


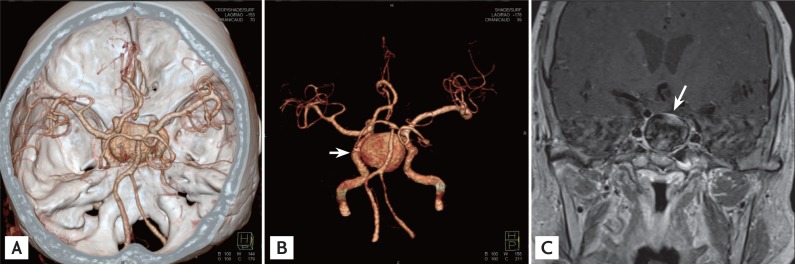
A 73-year-old woman presented at our institution with a 1-day history of drowsy mental status and a 2-month history of headache and general weakness. She had not taken any medications. Laboratory investigations showed severe hyponatremia (Na, 114 mEq/L) and a potassium level of 3.2 mEq/L. A computed tomography (CT) angiogram showed an intrasellar 3.0-cm aneurysm arising from the left internal carotid artery (Fig. 1A and 1B). Basal pituitary hormone profiles showed morning cortisol, 1.43 µg/dL; adrenocorticotrophic hormone, 21.86 pg/mL; thyroid stimulating hormone, 1.36 mIU/L; free thyroxine, 0.6 ng/dL; follicle stimulating hormone, 2.46 IU/L; luteinizing hormone, 0.23 IU/L; and prolactin, 45.72 ng/mL, suggesting panhypopituitarism. A T1-weighted magnetic resonance image (MRI) revealed an aneurysm compressing the pituitary gland that was enhanced heterogeneously after injecting gadolinium (Fig. 1C).
Treatment with intravenous saline for volume expansion and 100 mg intravenous hydrocortisone were started. Her symptoms improved immediately, and the hyponatremia normalized. The patient did not want further endovascular intervention for the aneurysm. The patient has been on a daily replacement dosage of 5 mg prednisolone and 75 µg thyroid hormone.
Sella aneurysms are an uncommon subtype of intracranial aneurysm and rarely cause hypopituitarism. The most common presenting symptoms of a patient with a giant intrasellar aneurysm are headache and visual field cuts or decreased visual acuity. Mental changes can occur, albeit rarely, when the aneurysm ruptures. Clinically significant hyponatremia has been reported at presentation in 21% of patients with unruptured intrasella aneurysms. The decreased mental status of the presenting case was associated with the hyponatremia induced by secondary adrenal insufficiency. Differentiating between pituitary adenoma and intrasella aneurysm is crucial to avoid a potential surgical catastrophe. CT angiography and MRI are useful tools for the differential diagnosis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





