


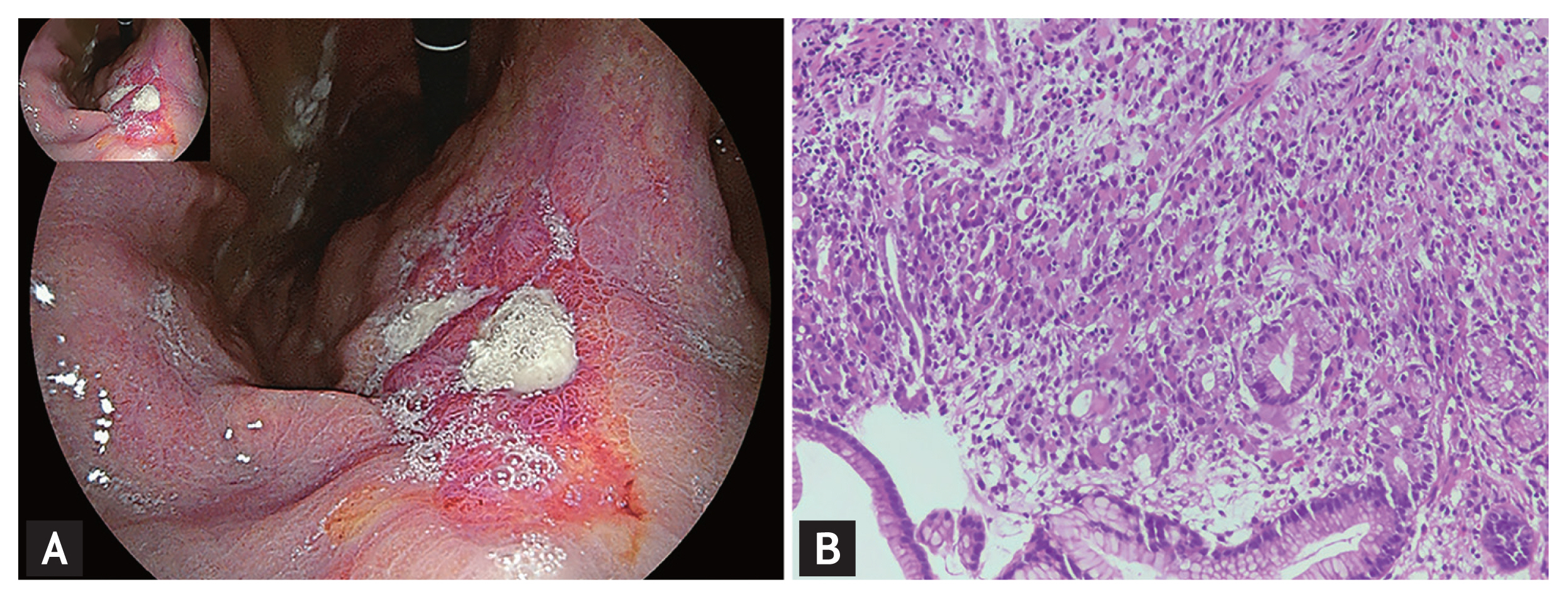
A 65-year-old female suffering from epigastric discomfort and weight loss was admitted to our hospital. She had a history of hepatolithiasis. Laboratory tests revealed that serum levels of carbohydrate antigen 72-4 (CA72-4), CA19-9, and carcinoembryonic antigen were significantly increased. Gastroscopy was indicated and a large ulcer at the gastric angle was identified (Fig. 1A). Pathological examination of the biopsy tissue confirmed the diagnosis of signet ring cell carcinoma (Fig. 1B). A subsequent abdominal computed tomography (CT) revealed a large liver mass and multiple enlarged regional lymph nodes, making advanced gastric cancer our primary concern. 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) was performed for further staging. An intense FDG-avid liver mass, multiple hypermetabolic lymph nodes and bone lesions were identified (Fig. 2A–C). Intriguingly, there was only faint FDG uptake at the signet ring cell carcinoma of the stomach (Fig. 2D and 2E). In turn, we performed an ultrasonography-guided needle biopsy of the liver mass. Histopathologic examination and immunohistochemical staining validated the diagnosis of hepatic squamous cell carcinoma (Fig. 2F–H). Considering FDG PET/CT and ear, nose, and throat (ENT) examination were negative at the common primary sites of squamous cell carcinoma (nasopharynx, neck, lung, cervix, and skin) and the distribution patter of the metastatic lymph nodes, the diagnosis of advanced primary hepatic squamous cell carcinoma was established.
The incidence of primary hepatic squamous cell carcinoma is extremely low and its pathogenesis has not been fully elucidated. The major etiological factors are associated with chronic inflammatory conditions such as hepatic cyst, hepatolithiasis. Secondary squamous metaplasia may be originated from chronic inflammation and lead to malignant transformation. 18F-FDG PET/CT is an important whole-body image tool for differential diagnosis, accurate staging and therapeutic response monitoring of digestive system malignancies. However, the sensitivity and specificity depend on the primary origins. Most squamous cell carcinomas demonstrate high FDG uptake, in contrast, signet ring cell carcinoma is often characterized by low glucose metabolism. This case exemplifies FDG PET/CT could be helpful for identifying multiple primary origins of digestive system malignancies, especially aggressive malignancies with high metastastic potential. Furthermore, it emphasizes a good correlation between intensity of FDG uptake and histologic subtypes of tumors.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institution and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was obtained from the patient for the anonymous use of patient clinical, imaging, and histologic data.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





