


INTRODUCTION
The cough reflex is a vital physiological mechanism to clear unwanted material from the lungs and prevent aspiration [1]. Cough is regulated by coordinated interaction between the airway sensory nerves, brainstem and higher brain regions, enabling effective removal of irritants from the lower airways [2]. However, following a respiratory viral infection, the cough reflex may become sensitized, leading to irresistible bouts of coughing triggered by exposure to relatively innocuous stimuli [3]. In most cases, post-viral cough settles after a few weeks although it may take longer to resolve [4,5].
Chronic cough, defined as a cough persisting for more than 8 weeks, is a clinical condition which can be difficult to treat and has received widespread clinical attention in recent years [6-10]. It is common in the community, affecting approximately 10% of the general adult populations worldwide, and approximately 2% to 5% in Asia Pacific countries including Korea [11-13]. Its higher prevalence among the elderly suggests that the burden of chronic cough may potentially continue to increase [14]. Although not directly related to mortality, chronic cough impacts a range of daily activities causing significant impairment of quality of life (QoL), frequently leading to social isolation of affected individuals [15-18].
The development of what was termed the “anatomic diagnostic protocol,” which advocated systematic evaluation of potential causes based on the anatomical distribution of the vagal afferent sensory nerves regulating cough, was the first clinical breakthrough to improve the management of patients with chronic cough [19]. Earlier studies reported that almost all patients with chronic cough could be successfully managed using this systematic approach [19,20]. However, later clinical experience did not match the initial optimism, as 10% to 40% of patients visiting referral clinics remain unexplained or refractory to currently available treatments [21]. This unmet clinical need led to the revised outlook of the pathophysiological mechanisms underlying chronic cough [22,23]; and in 2014, a new paradigm of cough hypersensitivity syndrome (CHS) was proposed by the European Respiratory Society (ERS) Task Force [24]. CHS is defined as “a clinical syndrome characterized by troublesome coughing often triggered by low levels of thermal, mechanical, or chemical exposure” [24], reflecting symptom profiles described by many patients. Many patients with chronic cough report triggering of coughing by trivial environmental or behavioral factors such as exposure to cold or dry air, perfumes and aerosols, talking on the phone, or eating crumbly food (termed allotussia) [25-27]. The term ‘CHS’ also reflects what is now considered the principal underlying pathophysiological mechanism namely, cough reflex hypersensitivity [28]. Based on recent neurobiological studies, inflammation-induced injury causing functional changes of the neural pathways are suggested to lead to the sensitization of the cough reflex and perhaps its persistence [3].
The validity of this new concept is supported by a number of promising early phase clinical trials with antitussives targeting the neuronal pathways responsible for cough [29-32]. In addition, with help of sophisticated cough measurement tools, imaging techniques and mechanistic studies, we are gaining more understanding of the pathophysiology of chronic cough or CHS [3,33-35], although these advances are also giving rise to more new questions. In this review, we provide an overview of recent progress in this field, with a focus on major mechanistic studies and clinical trials. We also discuss current knowledge gaps and future application of concepts discussed to clinical practice.
INSIGHTS FROM RECENT MECHANISTIC STUDIES
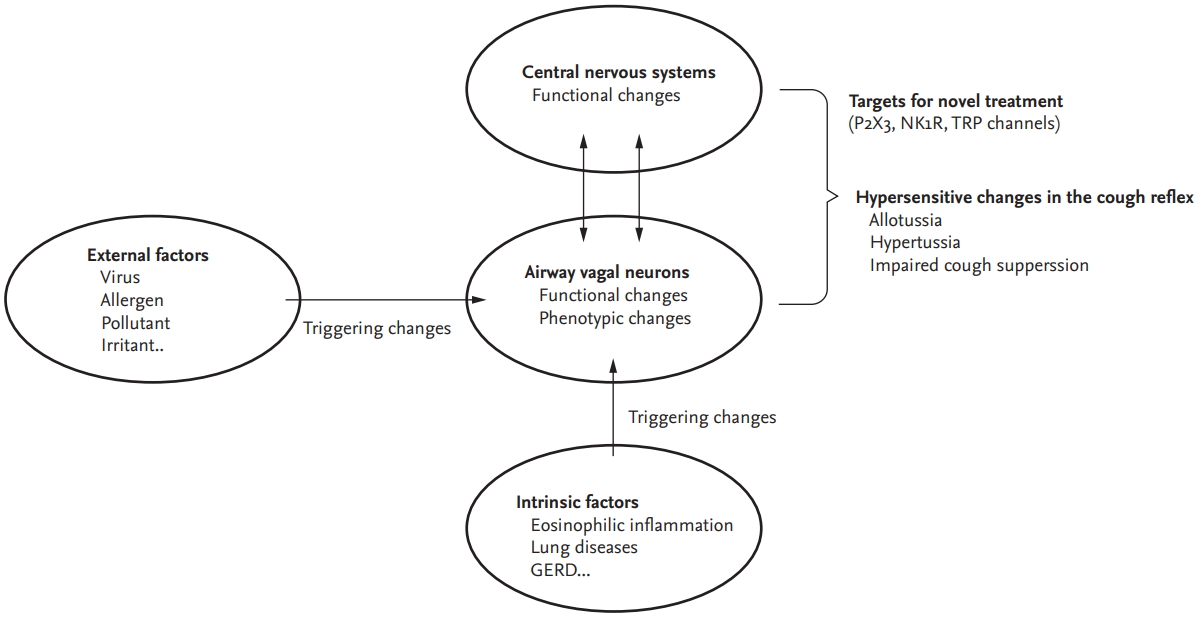
Functional or phenotypic changes in peripheral sensory neurons may be the first-level adaptive host responses in terms of developing cough reflex hypersensitivity. A wide variety of external and internal triggers, such as viral infection, allergens, eosinophils, air pollutants or subsequent airway inflammation, may induce a functional hypersensitive status in the cough reflex, accompanied by functional or phenotypic changes in neurons (Fig. 1).
Clinically, respiratory viral infection is a common cause of cough [36] and may enhance capsaicin cough sensitivity [37]; and mechanistically, the viral infection or inflammatory sequelae may induce functional changes in sensory neurons [38]. In in vitro experiments using human rhinovirus and IMR-32 neuroblastoma cell lines differentiated into sensory neuron phenotypes, there is evidence that the virus infects the neuronal cells and rapidly upregulates the expression of transient receptor potential channel vanilloid-1 (TRPV1) and ankyrin-1 (TRPA1) implicated in cough induced by chemical and physical irritants [38]. In guinea pig experiments, parainfluenza-3 virus infection led to enhanced cough sensitivity to capsaicin, citric acid, and bradykinin, and upregulated gene expression of TRPV1 in the vagal ganglia [39].
Similar functional and phenotypic changes in airway sensory neurons were also observed in experimental models of allergic inflammation. In ovalbumin-sensitized guinea pigs, ovalbumin challenge induced de novo TRPV1 gene expression in tracheal nodose ganglionic neurons [40]. Eosinophils may directly induce cough hypersensitivity, probably through their cationic proteins; eosinophil major basic proteins directly enhanced chemical and mechanical sensitivity of pulmonary afferent C-fibres in rats and also induced cough sensitivity to irritants in mice [41]. In a study of human asthmatics, the number of airway and blood eosinophils correlated with the length of airway nerves and the number of nerve branch points [42]. In addition, in another study of allergic asthmatics, allergen inhalation challenge significantly increased capsaicin cough responses and also spontaneous coughs over 24 hours in allergic asthmatics, compared to diluent inhalation (negative control) [43]. Cigarette smoke extracts or particulate matter 2.5 may also provoke similar changes in the airway nervous systems, although precise effects may differ between stimuli [44-46].
In humans, inhalation tussigen challenge tests are utilized to assess cough reflex sensitivity and may reveal enhanced cough responses (termed hypertussia) in patients with chronic cough. Commonly used agents include capsaicin, citric acid, distilled water, or adenosine triphosphate (ATP) and protocols for inhalation cough challenge testing and the use of the C2 or C5 endpoints (i.e., the concentration of tussigen causing two or five cough respectively) have been standardized [47]. Within individuals, capsaicin cough sensitivity increases during respiratory viral infection [37], and it also decreases by the resolution of coughing [48]. However, the tests are currently utilized for research purposes rather than for their clinical value due to their poor discriminatory ability between cough patients and healthy subjects contrasting the utility of bronchoprovocation challenge testing with agents such as methacholine or histamine [47]. In a recent study using ATP cough challenge tests, patients with chronic cough showed heightened cough response at lower concentration of ATP than healthy controls; however, the difference between groups was small [49].
The limited value of existing cough challenge testing has led to consideration of alternative challenge endpoints. In a nonlinear mixed-effects pharmacodynamic modeling study by Hilton et al. [50], recording the maximal cough response evoked by any concentration of capsaicin (Emax) appeared to better discriminate chronic cough patients from healthy controls than conventional C2 and C5 endpoints. The study also suggested that a failure of descending inhibitory pathways might be a discriminating feature between patients with chronic cough and healthy controls [50]. This notion was supported in a recent study comparing the ability to voluntarily suppress cough in response to capsaicin inhalation; patients with chronic refractory cough were significantly less capable of suppressing cough than healthy controls [51].
Clinical value of cough challenge test is still uncertain. However, using different endpoints (such as Emax [50]) or a modified study protocol (such as cough suppression test [51]), it may contribute to discover the mechanisms underlying chronic cough. Capsaicin cough responses have been recently used as a proxy for neuronal sensitization in characterizing asthmatic patients [52,53]. In addition, by applying different tussigens, it may help confirm the mechanisms of novel antitussives [54,55], or explore the heterogeneity of cough hypersensitivity across individuals [56].
Brain functional magnetic resonance imaging studies may help identify the central neuronal processes responsible for chronic cough. In studies by Ando et al. [57], using low level concentrations of inhaled capsaicin, just sufficient to induce the “urge to cough,” patients with chronic cough exhibited lower levels of activation in cortical regions implicated in cough inhibition (dorsomedial prefrontal and anterior mid-cingulate cortices) than healthy subjects.
INSIGHTS FROM RECENT CLINICAL TRIALS WITH NOVEL PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENTS FOR CHRONIC COUGH
Successful outcomes in the treatment with opioids, gabapentin or pregabalin, support the notion that patients with chronic refractory cough may benefit from neuromodulatory treatments [29-31]. However, the relatively modest efficacy of these agents and the disabling side effects have hampered widespread use and prompted the search for more suitable cough treatments.
Since capsaicin, the active ingredient of chili pepper, is a well-known tussigen triggering the TRPV1 pathway, pharmacological inhibition of the TRPV1 pathway has gained scientific interest. However, clinical trials with two potent TRPV1 antagonists (SB-705498 and XEN-D0501) failed to reduce cough frequency or improve cough-specific QoL, while they significantly inhibited cough responses to capsaicin [55,58]. TRPA1 is a receptor sensing cold temperature (< 17°C) and a wide range of irritants including acrolein, allyl-isothiocyanate, or cinnamaldehyde which are abundant in air pollutants and cigarette smoke [59]. In humans, cold air is one of the most common triggers for coughing and TRPA1 stimulation was shown to mediate cough [60]. However, the only TRPA1 antagonist to date having undergone early phase clinical development failed in a placebo-controlled trial of patients with chronic refractory cough [61]. This series of disappointments with specific TRP antagonists have galvanized the efforts to identify alternatives targeting other sensory neuronal receptors as potential antitussives [35].
ATP is a major damage-associated molecule released during cellular injury and which activates purinergic receptors. There are different subtypes in P2X receptors according to their tissue or cellular distribution; P2X3 receptor is located primarily on peripheral neurons, thus making it a promising therapeutic target in neuropathic conditions [62]. Remarkably, in a proof-of-concept study of patients with chronic refractory cough, a P2X3 antagonist, AF-219 (now called gefapixant), showed dramatic effects on objective cough frequency, cough severity, and cough-specific QoL [32], suggesting that P2X3 receptor is an integral part of the cough hypersensitivity pathway. Meanwhile, almost all patients developed taste disturbance during the treatment [32], which is now attributed to be the inhibition of P2X2/3 channels by a high dose of gefapixant (600 mg twice a day). Thus, in two subsequent dose-ranging studies, different dosages of gefapixant were tested to optimize the efficacy and tolerability, which found that gefapixant at a lower dosage (30 or 50 mg twice a day) may be appropriate for subsequent trials [63].
The success of P2X3 antagonists has led to the question of whether P2X3 is a single key molecule that regulates cough reflex hypersensitivity in chronic cough. However, inhalation of ATP did not cause a dramatic shift in cough sensitivity [49], suggesting that it may be merely a link in the chain rather than the driving engine of cough hypersensitivity [35]. Bonvini et al. [64] hypothesized a possible upstream regulator of ATP-P2X3 pathways and suggested a potential role of TRPV4 in regulating ATP-P2X3 in airway sensory neurons. However, a double-blind placebo-controlled clinical trial with a TRPV4 antagonist, GSK2798745, in patients with chronic cough showed negative results (ClinicalTrials.gov Identifier: NCT03372603). Thus, clinical relevance of TRPV4 remains to be further elucidated.
In a recent randomized placebo-controlled trial with gefapixant, inhalational cough challenge tests were sequentially performed with different tussigens such as ATP, capsaicin, citric acid, and distilled water [54]. Notably, gefapixant showed no effect on capsaicin and citric acid-induced coughs, while it significantly reduced cough sensitivity to ATP and distilled water. These findings suggest at least two distinct pathways in cough sensitivity; one mediated by purinergic pathways (responding to ATP and distilled water) with others independent of purinergic signals.
Larger clinical trials with gefapixant as well as other P2X3 selective antagonists (BAY1817080, BLU-5937, and S-600918) will finally confirm clinical roles of P2X3 antagonists in the management pathways of chronic cough. However, P2X3 may not be the sole pathway responsible for refractory cough, because gefapixant was not effective in some patients [32]. Also, it had no significant antitussive effects in patients with idiopathic pulmonary fibrosis (IPF)-associated cough [65]. In contrast, inhaled sodium cromoglycate, a mast cell stabilizer, was ineffective in controlling chronic refractory cough but improved IPF-associated cough [66]. Meanwhile, orvepitant, a neurokinin-1-receptor (NK1R) antagonist, showed benefits with improving subjective cough outcomes in patients with refractory cough [67], suggesting another therapeutic target in chronic cough. These altogether lead us to consider the heterogeneity in the mechanisms of chronic cough.
Heterogeneity in cough sensitivity was also shown in a recent study using cough challenge tests; patients with chronic obstructive pulmonary disease (COPD) showed enhanced cough sensitivity to capsaicin but a reduced response to prostaglandin E2 (PGE2) compared to healthy controls, while patients with chronic cough had heightened cough response to capsaicin, citric acid, and PGE2 [44]. These findings collectively indicate that there are likely heterogeneous processes underlying cough hypersensitivity across different patients and clinical conditions, and that that deciphering the heterogeneity would be key in developing the precise tools to control refractory cough. It is anticipated that the NEUROCOUGH Clinical Research Consortium, a multidisciplinary pan-European initiative endorsed by ERS [68], will provide the opportunity for precise phenotyping and molecular endotyping of chronic cough patients across a range of respiratory diseases, and thus, help generate further insights into the disease pathophysiology.
Meanwhile, non-pharmacological cough control therapy, or speech language and pathology therapy, is now considered a promising option for patients with chronic refractory cough, as demonstrated by randomised controlled trials [69,70]. The protocol is tailored for individual patient’s traits, but briefly, its key components include education, cough control techniques, vocal hygiene and hydration, and psychoeducational counselling. Notably, it has essentially no side effects and may have sustained therapeutic benefits (up to 3 months’ observation in a recent study [70]), when undertaken by professionals. With these strengths, in the coming years, its indication may extend to other chronic cough phenotypes than refractory cough; however, its efficacy and safety still needs to be proven in different cough phenotypes. Also, importantly, the service should be provided by experienced professionals. At present, the pool of individuals qualified for speech language and pathology therapy is lacking in many countries including Korea.
NEW CONCEPTS TO CONSIDER IN THE EVALUATION AND MANAGEMENT OF CHRONIC COUGH
While it is important to note that key principles of the anatomic diagnostic protocol remain valid, new approaches to the evaluation and management of cough are needed. To date, the key focus in controlling cough has centered on treating conditions such as asthma, rhinitis, or gastroesophageal reflux disease (GERD). However, placebo-controlled studies indicate that true therapeutic benefits gained from treating these conditions may be much less than the findings suggested from observational studies [71,72]. Cough is frequently self-limiting and prone to placebo effects [73], which may underlie the large discrepancy between placebo-controlled and uncontrolled (observational) studies.
An alternative to empiric trials of medicines, typically prescribed in a sequential manner is to take an approach based on identifying potential treatable traits [8], of which are worthy of consideration (Fig. 2).
Eosinophilic airway inflammation is a common feature of cough variant asthma and a defining characteristic of and eosinophilic bronchitis, which together may comprise up to 50% of chronic cough patients [74]. There is a controversy over direct causal effects of eosinophilic inflammation on cough, as anti-interleukin-5 monoclonal antibody, mepolizumab, did not affect cough while systemic corticosteroids did in patients with severe eosinophilic asthma [75]. However, it is much less arguable that eosinophilic airway inflammation is a treatable trait in chronic cough, because it is measurable in induced sputum and may predict corticosteroid responsiveness. Thus, the assessment and management of eosinophilic airway inflammation is recommended during the early stages of diagnostic work-up for chronic cough at specialist clinics [6,9,20,75]. However, there are practical issues in measuring eosinophilic airway inflammation, as induced sputum analysis is technically demanding and therefore restricted to specialist centers. Consequently, there is interest in developing practical alternatives to induced sputum tests, such as fractional exhaled nitric oxide (FeNO) measurement [76,77]. In a meta-analysis of observational studies, FeNO showed a promising utility in predicting the diagnosis of cough variant asthma, with specificity of 0.85 (95% confidence interval [CI], 0.81 to 0.88) and sensitivity of 0.72 (95% CI, 0.61 to 0.81) [76]. However, it showed a relatively poor predictability for sputum eosinophilia in patients with asthma or chronic cough [76,77]. In placebo-controlled trials, high FeNO levels were significantly associated with good corticosteroid responsiveness in patients with respiratory symptoms including cough [78,79]; however, it is unclear whether these findings could be directly translated into patients with isolated chronic cough. So far, there is no quality evidence to make strong recommendations for the routine use of FeNO in patients with chronic cough [8]. It is our view that in time, FeNO will emerge as an important treatable trait to consider in patients referred with chronic cough.
Obstructive lung diseases, such as asthma or COPD, are frequently associated with cough, and bronchodilators are the main therapeutic options (often in combination with inhaled corticosteroid [ICS]). Methacholine-induced bronchoconstriction may increase capsaicin cough responses in asthmatics [80]. However, the roles of bronchodilator therapy in managing chronic cough remain largely unclear. To our knowledge, most clinical trials of bronchodilator therapy in patients with asthma or COPD have not utilized validated cough measurement tools and rarely report cough endpoints. A small number of trials have suggested of the efficacy of treating airway obstruction in patients complaining chronic cough. In a placebo-controlled trial of 15 patients with chronic cough, treatment with an inhaled bronchodilator was effective in reducing cough severity score in a subset of asthmatic patients with cough [81]. In patients with chronic productive cough and COPD, a combination of ICS and salmeterol showed some improvements in cough scores compared to placebo, but the inter-group difference in cough score was relatively small and difficult to translate clinically [82]. Importantly, further studies are warranted to confirm whether airway obstruction is a major treatable trait in chronic cough.
GERD has been a controversial entity in terms of clinical relevance to cough. Systematic reviews of placebo-controlled trials demonstrated that acid suppressive therapy such as proton pump inhibitor (PPI) showed almost no benefits over placebo in cough patients without acid reflux (therapeutic gain; range, 0.0% to 8.6%), and only modest therapeutic gains in patients with pathologic acid reflux (range, 12.5% to 35.8%) [71]. These findings support the notion that a routine anti-acid therapy is not indicated but should be reserved for a subgroup with symptoms of acid reflux and/or evidence of pathological acid reflux on diagnostic testing; this view has been reflected in recent guideline recommendations [8,9,83]. Indeed, the relationships between cough and reflux are likely to be complex, as cough can frequently induce reflux and reflux can also provoke cough (thus can be self-perpetuating) [84]. PPI is generally safe, but there are potential concerns about adverse drug reactions problematic in the elderly, such as iron deficiency, vitamin B12 deficiency, hypomagnesemia, osteoporosis-related bone fracture, dementia, or pneumonia [14]. Although direct reports are sparse, there is a concern that PPI is being frequently prescribed without a clear rationale in subjects with chronic cough [85].
Meanwhile, recent studies suggest potential implications of non-acid reflux in chronic cough [84,86,87]; however, there are no controlled trials with prokinetics or reflux inhibitors in patients with chronic cough. Thus, further studies are warranted to confirm if non-acid reflux is clinically relevant to chronic cough.
Rhinitis or rhinosinusitis is one of the conditions that has been most frequently associated with chronic cough, particularly in Asia [13,88]. In a previous survey of physicians in Korea, upper airway cough syndrome was perceived as the most common cause of chronic cough and paranasal sinus radiography was one of the most frequently considered diagnostic tests [89]. However, mechanistically, it does not directly trigger cough via vagus nerves, while nasal inflammation may sensitize the cough reflex through activation of trigeminal nerves [90]. In an observational study of 89 subjects with purulent post-nasal drip, approximately 9% of them complained of cough, in the absence of lung diseases [91]. In a recent study, patients with chronic post-nasal drip showed significantly decreased nasopharyngeal sensitivity to air puff instillation than healthy controls [92]. In addition, to our knowledge, there is no placebo-controlled trial to confirm the benefits of second-generation H1-antihistamines or intranasal corticosteroids in patients with chronic cough and nasal symptoms, using validated outcomes for cough. Thus, further works are warranted to determine whether nasal inflammation is a treatable trait in chronic cough.
Laryngeal dysfunction is likely to be common in patients with chronic refractory cough [93], which is not surprising given the protective role of the larynx for the lower airways. However, precise roles of laryngeal dysfunction have not been confirmed in chronic cough [94]. Two observational studies suggested the potential benefit of gabapentin therapy for cough patients with abnormal motion of the larynx [95,96]. In clinical experience, it is suggested that speech language and pathology therapy including breathing technique education may be beneficial in chronic cough patients with comorbid laryngeal dysfunction [97]. Controlled trials with the measurement of laryngeal behavior will help understand and confirm the clinical relevance of laryngeal dysfunction in chronic cough.
Chronic cough in children is beyond the scope of the present review. However, certain etiologies of chronic cough in children are considered distinct from those in adults [98]. Common causes in children may differ between regions and clinical settings, but commonly include protracted bacterial bronchitis (PBB), tracheomalacia, bronchiectasis, asthma and post-infectious cough [8]; these findings are attributed to structural or immunologic maturation processes affecting the cough reflex pathways are occurring in childhood. Amongst various conditions, PBB is considered to be a distinct common entity in infants and young children with chronic wet cough [99]. The prevalence of PBB is not reported in Korean children, but the data from Australia, Turkey, and China indicate that it is one of the most common causes of chronic wet cough in young children [99-101]. In the recent ERS Task Force report, a consensus definition has been formulated as the following: (1) presence of chronic (> 4 weeks’ duration) wet or productive cough; (2) absence of symptoms or signs (i.e., specific cough pointers) suggestive of other causes of wet or productive cough; and (3) cough resolved following a 2 to 4-week course of an appropriate oral antibiotic [99]. Recent international and domestic guidelines commonly recommend a trial of antibiotics therapy in young children with chronic wet cough, normal chest X-rays, normal spirometry, and no warning signs [8,9,102]. Meanwhile, it is unknown whether a clinical entity like PBB exists in adults. However, a recent observational study in United Kingdom described that a cohort of adult patients with chronic productive cough and sputum neutrophilia who had been unexplained by existing disease labels but showed a significant response to a 3-month azithromycin treatment [103].
Cough hypersensitivity is becoming more measurable and controllable [32,47,49,63,67,69,70], and thus it may be considered as a treatable trait in chronic cough. However, this concept is still reserved for adults with chronic refractory cough (Fig. 2). It is usually considered that chronic cough without identifiable organic or anatomical causes is uncommon in children [98].
In summary, there are very few practical biomarkers that have been found to be useful in identifying a treatable trait or predicting a specific treatment response. As previously discussed, while there are no proven alternatives to induced sputum tests in defining eosinophilic airway inflammation or predicting ICS response, FeNO is likely to have an increasing prominent role. The clinical utility of methacholine bronchial challenge tests is unclear in predicting ICS treatment response among patients with isolated chronic cough, as non-asthmatic eosinophilic bronchitis is relatively commonly associated with chronic cough [20,88,104]. Heartburn symptoms are considered a biomarker to guide acid suppressive therapy [8,9,83]; however, the value of this symptom biomarker may be limited [105]. There are no biomarkers to guide H1-antihistamine therapy in chronic cough patients. Therefore, current clinical approaches are mostly based on therapeutic trials and further work is necessary to develop a precise clinical strategy for chronic cough [8].
CONCLUSIONS
In the last few decades, there have been important advances in the clinical and scientific understanding of cough. Importantly, the concept of CHS has been introduced, and it is gaining widespread endorsement within the allergy and respiratory community. There are now increasing numbers of successful clinical trials with novel antitussives and speech language pathology therapy, which is a very welcome news to patients with refractory cough and the clinicians. Central to this has been an appreciation of the neurobiology of cough; however, significant gaps in knowledge exist and new challenges are emerging on a regular basis particularly regarding clinical translation of exciting preclinical entities. In addition, there is a pressing need to educate clinicians and health care providers as to the importance of chronic cough as a common clinical condition that hampers the lives of patients. There is currently a real sense of optimism in this field and, in order to realize the potential of the remarkable progress in clinical evaluation and drug discovery, there is a need for clinicians, scientists, the industry, and patient organisations to work collectively. Efforts to achieve this goal are well advanced.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





