


INTRODUCTION
Erectile dysfunction (ED) is defined as a consistent or repetitive inability to obtain or maintain a penile erection of sufficient rigidity and duration for sexual intercourse [1]. ED is highly prevalent worldwide, currently affecting 150 million men and 322 million by the year 2025 [2]. Approximately half of men over 70 years of age have ED with moderate to severe symptoms [3,4] and thus experience poor quality of life [5]. Sarcopenia, which is characterized by decreased muscle mass, strength and/ or physical performance, is an important risk factor for an adverse health outcome and poor quality of life [6-9].
Except for the mechanism of direct damage to the nerves associated with erection, various causes, including vascular, psychogenic, and hormonal factors, are associated with ED. Among the vascular factors, cardiovascular disease (CVD), hypertension, diabetes mellitus, dyslipidemia, and smoking are well-known risk factors for ED [3,4,10]. Hormonal and psychogenic factors are represented by decreased androgen hormone level and depression [1].
Androgen hormone was known to be one of the causes of ED and sarcopenia. Although the diagnosis of ED and low androgen hormone could be uncertain, erections are androgen-dependent, and androgen replacement therapy for a patient with a low bioavailable androgen level has been confirmed [1,11,12]. Sarcopenia can be associated with low androgen levels because low levels of androgen are associated with decreased anabolism of skeletal muscle. Also, as a treatment for sarcopenia, supplementation of androgen hormone has been suggested [13,14]. However, it is not clear whether sarcopenia is an independent risk factor for ED. Only the association between ED and sarcopenia in men with diabetes has been reported in a previous study [15].
Therefore, the aim of this study is to analyze the relationship between sarcopenia and ED in a community setting. We prospectively assessed sarcopenia and ED over a 1-year period in order to investigate the association of sarcopenia and its components with prevalent and incident ED, excluding the established risk factors for ED in community-dwelling older men.
METHODS
Study population and design
The population of this study was analyzed from the Aging Study of Pyeongchang Rural Area (ASPRA), a population-based, prospective cohort study of frailty and geriatric syndromes that has covered 1,650 community-dwelling, older adults since December 2014 [16]. The detailed design and method of ASPRA have been described elsewhere [16,17]. Briefly, older adults residing in Pyeongchang County, Gangwon Province, Korea, located 180 km east of Seoul, were enrolled through public healthcare networks. Comprehensive geriatric assessments were performed annually. The inclusion criteria for participation in ASPRA were (1) age Ōēź 65 years, (2) registered in the National Healthcare Services, (3) ambulatory with or without an assistive device, (4) living at home, and (5) able to provide informed consent. The exclusion criteria were (1) living in a nursing home, (2) hospitalized, or (3) bed-ridden and receiving nursing-home-level care at the time of their enrollment. We have shown that the ASPRA cohort included over 90% of the eligible population in the study area, and the characteristics of the participants were comparable to those of a nationally representative sample of the Korean rural population, except for a higher proportion with agriculture as an occupation and a lower proportion with a formal education [16].
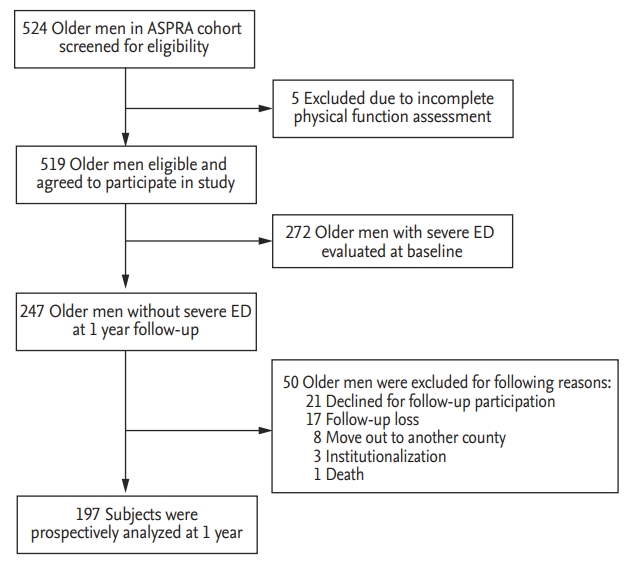
Of the total of 524 men who participated in the ASPRA cohort, as five were excluded due to incomplete physical function assessment, we analyzed the data from 519 (99.0%) men who completed assessments for ED between January 1, 2016 and December 31, 2017 for the present study. Of these 519 men, 272 with severe ED were evaluated at baseline. Those without severe ED at baseline (n = 247) were prospectively analyzed. After 1 year, 50 men were excluded due to follow-up loss, i.e., 21 who declined follow-up participation, 17 follow-up loss, eight who moved to another county, three who were institutionalized, and one who died. Therefore, the remaining 197 men were evaluated (Fig. 1). The protocol of this study was approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (IRB No. 2015-0673). Written informed consent was obtained from all participants.
Measurement of erectile dysfunction
The five-item version of the International Index of Erectile Function (IIEF) was used to evaluate sexual desire and ED with a scoring range of 5 to 25 [18]. Male physicians administered the IIEF-5 questionnaire to participants in a private area. Based on the IIEF-5 score, participants were classified as having severe ED (5 to 7), moderate ED (8 to 11), mild to moderate ED (12 to 16), mild ED (17 to 21), or no ED (22 to 25) [18]. The outcome of interest was severe ED because severity of erectile dysfunction is associated with poorer life quality [5] and a higher prevalence of frailty was observed in men with severe ED [19].
Measurement of sarcopenia
Nurses with specific, related training conducted measurements of muscle mass, grip strength, and gait speed to assess sarcopenia.
Muscle mass
Bioelectrical impedance analysis (InBody 620; InBody, Seoul, Korea) with measuring frequencies of 5, 50, and 500 kHz was used to evaluate body composition including the total mass and the lean mass. Bioelectrical impedance analysis was previously validated against dual-energy X-ray absorptiometry [20]. All of the patients were asked to fast overnight and four-limb impedance was measured by the device with the patient in a standing position. Appendicular skeletal muscle mass (ASM) was calculated as the sum of the lean mass of both arms and legs provided by the manufacturerŌĆÖs algorithm. ASM was divided by the height squared (ASM/ht2) in order to allow comparison of the muscle mass between the participants.
Grip strength
A spring-based dynamometer (T.K.K. 5401 Grip-D; Takei, Tokyo, Japan) was used to assess the handgrip strength (kg) in both arms [21]. Participants were asked to hold the dynamometer as strongly as possible while in a comfortably sitting position with their arm bent 90┬░ over the knee [22]. All tests were conducted twice at intervals more than one minute. The maximum value from the dominant arm was used for the analysis.
Gait speed
In order to evaluate the usual gait speed, participants were instructed to walk a total of 7 m on a level indoor surface and at the pace most comfortable and usual for them. A trained tester measured the 4 m distance transit time using a digital stopwatch between the first foot step at the starting line and the first footstep at the 4 m line. The 1.5 m intervals of each acceleration and decelerating section were excluded from the measurement [8]. The result was reported according to the gait speed (m/sec) [23].
Definition of sarcopenia
We determined sarcopenia according to the Asian Working Group for Sarcopenia consensus algorithm. Briefly, among older adults with low handgrip strength and/or slow gait speed and who has low muscle mass at the same time was classified as having sarcopenia [8]. Decreased muscle mass was defined as the sex-specific lowest quintile of ASM/ht2 [8,24], which has been widely adapted in sarcopenia definitions, and the clinical relevance of this measure in the ASPRA population has previously been reported [25]. Decreased grip strength was defined as handgrip strength less than 26 kg for men and less than 18kg for women. Slow gait speed was defined as gait speed less than 0.8 m/sec [8].
Other measurements
Other geriatric conditions were assessed by trained nurses using standardized instruments. Disability was defined as requiring assistance in performing any of the seven activities of daily living (ADL), i.e., ADL, bathing, continence, dressing, eating, toileting, transferring, and washing face and hands, or the 10 instrumental activities of daily living (IADL), i.e., IADL, food preparation, household chores, going out a short distance, grooming, handling finances, laundry, managing their own medications, shopping, transportation, and using a telephone [26]. Cognitive dysfunction was determined if the score on the Korean version of the Mini-Mental State Examination was < 24 [27]. Depression was determined if the score on the Korean version of the Center for Epidemiological Studies Depression scale was Ōēź 21 [28]. A risk for malnutrition was defined as a Mini-Nutritional Assessment-Short Form score of Ōēż 11 points [29]. Underlying comorbidities, i.e., hypertension, diabetes mellitus, CVD, and dyslipidemia, a history of falling down during the past year, and the amount of cigarette smoking were self-reported by participants. CVD was defined as a participant with any of the following: hypertension; any heart disease, e.g., ischemic heart disease, heart failure, a history of stroke, and dyslipidemia.
Statistical analysis
Baseline characteristics were compared between the participants with and those without sarcopenia, using a two-sample t test for continuous variables and a chisquare test for categorical variables. We examined the prevalence of ED in those with and those without sarcopenia at baseline. Logistic regression was used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for severe ED associated with sarcopenia and the three sarcopenia components, after adjusting for patient age, smoking, CVD, diabetes, depression, and polypharmacy. Among those without severe ED at baseline, we examined the incidence of severe ED in those with and those without sarcopenia and its components. The ORs and 95% CIs for incident-severe ED associated with sarcopenia and its components were estimated using logistic regression to adjust for the above-mentioned variables. Statistical analysis was performed using SPSS version 18.0 (IBM Corporation, Armonk, NY, USA). A two-sided p value < 0.05 was considered statistically significant.
RESULTS
Characteristics of study participants
The study population included 519 men with a mean age of 74.0 years (standard deviation, 5.8) and 164 (31.6%) with sarcopenia. Severe ED was present in 272 men (52.4%) at baseline. Compared with the non-sarcopenic men, those with sarcopenia were older (mean age, 77.3 years vs. 72.4 years; p < 0.001) and had a poorer health status based on a higher prevalence of cognitive dysfunction (35.4% vs. 7.9%, p < 0.001), higher risk of malnutrition (56.1% vs. 20.6%, p < 0.001), ADL disability (14.6% vs. 6.5%, p < 0.003), and IADL disability (25.6% vs. 9.9%). Other comorbid conditions were not statistically different (Table 1).
Association of sarcopenia and each sarcopenia component with prevalent erectile dysfunction
The prevalence of severe ED at baseline was higher in sarcopenic men (73.2% vs. 42.8%; OR, 3.64; 95% CI, 2.45 to 5.50; p < 0.001) (Table 2). The association was attenuated with adjustment for age (OR, 2.01; 95% CI, 1.29 to 3.16; p = 0.002) and additionally for smoking, CVD, diabetes mellitus, depression, and polypharmacy (OR, 1.89; 95% CI, 1.18 to 3.03; p = 0.008).
Each sarcopenia component was associated with severe ED after adjusting the other components: the ORs were 2.39 (95% CI, 1.58 to 3.60; p < 0.001) for decreased muscle mass, 1.73 (95% CI, 1.12 to 2.66; p = 0.013) for slow gait speed, and 2.43 (95% CI, 1.56 to 3.80; p < 0.001) for decreased grip strength (Table 2). The associations were attenuated with adjustment for age and additional risk factors for ED. The association of decreased muscle mass with severe ED remained statistically significant (OR, 1.63; 95% CI, 1.03 to 2.60; p = 0.039). The OR for decreased grip strength was similar, but not statistically significant (OR, 1.51; 95% CI, 0.92 to 2.48; p = 0.107).
Association of sarcopenia and each sarcopenia component with incident erectile dysfunction
Out of 197 patients, the 1-year incidence of severe ED was 26.4% (n = 52). Among the 52 patients with severe ED, 22.7% (n = 37) were without sarcopenia and 44.1% (n = 15) had sarcopenia (OR, 2.69; 95% CI, 1.25 to 5.81; p = 0.012). However, the association between sarcopenia and incident severe ED was attenuated with adjustment for patient age (OR, 1.70; 95% CI, 0.73 to 3.95; p = 0.215) and other risk factors (OR, 1.87; 95% CI, 0.79 to 4.43; p = 0.155) (Table 3).
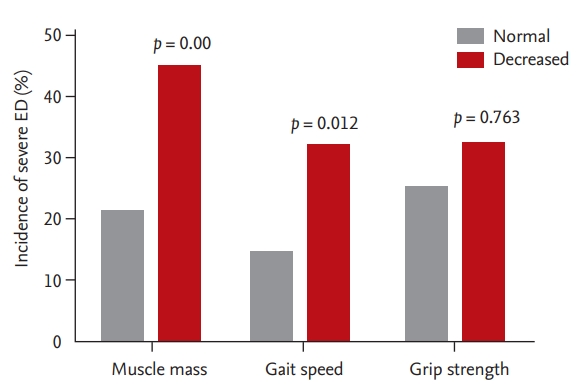
According to each sarcopenia component, the incidence of severe ED was higher in men with decreased muscle mass (45.2% vs. 21.3%; OR, 3.02; 95% CI, 1.43 to 6.35; p = 0.004) and slow gait speed (32.1% vs. 14.3%; OR, 2.84; 95% CI, 1.26 to 6.39; p = 0.012) compared to those with normal muscle mass and normal gait speed (Fig. 2). Therefore, the difference in the incidence of severe ED over weak grip strength was not significant (32.4% vs. 25.2%; OR, 1.14; 95% CI, 0.49 to 2.65; p = 0.763). Adjustment for age and additional risk factors moderately reduced the associations, but decreased muscle mass (OR, 2.54; 95% CI, 1.11 to 5.81; p = 0.027) and slow gait speed (OR, 2.80; 95% CI, 1.18 to 6.62; p = 0.019) remained significantly associated with severe ED. After adjustment, grip strength was not significantly associated with the incidence of severe ED (OR, 0.76; 95% CI, 0.30 to 1.91; p = 0.564).
DISCUSSION
In a population-based study of community-dwelling, older Korean men, we found that the prevalence of severe ED and sarcopenia was 52.4% and 31.6%, respectively. Our cross-sectional analysis showed that those men with sarcopenia were more likely to have severe ED than those without sarcopenia. Although the association between sarcopenia and severe ED 1 year after the study began did not reach statistical significance and decreased muscle mass and slow gait speed were independently associated with severe ED.
While the frequency of sexual activity decreases with aging, ED is the most common sexual problem in men [1,30]. Only a few studies examined the characteristics of older adults with ED. Those studies used a sexual activity questionnaire or a 15-question version of IIEF to measure ED in mainly urban area dwelling men and reported the prevalence of severe ED ranging from 15.0% to 49.4% [31-33], and which was lower than that in our study. The use of different ED questionnaires or the differences in health status of the study populations may explain the difference in the prevalence of severe ED.
The physiology of penile erection involves relaxation of the penile smooth muscle, enlarged sinusoids, and substantial venous plexus compression. Any situation that can interrupt such mechanisms can cause ED. Impaired parasympathetic outflow or increased sympathetic outflow can inhibit relaxation forces. In addition to patient age, diabetes mellitus, dyslipidemia, metabolic syndrome, atherosclerosis, and smoking can directly reduce the activity of nitric oxide synthase and induce apoptosis of endothelial and smooth muscle cells. And although the mechanism has not yet been fully elucidated, low androgen hormone level and patient depression are also known to affect ED [1].
Sarcopenia is caused primarily by age-related changes, such as sex hormones, apoptosis, and mitochondrial dysfunction. Secondarily, endocrine disorder, e.g., corticosteroid, insulin resistance, abnormal thyroid function, growth hormone, and insulin-like growth factor 1, neuro-degenerative disease, inadequate nutrition, and disuse are known to cause sarcopenia [8,25]. These risk factors demonstrate the overlap of sarcopenia and ED [8,25]. In particular, low levels of androgen are associated with decreased anabolism of skeletal muscle and can consequently cause decreased muscle mass and strength or sarcopenia. In addition, supplementation of the androgen hormone has been cautiously suggested in the treatment of sarcopenia [13,14]. In a meta-analysis, androgen replacement showed increases in overall muscle strength [34]. Sharing of these risk factors and the association of androgen hormone may explain the association between sarcopenia and ED. Previously, the association between ED and sarcopenia in men with diabetes has been reported in a study [15], although the results might not be generalizable to general, community-dwelling, older adults who have and do not have diabetes. Therefore, to our knowledge, our study is the first to report that sarcopenia may be a risk factor for severe ED, independently of established risk factors for ED.
Our results have several potential clinical implications. Recently, the association between ED and frailty, which shows the general performance and physiologic reservoir of older adults, has been suggested/reported [19]. Among sarcopenic older men, unidentified ED patients can be treated to improve their quality of life, and it can be a sentinel check-point to reveal unrecognized frailty and cardiovascular risk factors. In addition, a person with decreased muscle mass and slow gait speed might be able to receive education regarding the future severe ED risk and pre-emptively intervene in order to avoid severe ED in the future.
There are strengths and limitations to our study. Because ASPRA has a high participation rate of eligible individuals, selection bias due to non-participation is unlikely [16]. We administered standardized assessments, including a IIEF-5 questionnaire, comprehensive geriatric assessment, and bioelectrical impedance analysis [18,35], with high completion rates. Among 519 participants at the baseline, 407 men participated in the 1-year follow-up and among the 247 men without severe ED at baseline, 197 were reassessed for ED 1 year later. However, the baseline characteristics between those with IIEF-5 data (407 men) and without (112 men) at 1 year were similar (Supplementary Table 1). Because this study was a population-based study targeted to the community-dwelling, older adults, we provided the clinical evidence to explain the relationship between sarcopenia and erectile dysfunction, but could not show the laboratory findings regarding cellular changes or hormonal levels that further support our report. Subsequent studies are likely to be required and to be designed considering the linking mechanism between sarcopenia and erectile dysfunction.
Our study was underpowered to detect a clinically meaningful increase in the risk of severe ED over 1 year, and which resulted in a wide 95% CI. Nonetheless, two of the three components of sarcopenia, i.e., decreased muscle strength and slow gait speed, were associated with the incidence of severe ED at 1 year, and which suggests sarcopenia as a risk factor for future severe ED. Additional follow-up data from the ASPRA cohort will allow more precise estimation of the association. Lastly, our results from older Korean men who live in rural communities may not generalize to older men who live in urban areas or other countries. Our results should be interpreted with caution until further validation in other populations.
In conclusion, sarcopenia was associated with severe ED, and components of sarcopenia-slow gait speed and decreased muscle mass were independently associated with the incidence of severe ED at 1 year in community-dwelling, older men. Further research is warranted to examine whether an intervention targeting these components can prevent severe ED.
KEY MESSAGE
1. The prevalence of severe erectile dysfunction was high among older Korean men.
2. Sarcopenia was significantly associated with severe erectile dysfunction at baseline.
3. Two sarcopenia components, i.e., decreased muscle mass and slow gait speed, were associated with the incidence of severe erectile dysfunction at 1 year.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





