


INTRODUCTION
Existing data suggests a difference in the risk profile of Asian and Caucasian patients, with the Asian population having a higher risk for stroke, and a greater stroke-related morbidity and mortality [1ŌĆō3]. In Korea, the prevalence of non-valvular atrial fibrillation (NVAF) in all population reached 1.5% in 2015, which was more than doubled that seen in 2006 [4]. Accordingly, it is important to consider not only the increase in overall prevalence of atrial fibrillation (AF) in Korean population, but also the increase in the proportion of elderly population as well as mean CHA2DS2-VASc score [5].
In a randomized double-blind event-driven Phase III global study (Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation [ROCKET AF]), rivaroxaban was compared with warfarin for the prevention of stroke and embolism in patients with NVAF. This study demonstrated that rivaroxaban was similar to warfarin for stroke prevention in patients with NVAF, with a substantial lower risk of hemorrhagic stroke and intracerebral hemorrhage [6]. In addition, a secondary analysis of results from randomized patients in four geographic areas in East Asia (China, Korea, Taiwan, and Hong Kong) who participated in the full ROCKET AF study was performed. In this ROCKET AF East Asian cohort, the efficacy and safety of rivaroxaban versus warfarin have been shown to be similar among patients within and outside East Asia, and 20 mg once daily of rivaroxaban was suggested for stroke prevention in East Asians with NVAF [7]. In a subsequent prospective, observational clinical study which investigated the safety and effectiveness of rivaroxaban under routine practice in patients with NVAF in Europe, Israel and Canada (Xarelto for Prevention of Stroke in Patients with Atrial Fibrillation [XANTUS]), patients receiving rivaroxaban had a low rate of stroke (0.7 per 100 patient-years) and major bleeding (2.1 per 100 patient-years) [8].
In Korea, rivaroxaban use in AF patients was approved in 2013, but national insurance reimbursement was substantially limited. In 2015, however, the reimbursement of rivaroxaban was expanded to AF patients with CHA2DS2-VASc score of 2 or more [9].
Nevertheless, real-world evidence is increasingly being recognized as an essential component of the clinical evidence base, to complement phase III data in unselected patient populations and provide additional safety information after approval of new drugs [10], therefore the evaluation for the safety and effectiveness in routine clinical practice is required.
This current report is a sub-analysis of Korean patients of the Xarelto (Bayer AG Pharmaceuticals, Berlin, Germany) for prevention of stroke and non-central nervous system systemic embolism (CNS SE) in patients with NVAF in Asia: A non-interventional study (XANAP), which was conducted in 10 Asian countries [10]. XANAP is the first prospective, observational study to investigate the safety of rivaroxaban use in routine clinical practice in Asia, including Korea. Of 2,273 patients enrolled in XANAP, 844 were enrolled in Korea, which was the single largest contribution among the participating countries. The main goal of this analysis was to investigate safety and effectiveness of rivaroxaban use in clinical practice in Korea and to estimate incidences for treatment-emergent safety events including major bleeding, adverse events (AEs), serious adverse events (SAEs) and all-cause mortality under rivaroxaban in a real-life setting.
METHODS
XANAP was a prospective, observational cohort study of patients with NVAF starting rivaroxaban treatment to prevent stroke or non-CNS SE, conducted in 10 Asian countries. This analysis evaluated the safety and effectiveness outcomes among 844 Korean patients included in XANAP, subsequently referred to as XANAP Korea. This study was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital (IRB No. ED13010) and each IRB of participating hospital.
Study population
Eight hundred and forty-four eligible Korean patients were enrolled at 54 investigational sites aged 18 years or older with the diagnosis of NVAF who provided written informed consent forms (ICFs) to participate in this study, were enrolled from 54 sites in South Korea and started rivaroxaban treatment for the prevention of stroke or non-CNS SE.
Medication and follow-up
In XANAP, rivaroxaban treatment for patients was decided by his or her treating physicians. The approved dose of rivaroxaban was 20 mg once daily for patients with creatinine clearance (CrCl) Ōēź 50 mL/min and 15 mg once daily for patients with CrCl 15 to 49 mL/min in Korea [11]. Patients were followed for up to 1 year in XANAP.
Study outcomes
The primary outcomes measured focused on the safety of rivaroxaban, including: treatment-emergent AEs, SAEs, all-cause mortality, and major bleeding events, which were defined using the International Society on Thrombosis and Hemostasis criteria. Secondary outcomes included non-major bleeding, thromboembolic events, hospitalization due to bleeding or thromboembolic events, persistence with rivaroxaban treatment, and reasons for interruption of rivaroxaban treatment. An independent Central Adjudication Committee was convened to adjudicate the endpoints of major bleeding events, stroke, cause of death, transient ischemic attack (TIA), non-CNS SE, and myocardial infarction (MI).
Study governance
The XANAP study was conducted in accordance with the Good Pharmaco-epidemiological Practice. An independent academic steering committee oversaw the design and conduct of the study.
Statistical analysis
Descriptive statistical analyses were performed on the safety population which included all patients who took at least one dose of rivaroxaban during the observation period. When rivaroxaban was stopped during the follow-up, clinical events were considered treatment-emergent until 2 days after end of rivaroxaban treatment and included in the analyses. Statistical analyses were explorative and descriptive. Incidence proportions (number of patients with events/number of treated patient) with 95% Pearson-Clopper confidence interval (CI) and incidence rate (number of patients with at least one event divided by the cumulative person time at risk per 100 patient-years) with 95% poisson rate CIs were estimated.
RESULTS
Patients population
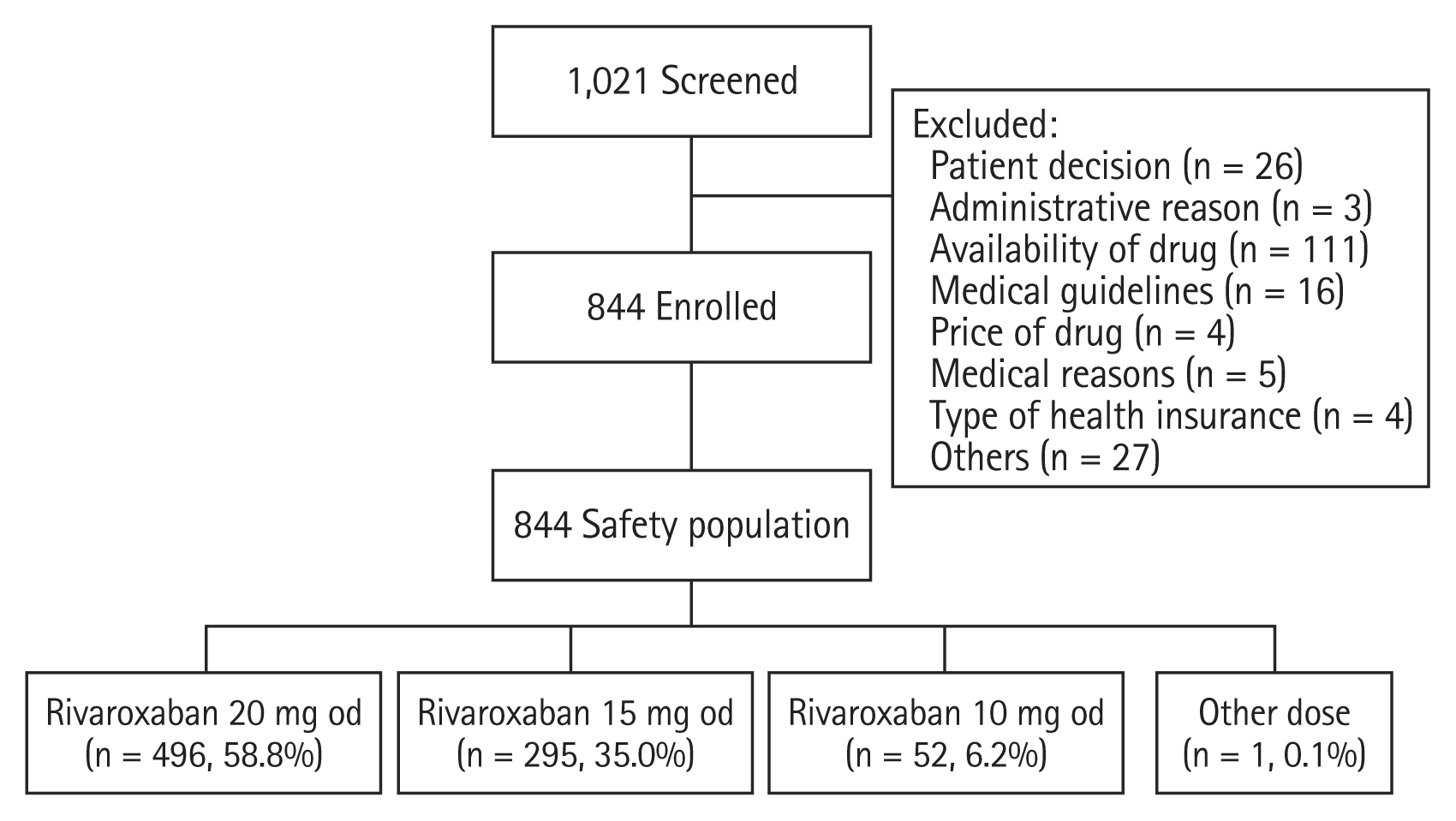
Of 1,021 patients screened, a total of 844 patients were enrolled in the Korean portion of the XANAP study (Fig. 1). Table 1 presents baseline demographic and clinical characteristics of the included patients in XANAP Korea. In XANAP Korea, the mean age ┬▒ standard deviation (SD) was 70.1 ┬▒ 10.7 years and 62.6% were males. Of the included patients, 47.0% had a history of prior stroke/TIA or non-CNS SE. The mean CHADS2 score was 2.5 ┬▒ 1.4 and the mean CHA2DS2-VASc score was 3.8 ┬▒ 1.9.
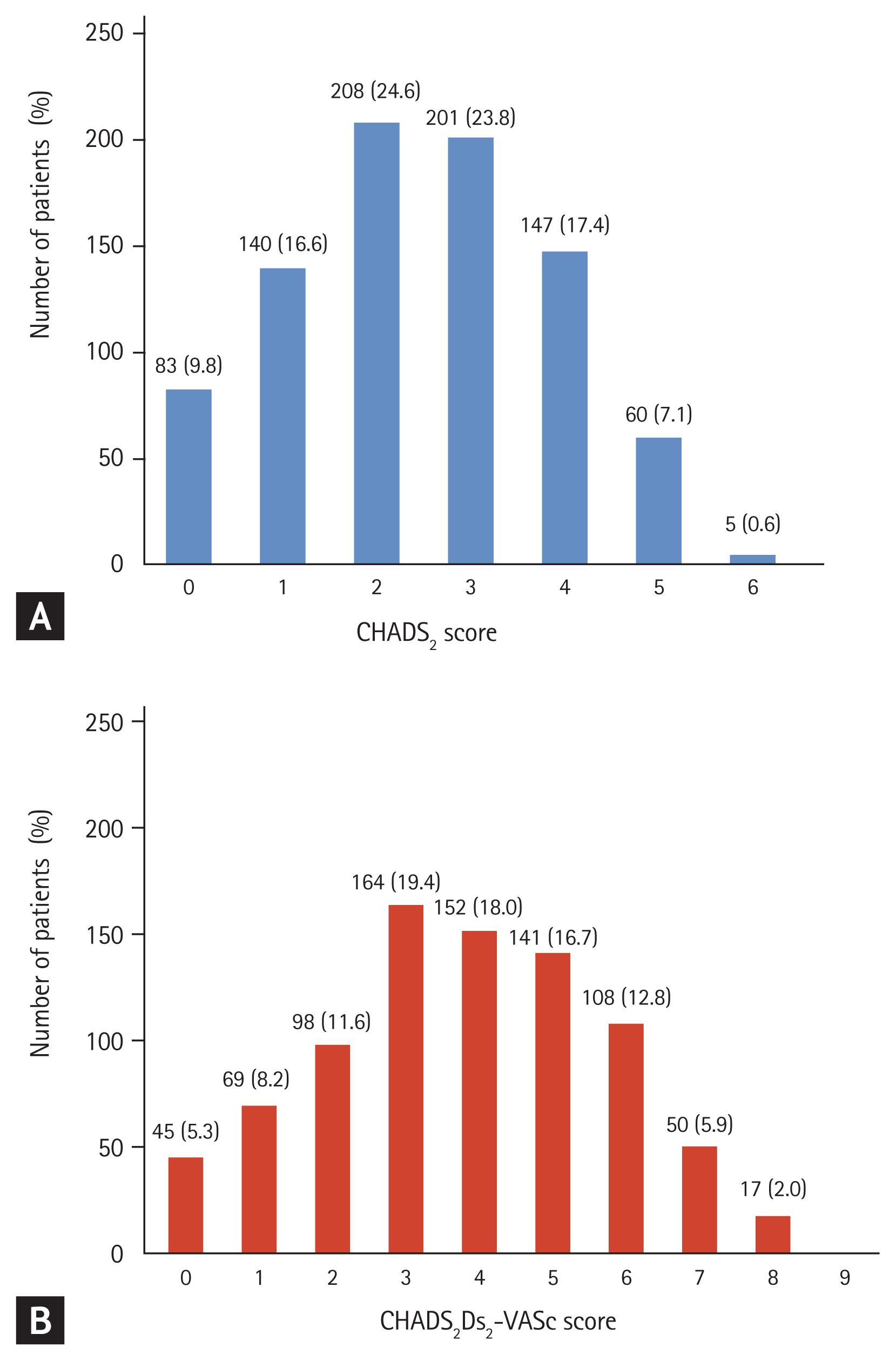
Fig. 2 shows the distribution of the CHADS2 and CHA2DS2-VASc scores of the study population at baseline in XANAP Korea. Of 844 patients, 208 patients (24.6%) and 201 patients (23.8%) had a CHADS2 score of 2 and 3, respectively. One hundred and forty-seven patients (17.4%) had a CHADS2 score of 4. Sixty patients (7.1%) and five patients (0.6%) had a CHADS2 score of 5 and 6, respectively. One hundred and sixty-four patients (19.4%) and 152 patients (18.0%) had a CHA2DS2-VASc score of 3 and 4, respectively.
In XANAP Korea, the median treatment duration was 338.5 days. The number of patients with at least one interruption was 48 (5.7%). The main reasons for the total of 51 interruptions of treatment were surgery (n = 17), bleeding (n = 10), AE excluding bleeding (n = 7), patient decision (n = 4), and supply issue due to health system (n = 8).
Outcomes
In this study, a total of 283 patients (33.5%) had a treatment-emergent AE (incidence rate, 54.8 per 100 patient-years; 95% CI, 48.6 to 61.6) and 89 patients (10.5%) had a treatment-emergent SAE (incidence rate, 14.6 per 100 patient-years; 95% CI, 11.7 to 17.9). Seven patients (0.8%) had adjudicated treatment-emergent major bleeding events (incidence rate, 1.1 per 100 patient-years; 95% CI, 0.4 to 2.2) and two patients (0.2%) had a fatal bleeding event (incidence rate, 0.3 per 100 patient-year; 95% CI, 0.0 to 1.1). Among the major bleeding events, there were five intracranial hemorrhages in four patients and two gastrointestinal bleedings. Incidence proportion of non-major bleeding was 8.4% (incidence rate, 11.6 per 100 patient-years; 95% CI, 9.1 to 14.6) (Table 2). There was a numerically higher incidence proportion of any bleeding reported by the investigator in 15 mg rivaroxaban treatment versus 20 mg (10.5% vs. 8.3%).
Incidence proportion of thromboembolic events was 1.5% (incidence rate, 2.0 per 100 patient-years; 95% CI, 1.1 to 3.5). Incidence proportions of stroke was 1.2% (incidence rate, 1.6 per 100 patient-years; 95% CI, 0.7 to 2.9), that of non-CNS SE was 0.1% (incidence rate, 0.2 per 100 patient-years; 95% CI, 0.0 to 0.9), and that of MI was 0.2% (incidence rate, 0.3 per 100 patient-years; 95% CI, 0.0 to 1.1).
There were 10 adjudicated treatment-emergent deaths in the Korean subgroup (1.2%). Investigator reported adverse events leading to death were death due to unknown cause, pneumonia, femur fracture, cardiac arrest, subdural hemorrhage, hemorrhagic transformation stroke, coma, septic shock, cerebral infarction, renal failure, uterine cancer, and depressed level of consciousness. Some patients had more than one fatal AE documented.
The total of 11 patients were hospitalized due to drug related SAE. Among them, eight (0.9%) patients were hospitalized due to thromboembolic events and seven (0.8%) patients due to bleeding events (Table 3).
DISCUSSION
XANAP Korea investigated 844 NVAF Korean patients treated with rivaroxaban for the prevention of stroke and non-CNS systemic embolism. There were three main findings. First, patients included in this analysis had a high risk of stroke with a mean CHADS2 and CHA2DS2-VASc score of 2.5 and 3.8. Second, the incidence of major bleeding was low and 99% of patients did not experience any treatment-emergent major bleeding. Third, there was no new safety concern identified. No new AE or SAE was observed under routine clinical practice in Korea.
In Korea, with increasing age, the ischemic stroke incidence rate per 100,000 person-years steeply increased from 6 in population aged younger than or equal to 44 years old to 2,075 in those aged older than or equal to 85 years old [12]. AF-related stroke accounts for 20% of ischemic strokes [13]. The prevalence of nonvalvular AF reached 1.5% in 2015, which is more than double that seen in 2006 [4]. This might be explained by growing aged population, increased AF awareness and early detection of AF [14].
The XANAP study is the first prospective, observational study to investigate the safety of rivaroxaban use in routine clinical practice in Asia, including Korea. XANAP Korea analyzed 844 NVAF Korean patients treated with rivaroxaban for the prevention of stroke and non-CNS SE, as part of the larger Asian XANAP study.
Compared to XANTUS and XANAP overall, there were more patients with a prior history of stroke/non-CNS SE/TIA (19.0% in XANTUS, 32.8% in XANAP overall, and 47.0% in XANAP Korea) and there were more patients with a prior vitamin K antagonist use (40.8% in XANTUS, 35.8% in XANAP overall, and 57.8% in XANAP Korea) in XANAP Korea. Patients in XANAP Korea had a higher risk of stroke compared to XANAP and XANTUS with a mean CHADS2 and CHA2DS2-VASc score of 2.5 and 3.8, respectively compared to 2.0 and 3.4 in XANTUS and 2.3 and 3.7 in XANAP overall (Table 4). This Korean patient characteristics appear to be affected by the specific cause, such as the Korea National Health Insurance reimbursementŌĆÖs limitation during the patient recruitment period.
Despite of the higher risk for stroke, the incidence rate of thromboembolic events in XANAP Korea was comparable to XANTUS (2.0 per 100 patient-years vs. 1.8 per 100 patient-years) and it was numerically lower than in XANAP overall (2.6 per 100 patient-year) [10]. These differences may have been influenced by clinical practice difference and difference of baseline characteristics such as having fewer patients with congestive heart failure or with hypertension compared to XANAP overall and XANTUS (Table 4).
In addition, XANAP Korea showed lower mean CHADS2 score compared to ROCKET AF (2.5 vs. 3.5, respectively), however, similar incidence rate of stroke or systemic embolism (2.0% vs. 2.1% for ITT) [7]. The results from XANAP Korea cannot be directly compared with those of the phase III ROCKET AF study because observational studies do not select patients based on strict inclusion criteria. In contrast, phase III studies typically exclude patients with competing co-morbidities, such as active cancer or short life expectancy. The baseline characteristics of patients enrolled in these trials and the follow-up periods were different; therefore, it is difficult to make meaningful comparisons of incidence rates between such different types of studies [10].
In XANAP Korea, 99% of patients with a mean CHADS2 score of 2.5 receiving rivaroxaban did not experience any treatment-emergent major bleeding. There was low adjudicated treatment-emergent major bleeding incidence of 0.8% (1.1 per 100 patient-years) and non-major bleeding of 8.4% (11.6 per 100 patient-years) in real clinical practice (Table 2).
In this Korean subgroup, numerically higher incidence proportion of treatment-emergent bleeding were observed in patients on 15 mg rivaroxaban treatment as compared to those on 20 mg (10.5% vs. 8.3%). This is likely attributed to the greater pre-existing co-morbidities of those patients on 15 mg. This is similar to the findings in both XANAP and XANTUS, where the authors similarly concluded that the dosing decision might have been based on other clinical considerations besides impaired renal function [8,10]. The dose reduction is not recommended for any other criteria except for renal impairment [11].
In this analysis, a total of 844 patients were enrolled. Overall, 99% of patients with a mean CHADS2 score of 2.5 receiving rivaroxaban did not experience any treatment-emergent major bleeding and the incidence rate of stroke among these patients were low. There was no new AEs or SAEs observed in the study.
The main limitation of this analysis was a relatively high proportion of patients (48.7%) with missing renal function data, similar to those observations in the XANAP (48.5%) and the XANTUS study (34.4%) [8,10]. Therefore, it is unknown if patients with missing CrCl levels were dosed per label recommendation or not; such a lack of information is a common drawback of real-world studies. As it was mentioned in the Method section, all treatment decisions including dosing and duration of treatment were at the sole discretion of the attending physician, thus, patients could be enrolled regardless of label recommendation.
Other limitations of this study were confined to those typical of the observational setting, i.e., observational studies may often be limited in their ability to account for confounding and bias due to patient selection [15]. However, allowance for real world factors better reflect the real clinical situations than clinical study, and greater allowance for ŌĆ£real worldŌĆØ factors, enable the detection of potential safety signals that may not be apparent in a clinical study setting. In addition, the independent, central endpoint-adjudication is expected to reduce reporting bias.
In conclusion, we reaffirmed the consistent safety for rivaroxaban in this study. We found consistent results with overall XANAP population for rivaroxaban in terms of safety in NVAF patients for the prevention of stroke and non-CNS SE.
KEY MESSAGE
1. Xarelto for Prevention of Stroke in Patients with Atrial Fibrillation in Asia-Pacific (XANAP) Korea is the first prospective, observational study to describe rivaroxaban use in a broad patient population with non-valvular atrial fibrillation in Korea.
2. The incidence rates of major bleeding, death and stroke with rivaroxaban were found to be low in routine clinical practice in Korea.
3. The safety and effectiveness outcomes found in this study were consistent with those of overall XANAP population.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





