


INTRODUCTION
B-cell precursor acute lymphoblastic leukemia (BCP-ALL) accounts for approximately 70ŌĆō75% of all adult ALL cases [1,2]. BCP-ALL is characterized by immunophenotyping of blasts, for which CD20 expression has become clinically important owing to its prognostic significance and the development of targeted agents [3,4]. CD20, a B-lineage-specific antigen, is expressed in normal and malignant cells. Generally, 80ŌĆō90% of mature B cells express CD20, whereas 30ŌĆō50% of B cells in patients with BCP-ALL express CD20 [5,6]. CD20 plays a pivotal role in cell cycle regulation via its function as a calcium channel, and its expression may be associated with drug resistance [7,8]. Although the prognostic implications of CD20 expression in pediatric ALL are controversial, the influence of CD20 expression in adult patients with BCP-ALL treated with vincristine, doxorubicin, and dexamethasone (VAD) or hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD) chemotherapy demonstrated a CD20 positivity rate of at least 20% was associated with poor prognosis [6,9ŌĆō12].
Rituximab is a chimeric monoclonal antibody that targets CD20 expressed on the surface of malignant B-cells. Its incorporation into first-line chemotherapy significantly improves outcomes for various B-cell lineage hematologic malignancies, such as diffuse large B-cell lymphoma and chronic lymphocytic leukemia [13ŌĆō16]. Chemoimmunotherapy with a hyper-CVAD and rituximab regimen also improved survival in adult patients with CD20-positive Philadelphia (Ph) chromosome-negative BCP-ALL [17,18]. In a randomized trial of 209 patients with Ph-negative ALL, patients who received rituximab-containing chemotherapy had longer event-free survival (EFS) than those treated with conventional chemotherapy, with estimated 2-year EFS rates of 65% and 52%, respectively [18]. Thus, adding rituximab to intensive combination chemotherapy has become the standard regimen for patients with Ph-negative BCP-ALL. Conversely, rituximab is not widely recommended as a front-line regimen for patients with Ph-positive ALL, as tyrosine kinase inhibitors (TKIs) are typically used. Thus, clinical studies evaluating rituximab plus multiagent chemotherapy with TKIs in patients with Ph-positive ALL are lacking.
In this multicenter, prospective clinical trial, we evaluated the survival benefit of rituximab-containing multiagent chemotherapy in patients with newly diagnosed CD20-expressing Ph-positive adult BCP-ALL. In addition, the effect of adding rituximab on prognosis in patients with Ph-negative ALL was also evaluated.
METHODS
Patient eligibility
Patients with newly diagnosed ALL, aged Ōēź 15 years, were eligible for this study if their leukemic blast cells in bone marrow (BM) expressed CD20 antigen Ōēź 20% at the time of diagnosis. Other inclusion criteria were: Eastern Cooperative Oncology Group performance status Ōēż 2 or Karnofsky scale > 60%, adequate cardiac function (ejection fraction > 45%) evaluated by echocardiography, adequate kidney function (serum creatinine < 1.5 mg/dL), and adequate liver function (serum bilirubin < 1.5 mg/dL and serum transaminase < 3 times the upper normal limit). Patients were excluded if they had an ongoing infection or were being treated for underlying disease with other investigational agents. Cytogenetic abnormalities were evaluated using conventional cytogenetics and fluorescent in-situ hybridization. The high-risk groups were defined as follows: age > 35 years, high white blood cell count (> 30.0 ├Ś 109/L), central nervous system (CNS) involvement with poor cytogenetic abnormalities such as hypodiploidy (Ōēż 44 chromosomes), t(9;22)(q34;q11.2):BCR-ABL1, t(v;11q23), and t(11;19):KMT2A translocations, and complex karyotypes (five or more chromosomal abnormalities) [19,20]. This study was approved by the Institutional Review Board of Asan Medical Center (2011-0635), Kyungpook National University Hospital (2011-12-018) and each other participating center. Written informed consent was obtained from all patients.
Study design
This trial was a prospective, non-randomized, multicenter phase II study conducted from November 2011 to July 2015 at 12 Korean centers. All enrolled patients received multiagent chemotherapy comprising vincristine/prednisolone/daunorubicin and L-asparaginase (Ph-negative patients) or imatinib (Ph-positive patients) with rituximab, the details of which are summarized in Table 1. Eight infusions of rituximab were administered throughout the treatment cycle according to previous reports [14,17]; on day 8 of induction and consolidation A and B, and on days 8 and 22 of consolidation C (Table 1). After achieving complete remission (CR), patients who could not undergo allogeneic hematopoietic cell transplantation (allo-HCT) received five cycles of consolidation chemotherapy with concomitant rituximab, followed by 2 years of maintenance therapy. Ph-positive transplant-eligible patients stopped taking imatinib prior to the allo-HCT, whereas transplant-ineligible patients took imatinib as maintenance therapy after consolidation for 2 years. Allo-HCT was performed when the patient had a suitable donor. Donor selection, conditioning regimen, and graft-versus-host disease (GVHD) prophylaxis were determined by the investigator. For patients who underwent allo-HCT during consolidation, rituximab was administered monthly beginning on day 90 post-transplantation. All patients received eight rituximab doses during the entire treatment period, regardless of allo-HCT status. CNS prophylaxis was performed using 15 mg of intrathecal methotrexate with 50 mg of hydrocortisone during induction and consolidations up to six cycles considering the condition(s) of the patients. This clinical trial is registered at www.clinicaltrials.gov as NCT01429610.
Evaluation of CD20 expression
Immunophenotypic analysis was performed using whole BM aspirate samples at the time of diagnosis. Lymphoblast surface antigens (CD19, CD20, and CD22) were detected using three- or four-color flow cytometry, and CD20 positivity was defined as a baseline CD20 expression rate of Ōēź 20% blasts as reported previously [6,17]. The clinically significant cut-off value of CD20 expression remains unclear; thus, we used the receiver operating characteristic (ROC) curve and area under the curve (AUC) to set the cut-off value for survival analyses.
Assessment of response and safety
To determine the response to induction chemotherapy, a BM study was conducted on approximately the 28th day after induction initiation if the patient achieved an absolute neutrophil count (ANC) Ōēź 1,000/╬╝L and platelet (PLT) count Ōēź 100,000/╬╝L. CR was achieved when there were < 5% blasts in the BM, Ōēź 20% cellularity in the BM biopsy with normal maturation of all cell types, the disappearance of BM chromosomal abnormality, absence of leukemia blasts in the peripheral blood, ANC Ōēź 1,500/╬╝L, PLT count Ōēź 100,000/╬╝L, and no evidence of extramedullary involvement of the CNS or soft tissue. Relapse was defined as disease recurrence after achieving CR with Ōēź 5% blasts in the BM, blasts in the peripheral blood, or evidence of new extramedullary involvement. Patients who failed to achieve CR after induction therapy and were alive for over 1 week were considered resistant.
Safety assessments were conducted at each patient visit. Toxicity was graded according to the Common Terminology Criteria for Adverse Events version 4.0 (NIH, Bethesda, MD, USA).
Statistical analyses
The sample size was determined based on relapse-free survival (RFS). RFS was determined from the date of CR to the date of relapse or death from any cause, whichever occurred earlier. Overall survival (OS) was determined from the date of study enrollment to the date of death or last follow-up. To determine the time dependence of allo-HCT according to CD20 expression, the Simon and Makuch method was used for graphical representation, and the Mantel-Byar test was used for univariate analysis. The Cox regression model was used for multivariate analyses. Factors with a p Ōēż 0.1 in the univariate analysis were included in the multivariate analysis. Hazard ratios (HRs) and 95% confidence intervals were estimated for each factor. Statistical significance was set at p < 0.05. All statistical analyses were performed using R statistical software (version 3.6.2; R Foundation for Statistical Computing, Vienna, Austria, available at http://www.r-project.org).
RESULTS
Patients
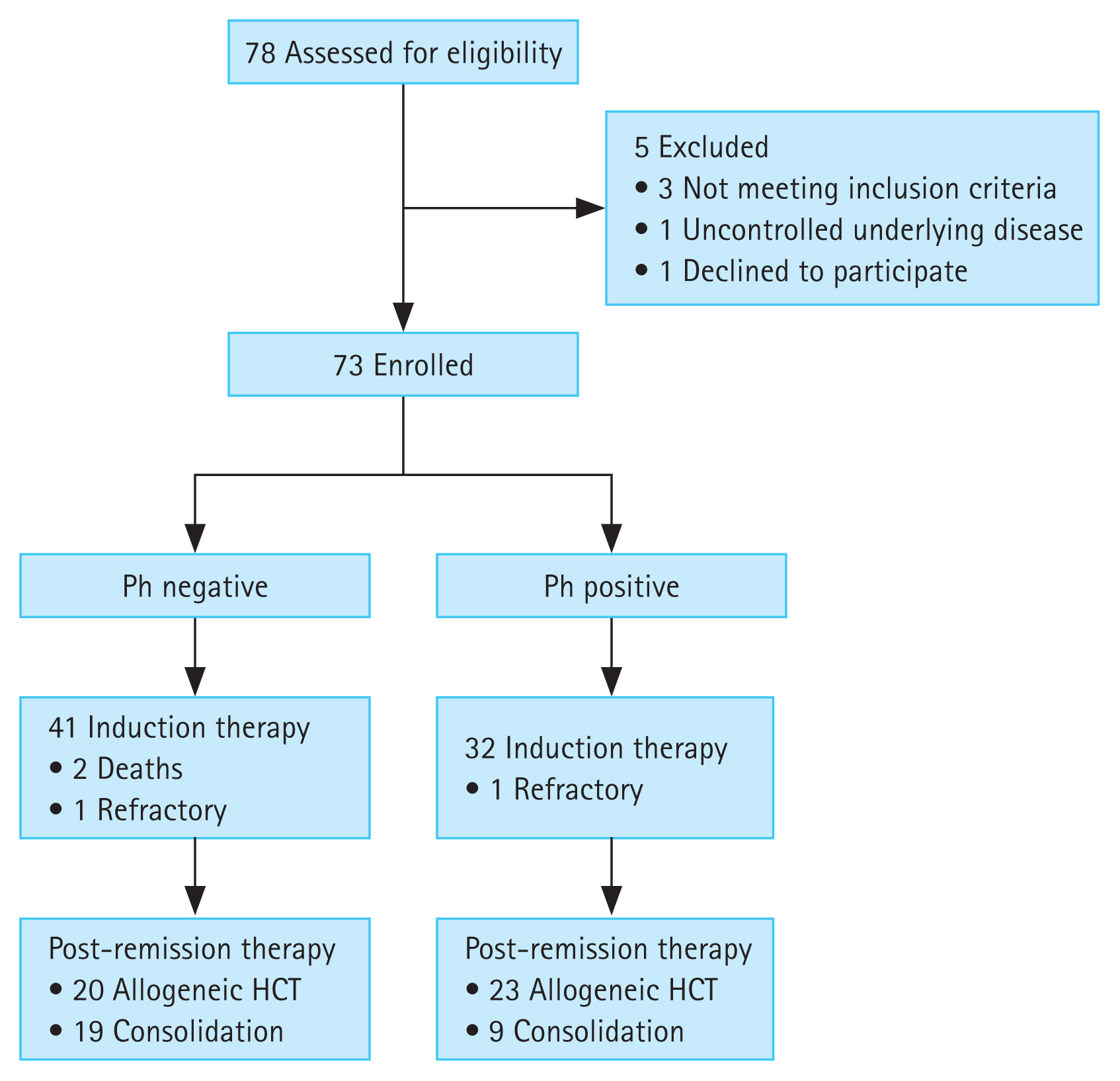
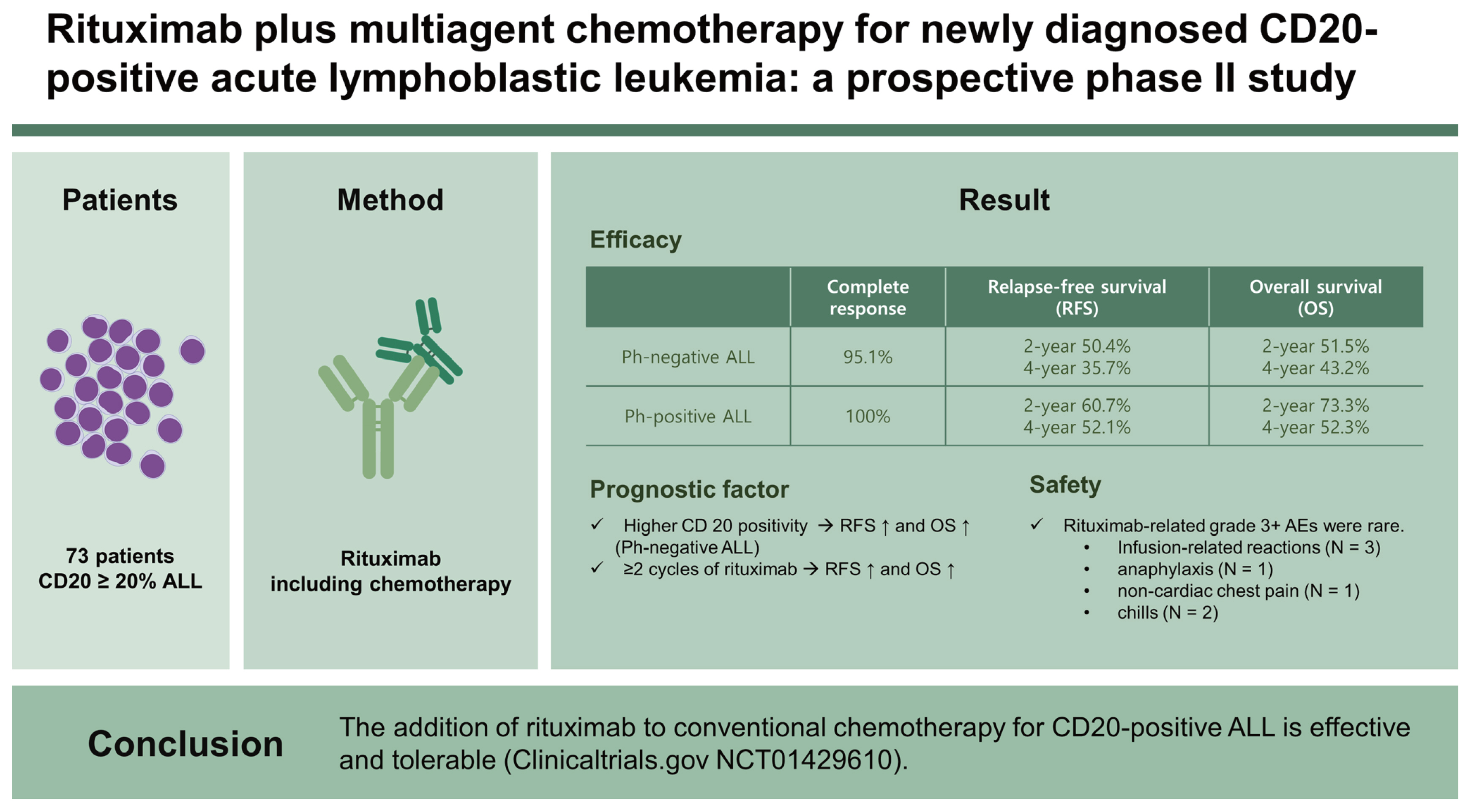
Seventy-eight patients with newly diagnosed ALL were enrolled from 12 centers. Five patients were excluded (three did not meet the inclusion criteria, one met the exclusion criteria, and one withdrew informed consent); therefore, 73 patients were finally included in the trial. Forty-one patients (56.2%) were Ph-negative, and 32 (48.3%) were Ph-positive. The median age of patients with Ph-negative ALL was 37 years, whereas that of patients with Ph-positive ALL was 53 years (p = 0.013). All patients with Ph-positive ALL were classified into the high-risk group because of the presence of the t(9:22) or BCR-ABL1 fusion gene, whereas 27 patients (65.9%) with Ph-negative ALL were found to be at high risk. The median proportion of blasts expressing CD20 was 51.8% (range, 20.2ŌĆō95.1%) in patients with Ph-negative ALL and 42.4% (range, 20.6ŌĆō99.4%) in patients with Ph-positive ALL. The baseline patient characteristics are summarized in Table 2.
Response to therapy and progress
After induction chemotherapy, 69 of 73 patients (94.5%) achieved CR, and two died of BM aplasia during induction therapy. The other two patients achieved CR after the first consolidation, yielding an overall CR rate of 97.3% (71 of 73). Of the 73 patients, 43 (58.9%) underwent allo-HCT; prior to allo-HCT, 42 patients had achieved CR, and one had relapsed. A median of eight rituximab doses were administered to the patients who received consolidation chemotherapy alone, whereas a median of six rituximab doses were administered to the patients who underwent allo-HCT. After achieving CR, 29 patients (39.7%) experienced relapse (BM relapse in 28 patients and CNS relapse in one patient).
Thirty-nine of 41 patients (95.1%) with Ph-negative ALL achieved CR, and 20 patients (51.3%) experienced relapse during post-remission therapy. Among the 41 patients, 20 (48.8%) received allo-HCT, of whom eight had disease relapse. All 32 patients in the Ph-positive ALL group achieved CR. Nine patients experienced relapse, and the cumulative relapse rate was 28.1%. Twenty-three patients (71.9%) underwent allo-HCT, four of whom (17.4%) experienced relapse after transplantation. Figure 1 displays the flow diagram of the enrolled patients.
Survival outcomes
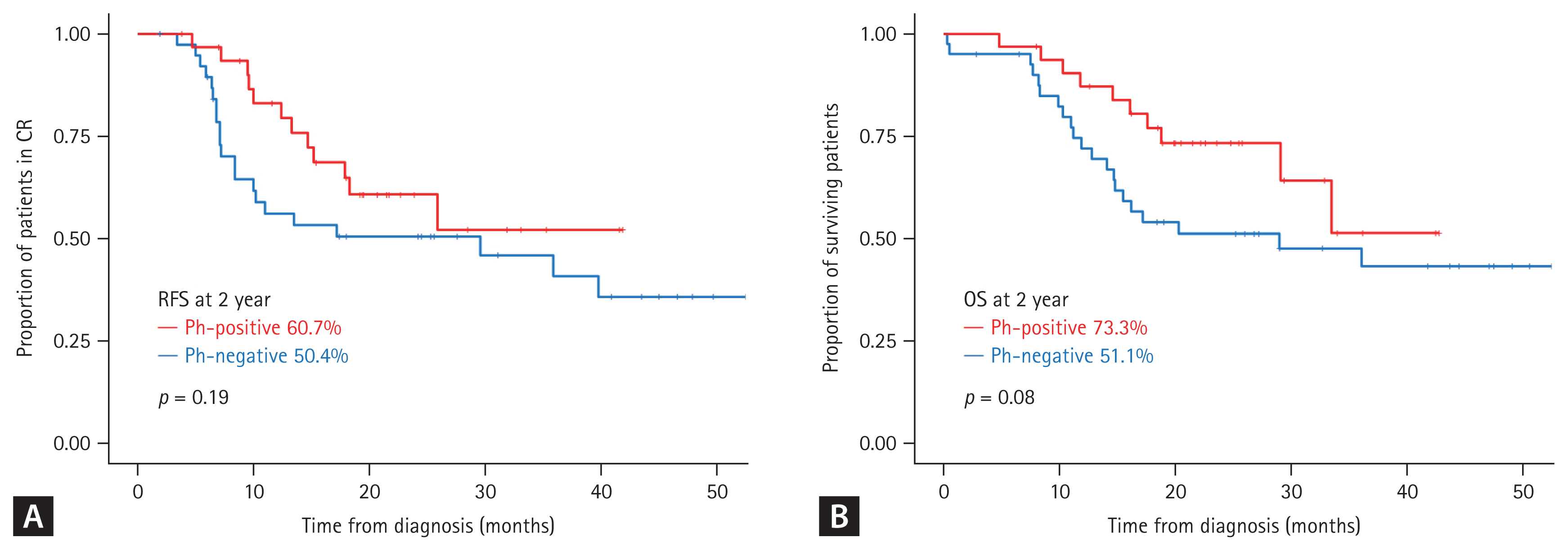
The median follow-up duration of all patients was 25.9 months (range, 2.8ŌĆō55.0). The 1-, 2-, and 4-year RFS rates were 68.4%, 55.3%, and 40.2%, respectively, whereas the 1-, 2-, and 4-year OS rates were 78.7%, 60.8%, and 48.0%, respectively (Supplementary Fig. 1). In patients with Ph-negative ALL, 21 (51.2%) died, with 10 dying after transplantation owing to disease progression (n = 8), acute GVHD (n = 1), and infection (n = 1). Ten patients (31.3%) with Ph-positive ALL died, of which eight died after allo-HCT owing to disease progression (n = 3), infection (n = 3), brain hemorrhage (n = 1), and acute pancreatitis (n = 1). The 2- and 4-year RFS rates in patients with Ph-negative ALL were 50.4% and 35.7%, respectively, whereas the 2- and 4-year OS rates were 51.5% and 43.2%, respectively. The 2- and 4-year RFS rates in patients with Ph-positive ALL were 60.7% and 52.1%, respectively, whereas the 2- and 4-year OS rates were 73.3% and 52.3%, respectively. Overall, patients with Ph-negative ALL had a higher incidence of disease relapse. In contrast, patients with Ph-positive ALL showed better RFS and OS (Fig. 2). The cumulative 2-year incidence of non-relapse mortality (NRM) was comparable between groups at 20.2% and 23.4% in Ph-negative and -positive ALL patients, respectively (Supplementary Fig. 2).
Comparison of outcomes based on CD20 expression
There was no significant difference in CD20 expression between patients with Ph-negative or -positive ALL. Overall, the median CD20 expression rate was 47.5%. We analyzed CD20 positivity and relapse using the ROC curve and AUC to identify a clinically significant cut-off value for survival (Supplementary Fig. 3). Our data suggests that 46.3% CD20 positivity was the most reliable cutoff value. Patients with higher (Ōēź 46.3%) CD20 positivity experienced significantly longer RFS (p = 0.006) than those with lower CD20 positivity (< 46.3%). Moreover, the CD20 positivity rate at diagnosis had a more significant effect on the long-term clinical course of patients with Ph-negative ALL than those with Ph-positive ALL. In the Ph-negative ALL group, patients with high CD20 positivity experienced more favorable RFS (p < 0.001) and OS (p = 0.06) compared to those with low CD20 positivity; conversely, CD20 positivity was not associated with differences in the long-term outcomes (RFS and OS) of patients with Ph-positive ALL (Fig. 3).
Comparison of outcomes based on allo-HCT status
A total of 43 patients (58.9%) proceeded to receive frontline allo-HCT at a median of 4.3 months (range, 1.7ŌĆō11.9) after achieving CR and after a median of 3 cycles (ranges, 2ŌĆō5) of consolidation. The details of allo-HCT are summarized in Supplementary Table 1. Overall, patients who underwent allo-HCT experienced a lower frequency of recurrence. In contrast, patients who did not undergo transplantation experienced continuous disease relapse over time (Supplementary Fig. 4). However, there was no significant difference in the long-term survival of patients receiving allo-HCT or not, regardless of CD20 expression (Supplementary Fig. 5). In our long-term survival analysis, patients with Ph-positive ALL experienced better RFS (p = 0.059) following allo-HCT than those with Ph-negative ALL; however, transplantation had no effect on OS.
Patients who underwent allo-HCT received rituximab a median of six times (range, 2ŌĆō8); however, 17 patients (10 Ph-negative and seven Ph-positive patients) did not receive rituximab after transplantation owing to patient refusal (n = 7), relapse (n = 3), the discretion of the clinician (n = 3), having completed the rituximab schedule before allo-HCT (n = 2), an adverse event (AE) (n = 1), or death (n = 1). Additionally, five patients received only one additional dose of rituximab based on the discretion of the clinician (n = 3), relapse (n = 1), or an AE (n = 1). Three patients received two cycles of rituximab, and 18 patients received three cycles of rituximab after transplantation. In patients who underwent allo-HCT, the total number of cycles of rituximab received throughout the treatment period did not affect long-term survival; however, patients who received rituximab for at least one cycle after allo-HCT experienced better RFS (HR, 0.37; p = 0.079) and OS (HR, 0.38; p = 0.045) than patients who did not receive rituximab after transplantation. Furthermore, patients who received Ōēź 2 cycles of rituximab after transplantation had significantly improved RFS (HR, 0.31; p = 0.049) and OS (HR, 0.29; p = 0.021) compared to those who received < 2 cycles (Supplementary Fig. 6).
Toxicities of combination chemotherapy with rituximab and imatinib
All grade 3 or 4 severe AEs reported during induction and/or consolidation chemotherapy are summarized in Table 3. Seventy-two of 73 patients (98.6%, one died before the rituximab schedule) were successfully administered rituximab infusions during induction therapy. All patients received rituximab according to the planned schedules during consolidation or after allo-HCT unless disease relapse or death occurred. Rituximab-related grade 3+ AEs were rare. Infusion-related reactions (n = 3), anaphylaxis (n = 1), non-cardiac chest pain (n = 1), and chills (n = 2) were reported as rituximab-related severe AEs. During induction, four patients discontinued imatinib for 2ŌĆō14 days owing to infection (n = 2) or nausea/vomiting (n = 2); however, no dose reduction occurred. Transient interruptions of imatinib were reported, and the imatinib dose in four patients was reduced to 400 mg/day owing to severe nausea/vomiting during consolidation. The hematologic/non-hematological toxicity profiles were tolerable. Cytopenia is a common hematologic AE. Most patients were administered granulocyte-colony stimulating factor and received transfusions during chemotherapy. Febrile neutropenia and serum aspartate transaminase/alanine aminotransferase elevation were the most reported severe AEs. Other causative AEs during induction and/or consolidation included skin rashes, nausea/vomiting, oral mucositis, and peripheral neuropathy. There were no statistically significant differences in the toxicity profiles of Ph-negative and -positive patients with ALL.
Prognostic factors affecting long-term survival
Cox regression analyses were performed to identify significant factors that influenced RFS and OS. The results of univariate and multivariate analyses are shown in Table 4. In the multivariate analysis, high positivity of CD20 (HR, 0.21; p = 0.001), Ōēź 4 cycles of rituximab (HR, 0.29; p = 0.012), and allo-HCT (HR, 0.44; p = 0.035) were favorable factors for RFS, whereas extramedullary involvement at diagnosis (HR, 3.44; p = 0.018) and the number of rituximab cycles (HR, 0.18; p < 0.001) were independent predictors for OS.
DISCUSSION
This study was conducted to determine the prognostic relevance of CD20 expression and the effect of rituximab in de novo adult BCP-ALL. The results suggest that the addition of rituximab to conventional chemotherapy regimens for CD20-positive BCP-ALL is effective and tolerable in both Ph-negative and -positive ALL patients.
In a clinical trial that used the same multiagent regimen as our study, Kim et al. [21] reported a 72% 2-year OS rate in 82 Ph-positive patients treated with nilotinib plus chemotherapy, which is at par with our findings for rituximab. In their study, the median age of the enrolled patients was 47 years, and 69.5% of patients underwent allo-HCT [20]. The median age of Ph-positive patients in our trial was higher than that of previous studies (53 years), with 71.9% of patients undergoing allo-HCT [21,22]. Importantly, toxicities related to imatinib and rituximab did not affect the treatment, and the NRMs were not a cause for concern.
Compared with the historical treatment group who received the same chemotherapy regimen without rituximab, patients who received rituximab-containing therapy exhibited better RFS and OS (Supplementary Fig. 7, Supplementary Table 2). Although improved survival outcomes were identified through a comparative study with a historical treatment group, long-term survivals in this study remained lower than expected (Table 5). Recently, outcomes of a phase 3 multicenter randomized controlled trial were reported. Adult patients with BCP-ALL received four doses of rituximab plus standard chemotherapy; 3-year EFS was 51.4%, and 3-year OS was 57.3% [23]. These results were not significantly different from our findings. Therefore, death during chemotherapy or stem cell transplantation (NRM) and its effect on the overall study outcomes should be considered.
Careful survival analysis is required in patients with Ph-negative ALL treated with rituximab and immunochemotherapy. In retrospective long-term data of de novo BCP-ALL, patients with > 20% CD20 positivity experienced worse outcomes; however, survival improved when rituximab was combined with chemotherapy [6,24,25]. To date, only a few studies have evaluated the relationship between survival outcomes and the proportion of CD20-positive blasts. In our study, patients with a > 46.3% CD20 positivity rate experienced better RFS and EFS than those with lower CD20 positivity. This finding is consistent with that reported by Maury et al. [18], who conducted a clinical trial with 209 de novo Ph-negative and CD20-positive ALL patients treated with rituximab plus the GRAALL-2005 regimen. In their trial, the median percentage of CD20-positive blasts was 66%, and patients with a > 66% CD20 positivity rate experienced favorable outcomes following rituximab treatment [18]. Furthermore, minimal residual disease (MRD) responders reportedly exhibited higher CD20 expression during rituximab-containing regimens than MRD persisters [26]. Thus, the use of rituximab only in patients with CD20 positivity above the arbitrary threshold of 20% remains controversial. Changes in CD20 positivity rates have been observed during early treatment [26], and pretreatment with corticosteroids reportedly upregulates CD20 expression in leukemia cells [27,28]. Therefore, studies evaluating combinatorial immunochemotherapy with rituximab in patients with BCP-ALL with CD20 levels < 20% are warranted.
Even in the era of intensive chemotherapy with targeted agents, disease relapse remains a major cause of treatment failure in adult ALL patients, and allo-HCT after CR remains the go-to treatment [29,30]. Previous studies have reported an approximately 30ŌĆō50% chance of relapse within 2 years following allo-HCT [31,32]; thus, post-transplant strategies are needed to maintain long-term CR. In the present study, 43 of 73 patients (58.9%) underwent frontline allo-HCT, and those who received at least one cycle of rituximab after transplantation showed improved long-term survival. Notably, the statistical significance was further strengthened when comparing patients who received Ōēź 2 cycles of rituximab after transplantation with those who received < 2 cycles. However, our data with regard to the use of post-transplant rituximab should be cautiously interpreted. Our results are not based on MRD, and patients who were unsuitable for further treatment after transplantation were likely not receiving rituximab. Rituximab is also used to treat GVHD, but the consensus on whether it affects the graft-versus-leukemia effect after allogeneic transplantation remains unclear.
The findings of the present study indicated significantly improved outcomes with rituximab; however, the major limitation is that the MRD test was not performed for the issues of the standardization for each hospital during the study period. Overcoming this limitation may provide clearer insights into choosing patients who would benefit the most from rituximab in combination with multi-agent chemotherapy.
In conclusion, the combination of rituximab with multiagent chemotherapy is a feasible and promising treatment strategy. Although this was not a randomized trial, we observed a positive relationship between CD20 positivity and disease outcome, suggesting that the addition of rituximab to traditional multiagent chemotherapy may improve clinical outcomes, irrespective of Ph chromosome status or transplantation performance. Overall, this trial supports the addition of rituximab to chemotherapy treatment strategies for patients with ALL.
KEY MESSAGE
1. The addition of rituximab to conventional chemotherapy for CD20-positive acute lymphoblastic leukemia (ALL) is effective and tolerable.
2. CD20 positivity rate at diagnosis had a greater effect on the long-term clinical course of patients with ALL.
3. Patients who received Ōēź 2 cycles of rituximab after allogeneic hematopoietic cell transplantation had significantly improved long-term survival.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement figure 1
Supplement figure 1 Print
Print





