


INTRODUCTION
Currently healthcare-associated infections (HAIs) are associated with increasing medical costs and significant disability to the patients [1,2]. Moreover, those are the causes of prolonged hospitalization periods, and increased mortality and morbidity [3–5]. In intensive care units (ICUs) in particular, aside from disease severity, there are various risk factors for HAIs such as the use of invasive procedures and instruments, use of broad-spectrum antibiotics, and a high level of colonization by pathogenic organisms. In HAIs, the proportion of multidrug-resistant organisms as primary pathogens is increasing annually [6].
Infection-control measures including hand hygiene, active surveillance cultures, and environmental cleaning are generally recommended to reduce the HAIs [7]. It is recognized that hospital instruments are closely associated with the spread of infection as inappropriately sterilized instruments and environmental surface contamination leads to the emergence of infectious disease [8]. Contaminated environmental surfaces by microorganisms do not directly cause infection of patients and medical personnel, but offer a potential chance of spread of infection through surface contact [9]. Hence, the method of cleaning and disinfection must be adequate to counter this threat. Microorganisms will still remain on environmental surfaces because disinfectant efficacy declines as time passes. The methicillin resistant Staphylococcus aureus (MRSA) pathogen, which is a major cause of HAIs, can survive in a non-biosphere such as on the glass or steel from 4 weeks to 7 months, vancomycin resistant Enterococcus faecium (VRE) from 5 days to 4 months, Acinetobacter spp. from 3 days to 5 months, Pseudomonas spp. from 6 hours to 16 months, and Candida spp. from 1 to 150 days [10].
Copper and copper alloys are recognized to have bactericidal and bacteriostatic properties. Previous studies have attempted to verify the antimicrobial activity of copper in different environments [11–13]. It has been shown that copper surfaces have antimicrobial properties and therefore have reduced a numbers of microorganism colonies. This decreases the chances of contamination of medical personnel via fixtures and fittings or medical instruments. The activity of copper in this regard has not been tested in a clinical study. In the present study we assessed the antimicrobial properties of copper and copper alloy against MRSA and VRE and demonstrated the reduction of microbial environmental colonization in an ICU setting of a Korean hospital.
METHODS
The study was approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (2011-0466) and was conducted in the laboratory and medical ICU at Asan Medical Center with 18 medical ICU beds for 3 months. MRSA and VRE were supplied by Korean cell culture center (Seoul, Korea), and were incubated in tryptone soy broth at 37°C with aeration. Copper, copper alloy, and stainless steel experimental plates (5 × 5 cm, provided by the International Copper Association, Seoul, Korea) were sterilized in an autoclave. After incubation, the plates were inoculated with 40 μL of MRSA or VRE containing approximately 6 × 104 colony-forming units (CFU)/mL at room temperature (24°C), and 10.7% humidity. Using the stamp method, sampling was done at 10 time points (15, 30, 45, 60, 75, 90, 180 minutes, 6, 12, and 24 hours). The plates were incubated at 37°C for 48 hours and CFUs were counted. All experiments were performed in triplicate.
In vivo analysis
Two similar rooms were chosen among the 18 medical ICUs at Asan Medical Center. One room had copper-containing surface items that were touched often by medical personnel. The other room contained stainless steel surface items that included an infusion pole, a bedside rail, a door knob, a drawer and a drug cart. The items of two rooms were the same but the surfaces were covered with different materials, and were sampled once weekly at 9:30 AM after routine cleanings and again at 11:30 AM after visiting hours, during that time patients had received healthcare workers or visitors. A sterile swab moistened in 0.9% sterile saline was applied five times horizontally and vertically over a 5 × 5 cm area. Samplings were transferred to the laboratory and each CFU was counted. The same disinfectant and protocol was used for both the copper and non-copper-containing surface items. Temperature and humidity were also similar for each tested surface.
Statistical methods
The median total CFU count was compared that were remained at according to time interval. Using the chi-square test, we evaluated the antimicrobial activity on the tested metal surfaces assuming that a decreased colony count means higher antimicrobial activity. The statistical analysis were performed with IBM SPSS Statistics version 20.0 (IBM Co., Armonk, NY, USA). A p value of < 0.05 was considered statistically significant
RESULTS
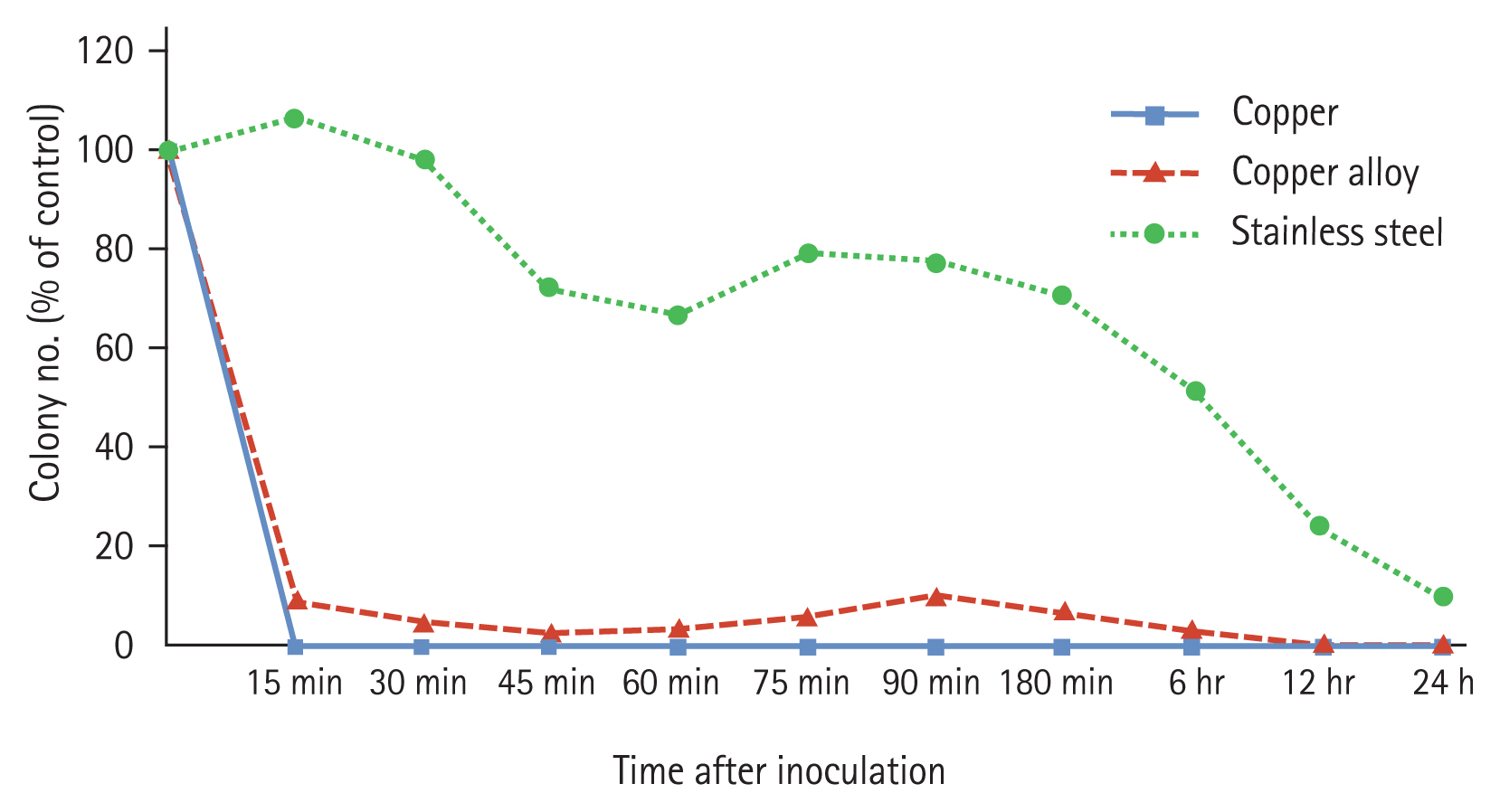
In vitro time-kill curves were obtained in triplicate and indicated that exposure to copper significantly reduced, and in some cases completely killed MRSA colonies after 15 minutees, which was maintained for 24 hours. On copper alloy plates, MRSA colonies were decreased by nearly 90% after 15 minutes and completely killed at 12 hours, and this was maintained for 24 hours. In comparison, MRSA colonies only slowly decreased on stainless steel plates and 5% of the colonies remained after 24 hours (Fig. 1).
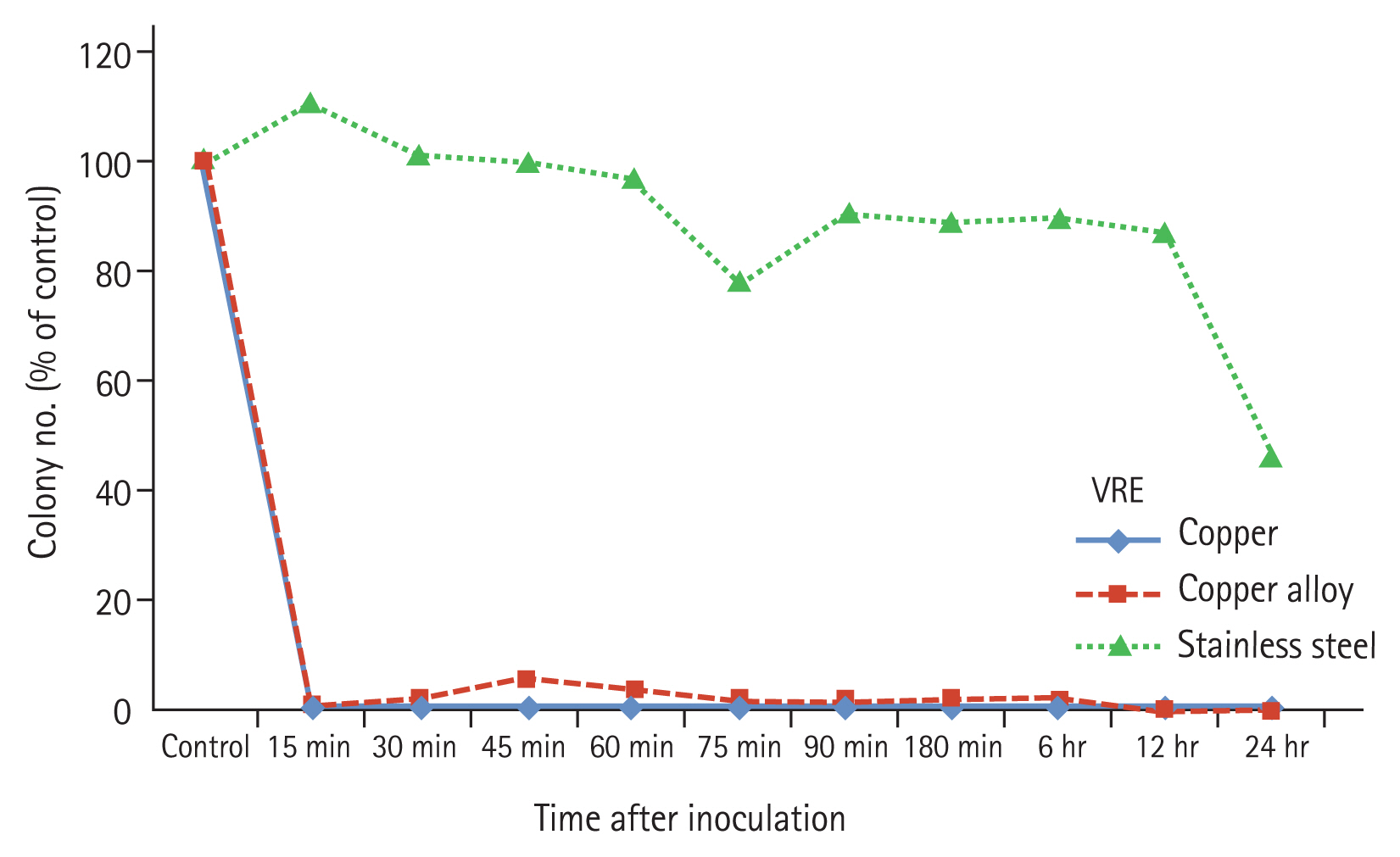
On copper plates, the time-kill curves for VRE were similar to those for MRSA. VRE colonies were found to be significantly reduced and fully eradicated at 15 minutes, which was maintained for 24 hours. On copper alloy plates, 3% of the VRE colonies remained at 15 minutes, VRE colonies were completely destroyed after 12 hours, and this was maintained for 24 hours. In comparison, on stainless steel plates, VRE colonies were only slightly decreased as time progressed and 45% of the colonies persisted (Fig. 2).
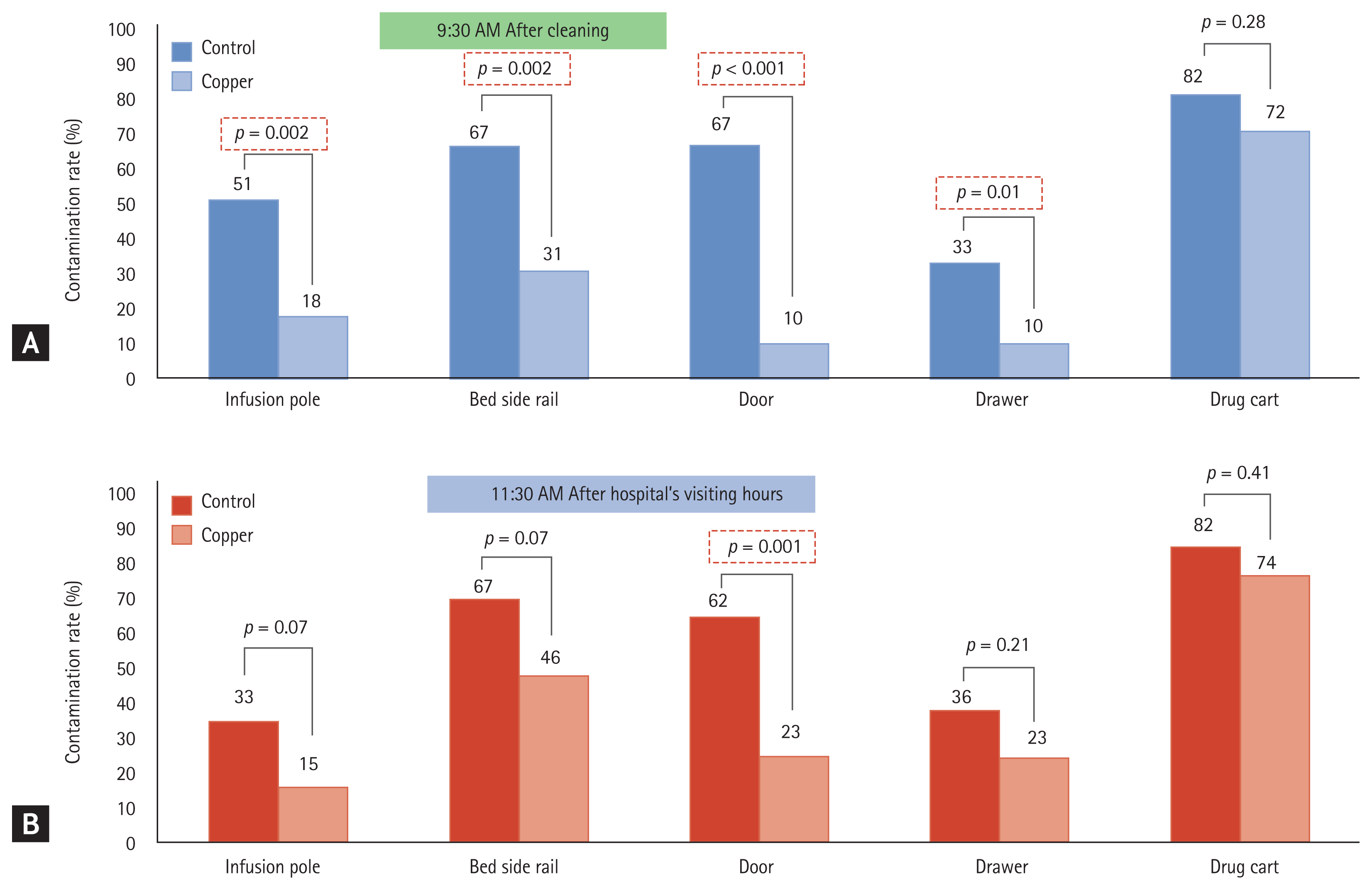
The median CFU count per plate from our in vivo analysis of MRSA, comparing copper-containing surfaces with non-copper-containing surfaces is summarized in Table 1. Compared with the controls, MRSA colonies were reduced after cleaning and after patients were seen by their visitors in the copper-containing room. At 9:30 AM, after cleaning, the measured bacterial contamination rate low with statistical significance at the infusion pole, bedside rail, door, and drawer (Fig. 3A). At 11:30 AM, after patients were seen by their visitors, the contamination rate was low only at the door (Fig. 3B). Fig. 3 shows our quantitative analysis of MRSA on copper-containing items compared with the controls.
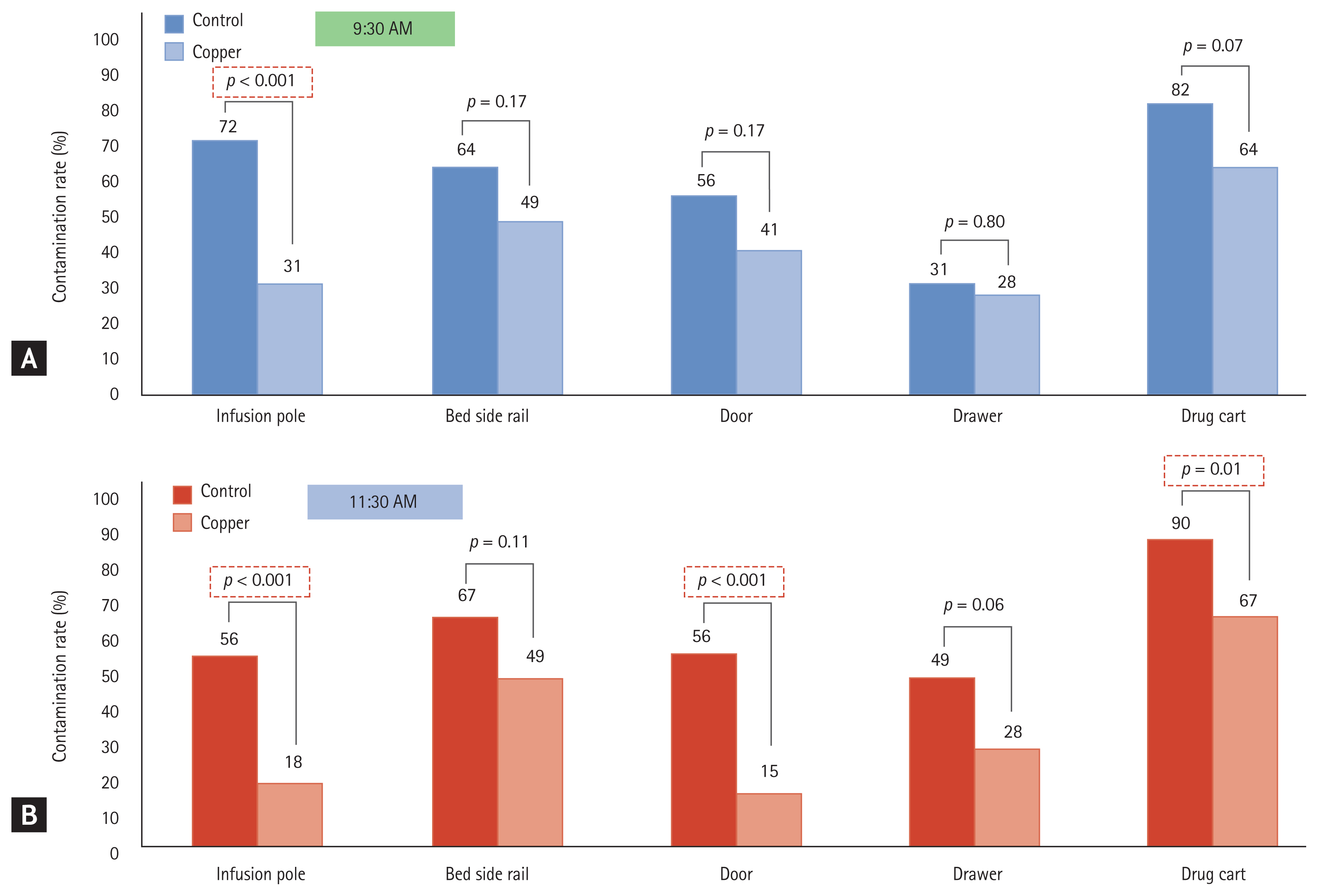
Similar to MRSA, the contamination rate of VRE was low on copper-containing items compared with the controls. VRE was low when measured at the infusion pole after cleaning of the room (Fig. 4) and at the door after patients were seen by their visitors. This was found to be statistically significant and is shown in Table 2.
Hospital equipments (such as infusion pole, a bedside rail, a door knob, a drawer, and a drug cart) in the ICU were used in the experiments (Supplementary Fig. 1).
DISCUSSION
In this study, we investigated contact killing effect of copper and copper alloy surface in vitro and we demonstrated the reduction on microbial colonization on the copper surface in vivo hospital setting, especially in ICU.
There have been many attempts to reduce HAI rates in different ways since the emergence of multi-drug resistant organisms and the increased number of infections by them. It is well known that copper and copper alloy have bactericidal and bacteriostatic effect [11–13].
Still there are several studies of copper alloys on the gram negative bacterial infections. Souli et al. [12] investigated antimicrobial activity of copper surfaces against carbapenemase-producing contemporary Gram-negative clinical isolates: Escherichia coli, Enterobacter spp., Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii producing either VIM-1 and/or KPC-2 or VIM-2 or OXA-type carbapenemases. Eser et al. [14] reported antimicrobial activity of copper alloys against invasive multidrug-resistant nosocomial pathogens. Clinical isolates of MRSA (n = 4), MDR Acinetobacter baumannii (n = 6), and Pseudomonas aeruginosa (n = 4) were evaluated. Cu99 showed a bactericidal effect of less than 1 hour for MRSA, 2 hours for P. aeruginosa and exhibited a closer bactericidal range effect against A. baumannii. Rozanska et al. [15] showed antimicrobial effect of copper alloys on Acinetobacter species isolated from infections and hospital environment. And the results of the study confirmed effective activity (bacteriocidal or bacteriostatic) of copper alloys [15].
Further studies will warrant elucidating the clinical application of our present experimental results that copper alloys reduce MRSA or VRE infection; that is to say, diminishing transmission of infections by copper alloys or decreased number of HAI by those.
To take advantage of copper’s antimicrobial activity, many clinical studies have tried to utilize copper surfaces and instruments in the hospital environment for the purpose of reducing the microbial burden and hospital associated infections [16–19]. We have here demonstrated that copper and copper alloys suppress the growth of multi-drug resistant microorganisms and exhibits a killing effect on these microbes.
In addition we observed that copper can suppress multi-drug resistant bacterias (MRSA and VRE) and eliminate them. The mechanistic action of copper on bacteria has been determined previously as copper ions can bind or cross-link DNA strands and damage DNA [20].
The future studies need to be focus on other types of multi-drug resistant organisms as we are not able to generalize our present experimental results to other strains. The cost-effectiveness of widespread copper use is an issue as it is an expensive metal. Moreover, copper is easy to use but can accumulate rust over time. We thus need to consider how to preserve the properties of copper whilst preventing rust. And copper is able to conduct electricity, that astonishes very transiently the person who touches copper.
This study is to observe the antimicrobial activity of copper in a Korean hospital environment. Although proper hand hygiene remains a more important barrier against HAIs than antimicrobial surfaces [13], potential of copper as another barrier is warranted.
KEY MESSAGE
1. Copper and copper alloys suppress multi-drug resistant bacteria (methicillin resistant Staphylococcus aureus and vancomycin resistant Enterococcus faecium) and eliminate them on the surfaces of material in vitro.
2. The microbial colonization is reduced on the copper surfaces in vivo hospital setting, especially in intensive care unit.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





