



INTRODUCTION
End-stage heart failure (HF) patients are a steeply increasing burden in Korea [1,2]. Heart transplantation (HTx) is the treatment of choice in end-stage HF, however, only a limited number of patients undergo HTx due to strict eligibility criteria and a shortage of donors [1,3ŌĆō5]. According to the latest annual report from the Korean Network for Organ Sharing, the median wait time was 50 months before receiving HTx [6]. For end-stage HF patients who are not eligible for HTx or are not expected to survive the waiting time because of severe cardiac dysfunction, continuous flow left ventricular assist devices (cf-LVADs) have been shown to increase survival for those who undergo LVAD as bridge to transplant (BTT) or destination therapy (DT) [7]. For patients who undergo LVAD as BTT, LVAD treatment has improved the survival time to HTx, facilitated better use of donor organs, and enhanced post-HTx survivals [8,9]. As the device has become more durable and portable, LVAD implantation as DT is increasing and recent trials have shown better functional capacity and quality of life in DT patients when compared to patients with other medical treatment [10,11].
In Korea, after the first few successful cases [12,13], the cases of LVAD implantation are increasing since the approval system for reimbursement under the national health insurance has been introduced for LVAD in October, 2018. Considering the rapidly growing volume of LVAD implantation patients in Korea, we aimed to describe the clinical outcomes of the initial 50 cases from a single center.
METHODS
Study population
This study was a retrospective analysis using data from a single center registry. A total of 50 end-stage HF patients who remained symptomatic despite medical therapy underwent cf-LVAD implantations at Samsung Medical Center from August 2012 to December 2019 (Fig. 1). Informed consent was received from all relevant and the study was approved by the Institutional Review Board of Samsung Medical Center (No. 2017-08-044 and No. 2017-08-167). All patients were followed up until death, HTx, or the censor date, August 2020.
The criteria for LVAD implantation were in accordance with the current LVAD reimbursement indications, which are based on the patient selection criteria from previous LVAD trials (Supplementary Table 1) [14ŌĆō16]. The HeartWare Ventricular Assist Device (HVAD) pump (HW; Heartware, Framingham, MA, USA) was implanted in 17 (34%) patients, while HeartMate II (HMII; Thoratec, Pleasanton, CA, USA) was implanted in 33 (66%) patients. Patients were categorized by the intention for LVAD implantation (BTT/bridge to candidacy [BTC]: n = 30 [60%] vs. DT: n = 20 [40%]). In subanalysis, patients were divided by the period before and after reimbursement initiation by the national insurance, which took place on October, 2018. Detailed information on patient demographics, preoperative risk factors, laboratory parameters, hemodynamic measurements including echocardiography and cardiac catheterization, as well as preoperative risk factors were compared. All patients were maintained on aspirin and warfarin treatment unless contraindicated by serious bleeding.
Multidisciplinary team
All patients underwent comprehensive assessment by a multidisciplinary team to determine indications for LVAD therapy. Our LVAD team maintains a high level of interaction through constant communication and consists of: cardiologists and cardiac surgeons specializing in HF, cardiac intensivist, nurse specialists including device coordinator, staff nurses of the cardiac and cardiothoracic surgical intensive care unit, perfusionist, cardiac rehabilitation team, pharmacist, psychologist, and social service worker. Family dynamics and support as well as medical, socioeconomic condition were carefully evaluated before surgery. After discharge, patients were provided advice and physician contact when needed through a 24/7 hotline by nurse specialists.
Definitions and outcomes
Definitions of associated comorbidities and major adverse outcome are described in Supplementary Table 2 [17ŌĆō26]. All definitions were in accordance with the International Society for Heart and Lung Transplantation (ISHLT) Mechanically Assisted Circulatory Support (IMACS) registry and previous studies [17ŌĆō21,27]. Major adverse events included major bleeding, cardiac arrhythmia, device thrombosis, hemolysis, hepatic dysfunction, major infection, neurologic dysfunction, renal dysfunction, respiratory dysfunction, and right heart failure (RHF) (Supplementary Table 2). Infections were also categorized according to the ISHLT standard definition of infection in LVAD patients [26]. All-cause mortality, major adverse events, and rehospitalizations after LVAD implantation were analyzed.
Statistical analysis
Categorical variables are expressed as percent (frequency) and continuous variables as median (interquartile range [IQR]). Comparisons of continuous and categorical data between groups were performed using unpaired t tests and Fisher exact tests, respectively. The Kaplan-Meier method and log-rank test were used for time-to-event analysis. Statistical significance was considered at a p < 0.05. Statistical analysis was performed using SPSS version 26 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics
Median follow-up was 14 months (IQR, 8 to 23). Clinical characteristics, laboratory, and hemodynamic findings are shown in Table 1. The median patient age was 67 years (IQR, 59 to 73) and 76% were men. The etiology of end-stage HF was ischemic heart disease in 28 (56%) patients, and 16 (32%) patients had prior history of cardiac surgery. Upon LVAD implantation, 86% had New York Heart Association (NYHA) class IV HF symptoms and 60% patients were at the level of Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profile three (60%). When compared according to intention of LVAD implantation, the DT group had a significantly smaller body surface area (p = 0.015) and more advanced age (p < 0.001), which was a critical point for determining treatment strategy. As expected, patients in the DT group were associated with a higher prevalence of comorbidities. Laboratory findings were also worse in the DT group, such as lower albumin, blood urea nitrogen, and higher high-sensitivity C-reactive protein levels. Preoperative status, hemodynamic studies, echocardiographic finding, and preoperative medications were comparable between BTT/BTC and DT groups.
We performed a comparison of baseline characteristics according to sex (Supplementary Table 3) and implantation period (pre- vs. post-reimbursement) (Supplementary Table 4). Women had a significantly smaller body surface area, lower cardiac output, lower sodium, and higher N-terminal-pro hormone B-type natriuretic peptide (NT-proBNP) levels compared to men. Due to a small body surface area, all women underwent HVAD implantation, while 55% of men had implanted HVAD. In our cohort, 23 (46%) patients underwent LVAD implantation at the pre-reimbursement period. Compared to patients after reimbursement, those who received LVAD before reimbursement were significantly older, and had a lower mean pulmonary wedge pressure. More patients evaluated at NYHA class III underwent LVAD implantation in the pre-reimbursement period when compared to the post-reimbursement period.
All-cause mortality and adverse outcomes
There was no in-hospital mortality after LVAD implantation in the initial 50 LVAD patient cohort. The median hospital stay after implantation was 44 days (IQR, 28 to 66). A total of 11 patients died during follow-up. The causes of mortality are described in Table 2. The most common cause was hemorrhagic stroke (n = 3, 27%).
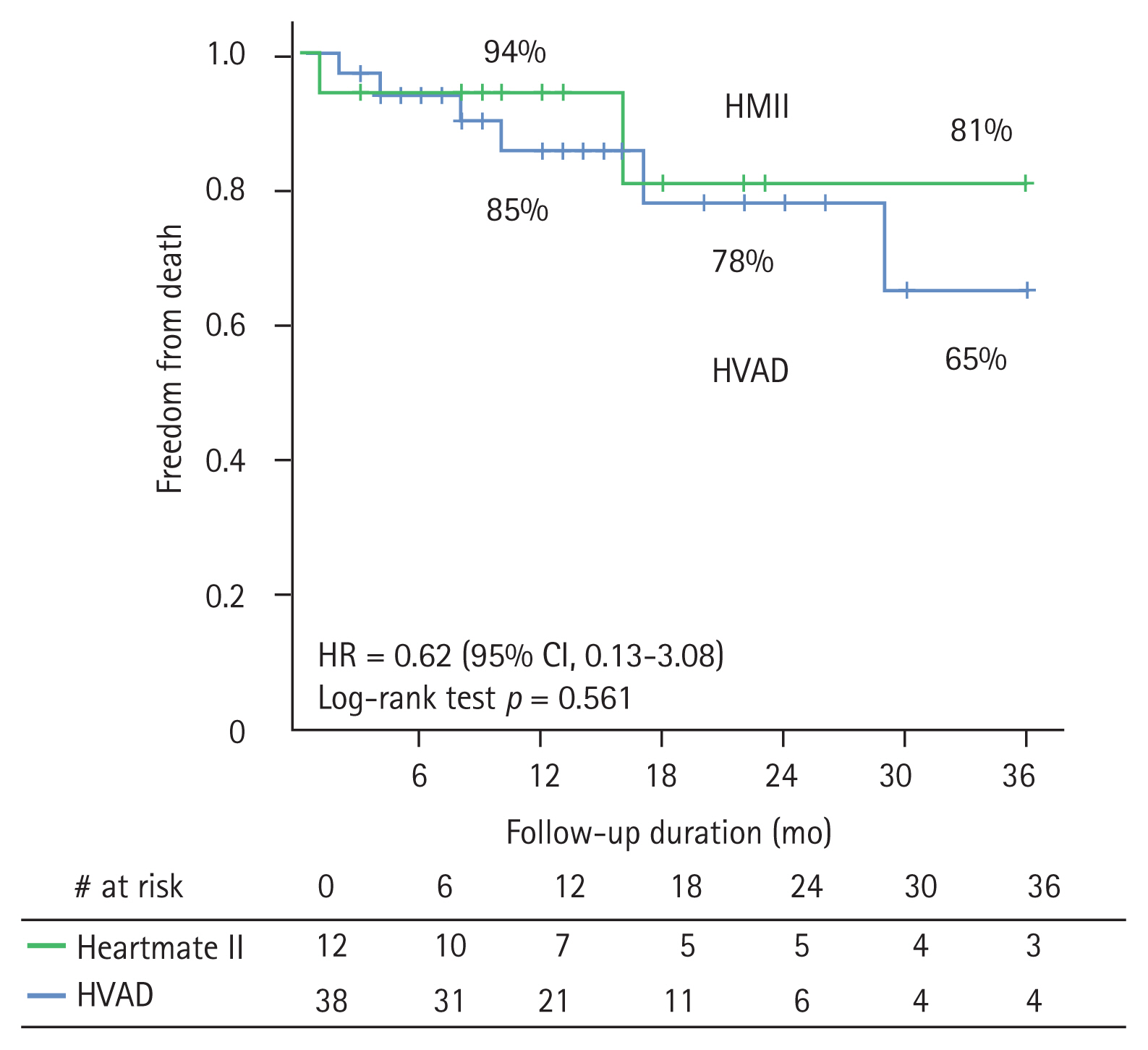
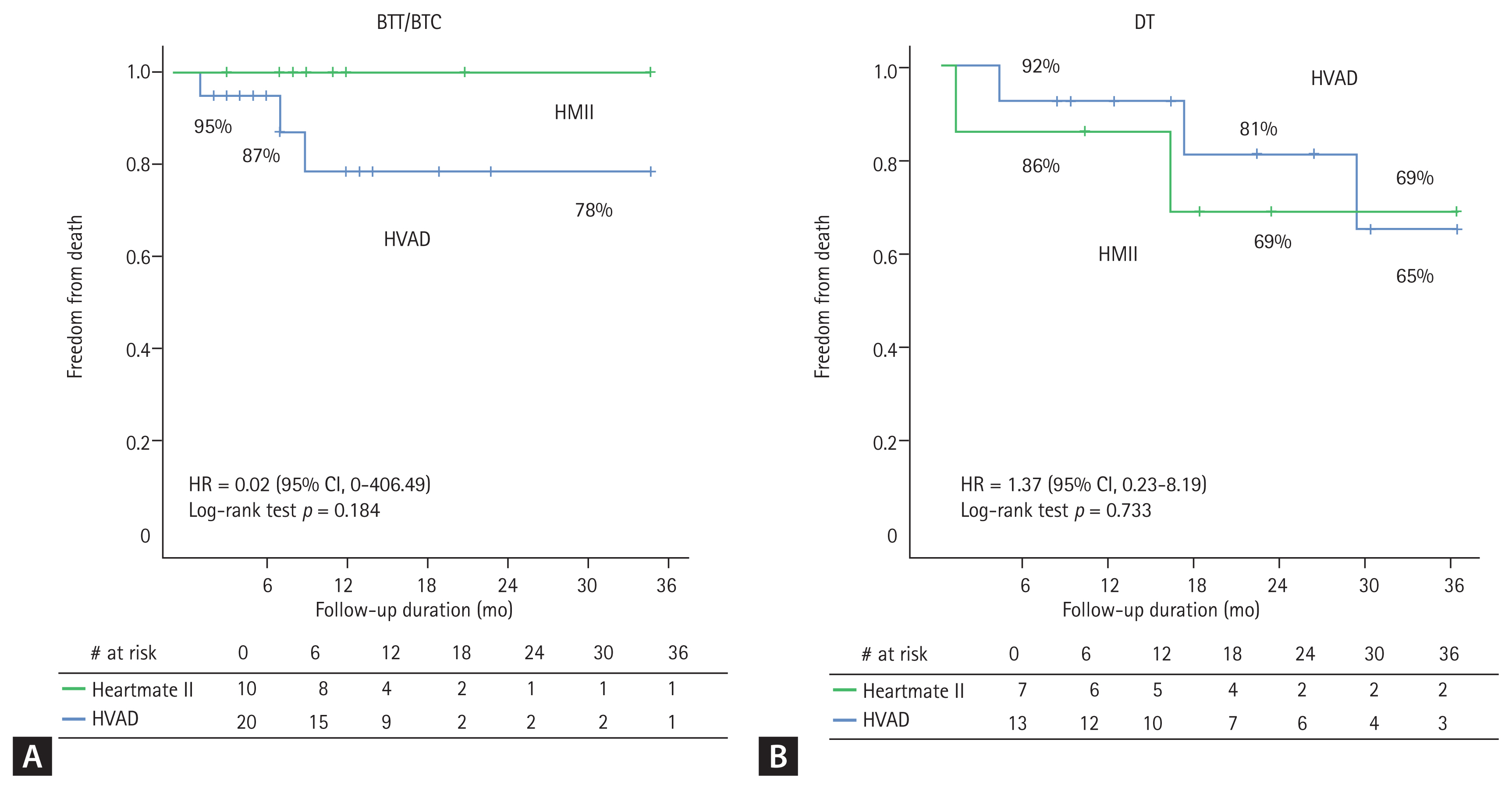
Overall survival stratified by implanted device is depicted in Fig. 2. There was no significant difference in overall survival according to device type, even when grouped by intention of implantation (Fig. 3). Of the 30 patients who underwent LVAD as BTT/BTC, 22 (73.3%) underwent HTx in a median of 10 months (IQR, 7 to 14). Estimates for receiving HTx were 46% at 12 months and 80% at 24 months. In the DT group, the median survival time was 22 months (IQR, 13 to 37).
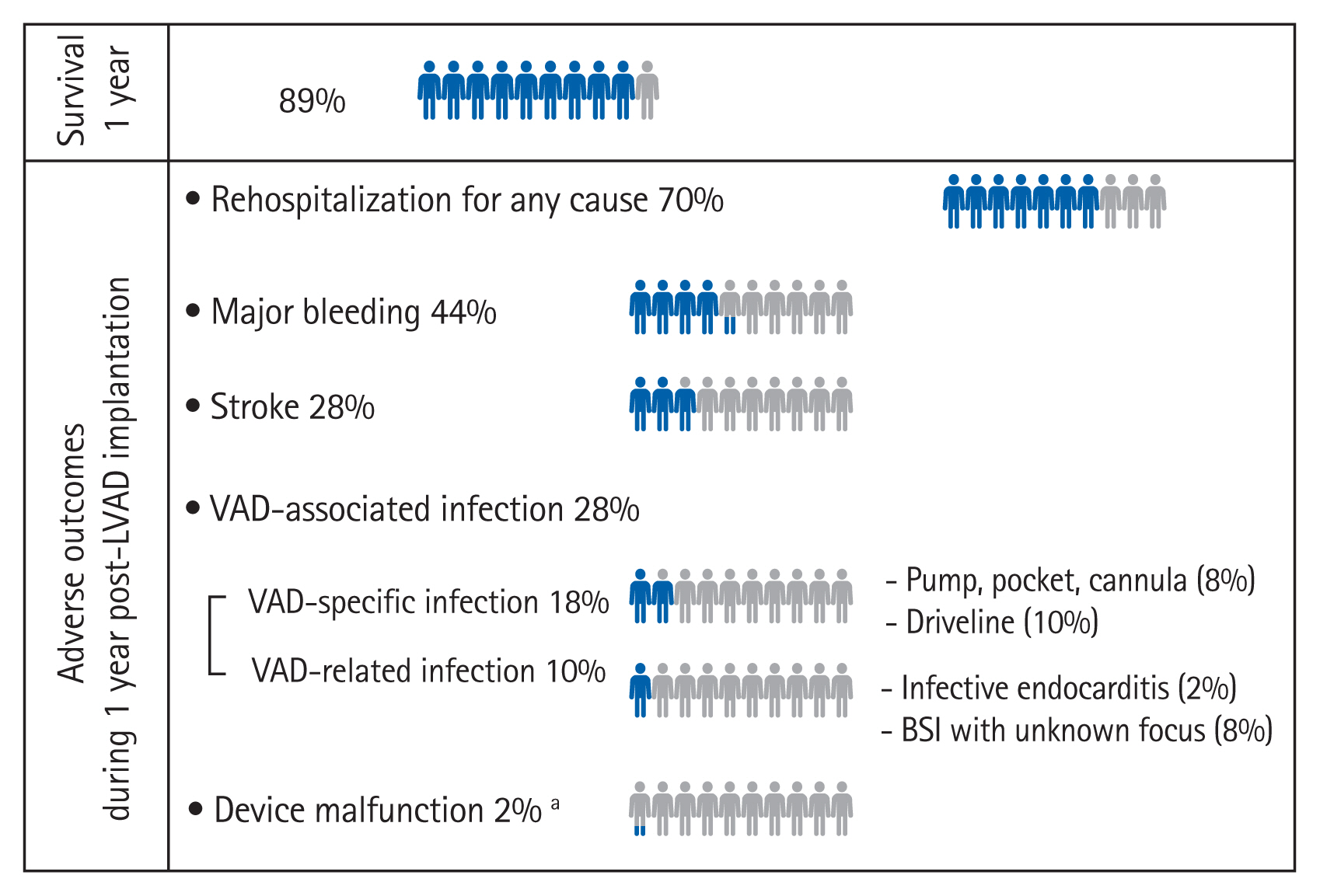
Fig. 4 summarizes the benefit and risk of LVAD implanted patients at the first year of LVAD implantation. The most common adverse event during the first year was major bleeding (44%) and stroke (28%), followed by VAD-associated infection (28%). Among major bleeding events, gastrointestinal (GI) bleeding was the most common, followed by surgical site bleeding. Supplementary Table 5 shows comparisons of hemocompatibility-associated adverse events between HeartMate II (n = 17, 34%) vs. HVAD (n = 33, 66%) devices. Similar to previous studies, patients implanted with the HeartMate II device had similar rates of stroke or bleeding compared with those with the HVAD device (Supplementary Table 5). Among ventricular assist device (VAD)-associated infections, VAD-specific infection (18%) was the most common. There was one case of device malfunction due to alleged pump failure, which resulted in device exchange. RHF after surgery occurred in 22% of patients, one-third of which required right ventricular assist device (RVAD) insertion (8%).
Rehospitalizations
A total of 38 (76%) and 42 (84%) patients experienced rehospitalization within the first year of LVAD implantation and during follow-up, respectively. The most common cause of rehospitalization was GI bleeding. Time to rehospitalization or rehospitalization rates did not differ between the groups receiving HeartMate II versus HVAD or for patients with DT or BTT/BTC designations (Supplementary Table 6).
Subgroup clinical outcome analysis stratified by sex
Supplementary Table 7 describes clinical outcomes after LVAD implantation according to sex. All-cause mortality (Supplementary Fig. 1) and adverse events after LVAD implantation was similar in both sexes, but a significantly higher RHF was noted after surgery in women.
Subgroup clinical outcome analysis stratified by LVAD implant period (pre- vs. post-reimbursement)
Supplementary Table 8 describes the clinical outcomes after LVAD implantation according LVAD implantation periods (pre- vs. post reimbursement period). Patients who had underwent LVAD implantation in the pre-reimbursement period had a higher rate of RHF after surgery. However, all-cause mortality was similar between groups (Supplementary Fig. 2).
DISCUSSION
In this article, we summarized clinical outcomes of the initial 50 cases of cf-LVAD implantation from a single center for the first time in Korea. Survival of all LVAD patients was 89% at 1 year. In BTT/BTC patients, survival was 86% in 1 and 2 years post LVAD implantation. In DT patients, survival was 90 and 77% in 1 and 2 years post LVAD implantation, respectively. The most common cause of death was hemorrhagic stroke and 76% patients experienced rehospitalization during the first year after being discharged with LVAD implantation. The most common adverse event during the first year was major bleeding.
In our cohort, 94% patients were in the INTERMACS profile range of 1 to 3. According to the recent IMACS registry, 85% of implants were in patients in INTERMACS profile 1 to 3 [27], which reflects the lack of sufficient endorsement by clinicians in ambulatory HF patients considering the burden of adverse events. In our cohort, 44% of patients received LVAD as DT. In the IMACS registry, 70% patients underwent LVAD as DT [28]. With improvement of durability, safety profile, and outcomes, patients undergoing LVAD implantation as DT are increasing due to limited donors for HTx and an increasing number of end-staged HF patients. In our center, we are also experiencing increasing LVAD implantation as DT cases, amounting to a similar number to that of our BTT cases.
Implantation of cf-LVAD is a safe and effective treatment strategy for patients with end-stage HF who are refractory to medical therapy. In the United States, survival among all CF-VAD patients is currently 81% and 70% at 1 and 2 years post LVAD implantation, respectively [29]. In our cohort, survival showed similar results: 89% and 79% at 1 and 2 years post LVAD implantation, respectively. Survival rates were similar in BTT/BTC and DT patients. In the DT population, despite the advanced age and higher comorbidities that contraindicate them for HT, long-term outcomes were still satisfactory with 77% overall survival at 2 years, which is similar to the outcomes of recent IMACS registry [27]. In our cohort, survival without disabling stroke or reoperation of DT patients was 64% at 2 years (Supplementary Fig. 3), while in previously reported data from HVAD and HeartMate II trials, 46% to 59% of patients were able to achieve survival without disabling stroke or reoperation at 2 years [30ŌĆō32]. In this analysis, patients were implanted with either HeartMate II or HVAD devices. Results from Multicenter Study of MagLev Technology in Patients Undergoing Mechanical Circulatory Support Therapy With HeartMate 3 (MOMENTUM 3) demonstrated superiority of the HeartMate 3 device compared with HeartMate II, including a significant reduction in disabling stroke and hemocompatibility-associated adverse events, such as pump thrombosis, stroke of any type or severity, and nonsurgical bleeding [33]. The HeartMate 3 cohort recently achieved a 79% rate of survival without disabling stroke or reoperation at 2 years, owing to a significantly reduced stroke and pump thrombosis burden. With the recent approval of the HeartMate 3 device in Korea, outcomes are expected to improve as well in Korea.
Consistent with the previous IMACS registry, the most common cause of death from our cohort was hemorrhagic stroke [27]. Stroke incidence were similar between HeartMate II and HVAD (32.1% vs. 31.8%). This is consistent with the early results from The HeartWare Ventricular Assist System as Destination Therapy of Advanced Heart Failure (ENDURANCE II) trial reporting similar stroke rates between HVAD and HeartMate II devices, as long as blood pressure is well controlled [34]. Major bleeding was the most common adverse event in the first year of LVAD implantation and GI bleeding was the most common bleeding event, consistent with previous reports. Among VAD-associated infections (n = 14), superficial driveline infection was the most common focus (n = 4, 28.6%). A significant proportion of patients (76%) experienced rehospitalization at the first year after LVAD implantation. This was comparable to readmission rates in other registries, which were reported to be approximately 55% to 81% [35ŌĆō37]. In our cohort, the most common cause of readmission was GI bleeding (n = 4, 9.5%). High rates of rehospitalization remain to be profound clinical and economic considerations in LVAD patients, which is expected to be improved with HeartMate 3.
Notably, women were unlikely to receive LVAD compared to men and baseline NT-proBNP was significantly higher than men at the time of LVAD implantation. Due to smaller body size, all women underwent HVAD implantation. Women experienced significantly more RHF after LVAD implantation. LVAD implantation at relatively more severe HF in women, as well as smaller chamber size may increase risk of RHF in women due to increased vulnerability to pressure changes with the LVAD.
Limitations
This study is the result of a small number of patients from a single center and carries the innate limitations of observational data. The small number of patients in our study limited statistically significant multivariable analysis. However, our results are meaningful considering this registry data reports early experience from a leading center in Korea. Our data could be used to help make decisions for end-stage HF patients and their physician, especially in the era where LVAD implantation as DT is increasing worldwide. As the number of LVAD cases are rapidly increasing, our results could contribute to increasing evidence of clinical benefit from LVAD implantation in Korea. A multi-center national LVAD registry is strongly needed to provide information for quality control/improvement after LVAD implantation and to provide prognostic information for long term clinical outcome of LVAD patients in Korea.
KEY MESSAGE
1. This is the first domestic report on 50 cases of continuous flow left ventricular assist device (cf-LVAD) implantations from a single center in Korea.
2. With creditable survival and adverse event rates, our results support the use of LVAD for bridge to transplantation and destination therapy.
3. With the newer generation LVAD and a dedicated team approach, clinical outcomes of LVAD for end-stage heart failure could be improved.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





