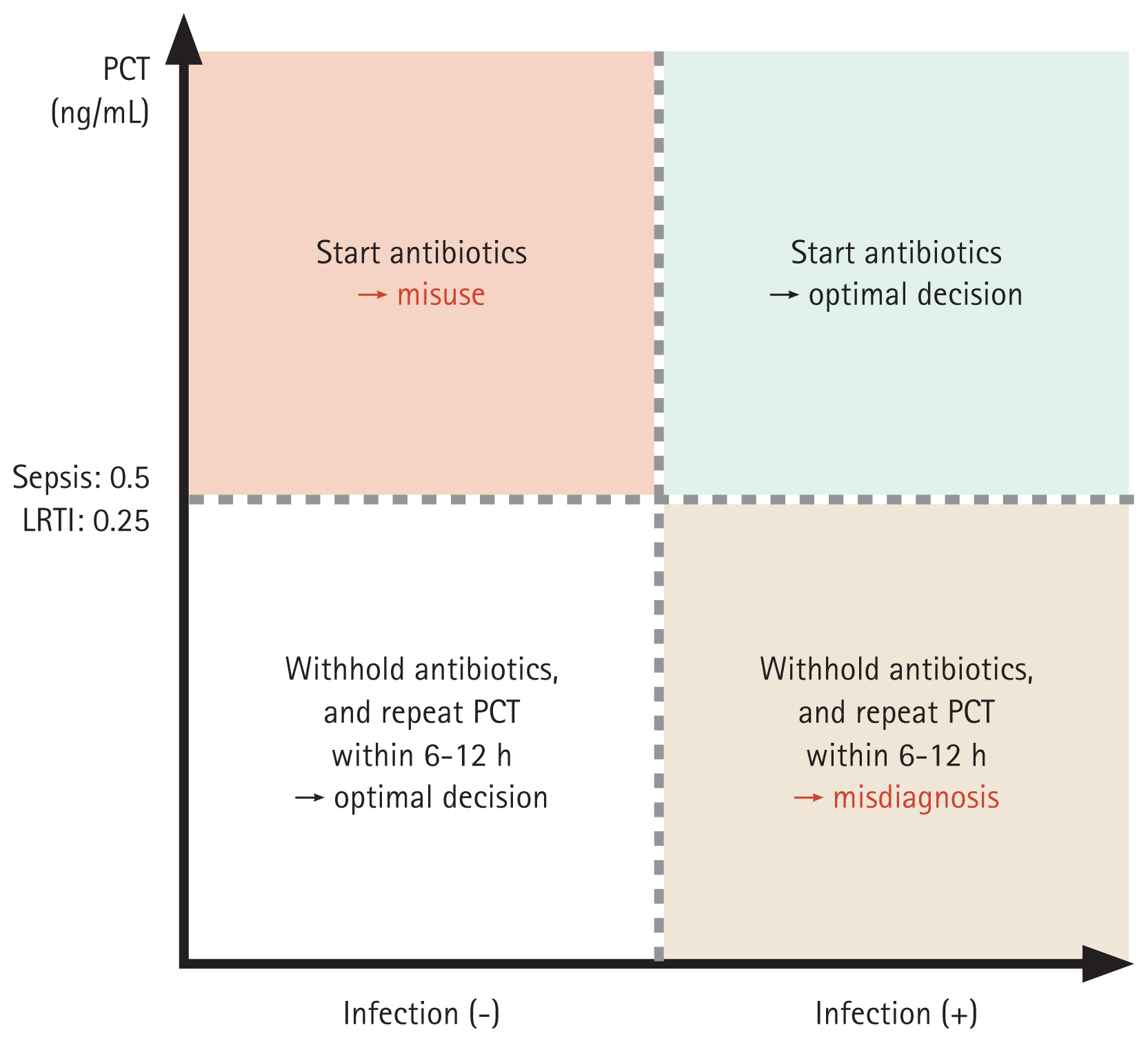
PCT testing cannot be applied in the management of all bacterial diseases, but it is relevant regarding the decision to initiate/discontinue antibiotics in sepsis and LRTI. When discriminating between non-infectious organ failure (formerly systemic inflammatory response system) and sepsis, patients who meet the diagnostic criteria for sepsis and have PCT levels Ōēź 0.5 ng/mL can be started on antibiotics. If LRTI is suspected, the cut-off for initiating antibiotics is 0.25 ng/mL. However, PCT-guided antibiotic initiation may lead to antibiotic misuse and misdiagnosis (Fig. 1). To reduce the likelihood of misdiagnosis, PCT levels should be measured again within 6ŌĆō12 hours; to reduce the risk of antibiotic misuse, a clinician may decide to not administer antibiotics even if the PCT criteria are met. If antibiotics are maintained, short-term PCT measurements are needed before treatment discontinuation.
PCT-guided antibiotic discontinuation is recommended in patients with PCT levels < 0.5 ng/mL (< 0.25 ng/mL in LRTI) or a decrease of Ōēź 80% in their peak PCT level. PCT should be measured 5ŌĆō7 days after antibiotic administration begins. If the levels do not meet the antibiotic discontinuation criteria, they can be measured again after 2 days. In Korea, unjustified PCT measurements may not be covered by insurance, which can increase costs. Furthermore, while biomarkers can provide objective evidence in universal ASPs, their use should never take precedence over a clinicianŌĆÖs judgment.
GAPS AND FUTURE DIRECTIONS IN CLINICAL RESEARCH
Several research gaps regarding biomarkers and antimicrobial stewardship remain. Most studies have focused on reducing the total amount or duration of antibiotics. However, the purpose of antimicrobial stewardship is not only to reduce antibiotic use but also to identify patients who need antibiotics and administer the appropriate drug in a timely manner. Further studies on biomarkers are needed to support clinical decision-making as it pertains to empirical antibiotic selection and to shed light on the role of microbiological biomarkers. Microbiological biomarkers based on classical antibody measurements are of low sensitivity, and recent PCR techniques do not distinguish colonizers from pathogens. Further research on microbiological biomarkers should focus on the rapid discrimination of pathogens. The combination of novel microbiological biomarkers and existing host-response biomarkers will provide objective evidence for ASP and reduce the likelihood of clinical misjudgment.
CONCLUSIONS
Biomarkers are increasingly being applied in antimicrobial stewardship, especially to inform the decision of when to start or stop antibiotics for various infectious diseases. The most commonly used biomarker is PCT. The cut-off values of PCT for sepsis and pneumonia are 0.5 and 0.25 ng/mL, respectively. A clearly defined role for other host-response and pathogen-specific biomarkers in antimicrobial stewardship is still lacking. Future studies on these biomarkers are warranted to inform antimicrobial stewardship in a broader array of diseases.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





