


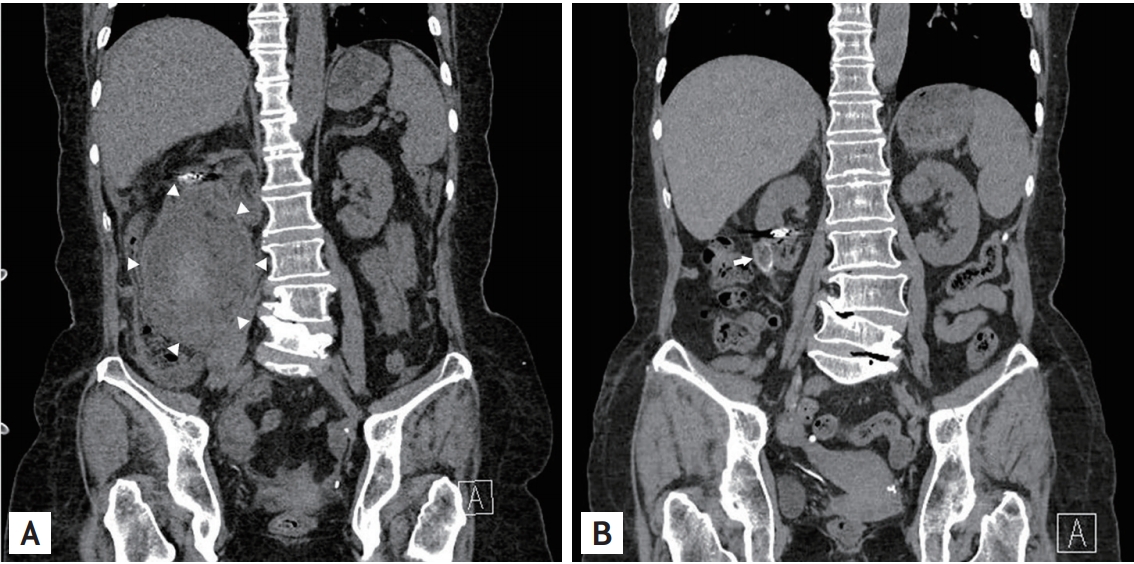
A 61-year-old woman presented at the emergency department with sudden onset abdominal pain. She had a history of hypertension and angiomyolipoma (AML) for 18 years. On physical examination, tenderness in the right upper quadrant was observed. Her blood pressure was 89/54 mmHg and hemoglobin level declined to 7.7 mg/dL from 10.0 mg/dL. We performed abdominopelvic computed tomography (CT) to evaluate the cause of epigastric pain and anemia. In the coronal view on CT, rupture of a giant AML containing hematoma in the lower pole of the right kidney was observed (Fig. 1A). Emergency angiography was performed, and the branch of the right renal artery feeding AML was embolized. After that, the patientŌĆÖs vital signs and hemoglobin level were stabilized, and she recovered uneventfully. Approximately 3 years after discharge, we performed a follow-up abdominopelvic CT, which revealed near complete disappearance of the prior ruptured AML (Fig. 1B).
Wunderlich syndrome is characterized by spontaneous, non-traumatic retroperitoneal bleeding, and the most frequent cause for this syndrome is AML. AML is known as the most common benign tumor of the kidney, and AMLs of large sizes of > 4 cm are known to be associated with a high risk of bleeding. In the case of life-threatening bleeding from AML, selective angioembolization can provide safe and minimally invasive treatment. Surgical resection, especially if malignancy is suspected, can remove the tumor and prevent repeated bleeding. In the present case, we followed up our patient for whom angioembolization for the ruptured AML was performed and were able to obtain serial CT images. This case shows a serial image of regression of AML several years after angioembolization of the rupture AML.
This study was approved by Institutional Review Board (CNUH-EXP-2020-033) and written informed consent was obtained from the patient.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





