


INTRODUCTION
Aristolochic acid (AA)-containing compounds gained notoriety after the emergence of interstitial nephritis in European women who took these compounds to achieve weight loss [1]. The first case of aristolochic acid nephropathy (AAN) was reported in Belgium, and several cases of irreversible renal toxicity after intake of AA-containing compounds have since been reported [1-3].
The presence of AA in an herbal medicine (HM) is important for the diagnosis of AAN in patients with HM-induced renal dysfunction [4]. However, it has not been confirmed that the nephrotoxic potential of AA-containing HM is similar to the nephrotoxic potential of AA. Furthermore, it is unknown if the presence of AA in HM is a major causative factor of renal injury. Therefore, the goal of our study was to evaluate the nephrotoxic potential of HM containing AA in an experimental model in mice [5].
Characteristics of HM used in experiment
We obtained HM from a 33-year-old woman who was prescribed HM for postpartum edema control for one and half months at oriental private clinic. Five months later, routine health examination showed normal renal function and mild proteinuria. Four months later, she visited emergency room due to flank pain, fever and poor oral intake. Laboratory findings revealed renal failure (blood urea nitrogen 68.4 mg/dL, serum creatinine 8.98 mg/dL), anemia (hemoglobin 8.0 g/dL) and metabolic acidosis (pH 7.306, bicarbonate 15.4 mEq/L on arterial blood gas analysis). We started hemodialysis due to uremic symptoms and performed renal biopsy. Pathologic finding was chronic tubulointerstitial nephritis. Thus, we suspected Chinese herb nephropathy, and confirmed AAN by the presence of AA (21.75 mg/kg) in HM using high-performance liquid chromatography.
Experimental animals and AAN model design
The Animal Care and Use Committee of the Catholic University of Korea approved the experimental protocol (CUMS-2017-0218-01). All procedures performed in this study followed the appropriate ethical guidelines for animal studies. Six-week-old C57BL/6 male mice (Orient Bio, Seongnam, Korea), weighing 21 to 23 g, were housed in individual cages at a constant temperature and under a controlled light cycle (12 hours light/12 hours dark). The mice were fed a normal diet with sterilized tap water.
After all mice were acclimatized for 1 week, weightmatched mice were randomized to six groups (n = 8/ group): three groups were used for the short-term study and three groups were used for the long-term study. In the short-term study, HM was made to final concentrations of AA (5 mg/kg) and intraperitoneally injected to the mice once per day for 5 days. For the long-term study, we calculated the patientŌĆÖs daily intake of AA (0.073 mg/kg twice a day) in HM (200 mL/ day/60 kg, twice a day; AA content, 4.35 mg/200 mL), and treated HM or AA via oral gavage, twice per day for 30 days. AA (Sigma-Aldrich, St. Louis, MO, USA) was diluted in phosphate-buffered saline (PBS) and sterilized tap water was given to the VH group. After the short-term or long-term treatment, the animals were anesthetized, and blood samples and tissue specimens were obtained for further analysis.
Measurement of renal function
Blood urea nitrogen (BUN) and serum creatinine (SCr) were measured by using a quantitative enzyme colorimetric method (Stanbio Laboratory, Boerne, TX, USA) in accordance with the manufacturerŌĆÖs instructions.
Evaluation of renal histology
For conventional microscopy of the animals in the short-term study, fixed kidney samples embedded in wax were cut into 5 ┬Ąm slices and stained with hematoxylin and eosin reagents. A complete section of the kidney was screened at a magnification of ├Ś400, and findings for the cortex were semi-quantitatively scored by three independent observers. We assessed renal tubular necrosis by measuring the randomly selected hematoxylin and eosin (H&E) stained sections, and presented its severity as scores based on the percentage of tubules affected (0: < 10%; 1: 10% to 25%; 2: 25% to 50%; 3: 50% to 75%; 4: > 75%) [6]. For the analysis of the mice in the long-term study, kidney tissue sections were stained with periodic acid-Schiff reagent. The tubular dilatation was estimated in a minimum of 20 fields per section by counting the percentage of dilated area per field at a magnification of ├Ś400 using the polygon program (TDI Scope Eye version 3.6 for windows, Olympus, Seoul, Korea). Histopathologic analysis was performed in randomly selected fields of sections by a pathologist blinded to the identity of the treatment groups.
Immunohistochemistry analyses and TUNEL staining
Immunohistochemistry was performed to identify markers of tubular injury (neutrophil gelatinase-associated lipocalin [NGAL]), oxidative stress (8-hydroxy-2ŌĆÖ-deoxyguanosine [8-OHDG]) and apoptosis (active caspase 3) using previously described methods [7]. Primary antibodies for immunohistochemistry are as follows: NGAL antibody (Millipore, Bellerica, MA, USA) 8-OHDG (JaICA, Shizuoka, Japan), manganese-dependent superoxide dismutase (MnSOD, Abcam, Cambridge, MA, USA) and active caspase3 (Millipore, Bellerica, MA, USA). We counted the positive cells per field in 15 randomly selected areas per animal in all groups.
Dewaxed sections were incubated in retrieval solution (pH 6.0), methanolic H2O2, and 0.5% Triton X-100, and then washed in PBS. Nonspecific binding sites were blocked by incubation in 10% normal donkey serum (Jackson ImmunoResearch, West Grove, PA, USA). The sections were incubated overnight at 4Ōäā with primary antibodies and then with peroxidase-conjugated secondary antibodies (Molecular Probes, Carlsbad, CA, USA; Jackson ImmunoResearch) for 2hours at room temperature. Peroxidase activity was detected by using 3,3ŌĆÖ-diaminobenzidine (Vector Laboratories, Burlingame, CA, USA) as a chromogen. Quantitative analysis was achieved through the calculation of the percentage of positively stained area with the same intensity by using histogram equalization (TDI Scope Eye). Apoptotic cells in tissue sections were detected by the terminal deoxynucleotidyl transferase dUTP nick end labelling (TUNEL) method and staining with the in situ Apoptosis Detection Kit (Millipore, Billerica, MA, USA). For each treatment condition, TUNEL-positive cells were counted in 15 randomly selected, non-overlapping areas per animal.
Immunoblotting analysis
Whole cells were lysed in PRO-PREP protein-extraction solution (Intron Biotechnology, Seongnam, Korea) in accordance with the manufacturerŌĆÖs instructions. Equal amounts of protein were subjected to immunoblotting analysis; after incubation with the appropriate primary and secondary antibodies, signals were detected by using an enhanced chemiluminescence system (ATTO Corp., Tokyo, Japan). Quantification of the relative band densities was performed; the intensity of the control group was set to 100% and band densities were normalized to the density of ╬▓-actin bands from the same gel (Quantity One version 4.4.0, Bio-Rad, Hercules, CA, USA).
Electron microscopy
Renal cortex tissues were fixed in 2.5% glutaraldehyde in 0.1M phosphate buffer, were post-fixed with 1% OSO4 and embedded in Epon 812. Ultrathin sections were cut, stained with uranyl acetate/lead citrate, and photographed by using a JEM-1200EX transmission electron microscope (JEOL Ltd., Tokyo, Japan). Sections were scanned randomly at 20 different spots per sample at ├Ś 5,000 magnification. The number of mitochondria was measured in 15 random proximal tubular cells by using imaging software (TDI Scope Eye).
Statistical analysis
The data are expressed as the mean ┬▒ standard error (SE) of at least three independent experiments. Multiple comparisons between groups were performed by oneway analysis of variance with BonferroniŌĆÖs post hoc test computed by using SPSS software version 19.0 (IBM Co., Armonk, NY, USA). Results with p values of < 0.05 were considered statistically significant.
RESULTS
Renal function of AA- and HM-treated mice
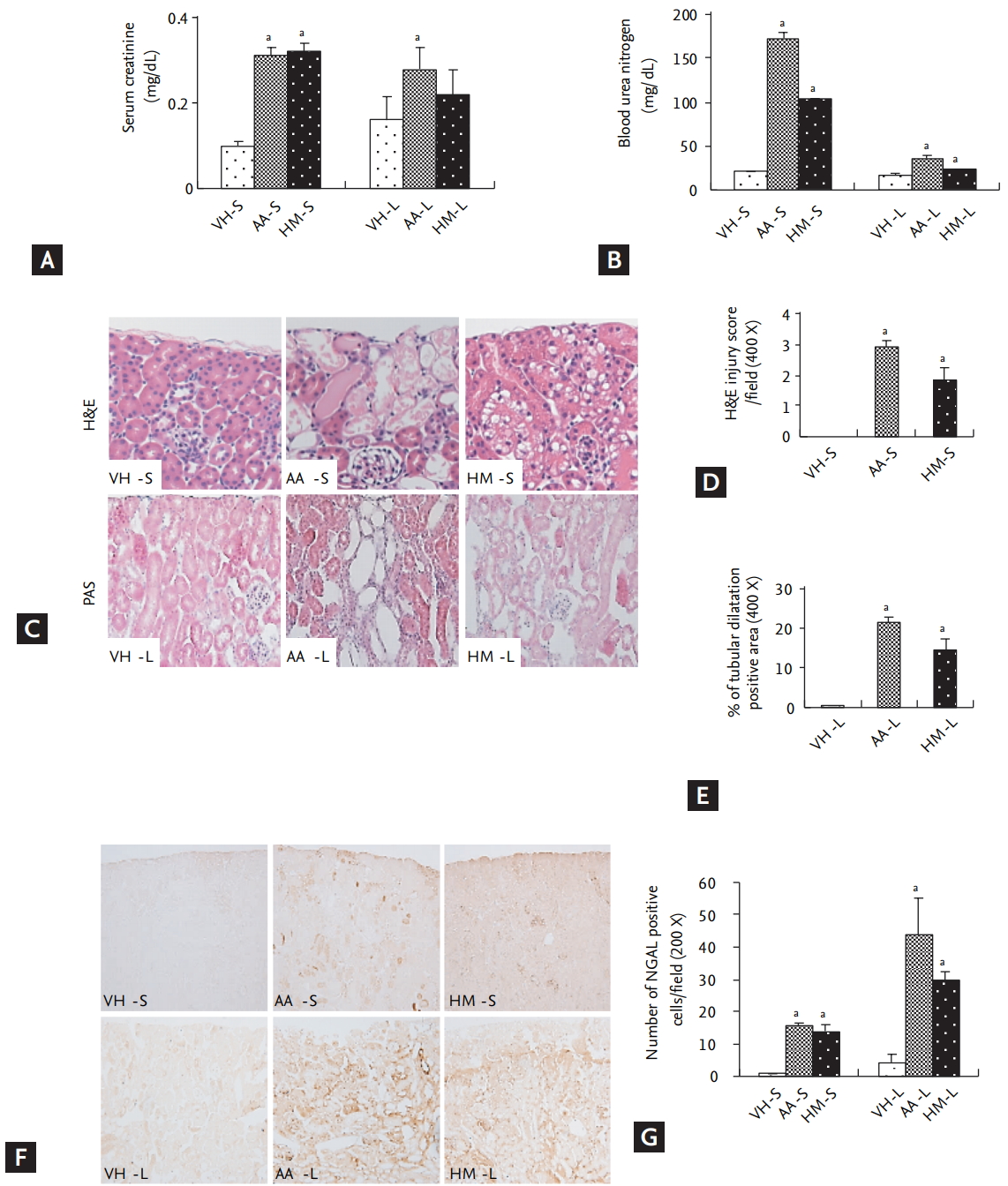
The renal function of each experimental group is shown in Fig. 1A and 1B. In the short-term study, SCr and BUN were markedly increased in the AA (SCr, 0.31 ┬▒ 0.02 mg/ dL; BUN: 173 ┬▒ 7 mg/dL) and HM (SCr, 0.32 ┬▒ 0.02 mg/ dL; BUN, 104 ┬▒ 0.1 mg/dL) groups compared with the VH group (SCr, 0.10 ┬▒ 0.01 mg/dL; BUN, 21 ┬▒ 0.2 mg/dL) group. In the long-term study, SCr (AA, 0.28 ┬▒ 0.05 mg/dL vs. VH, 0.16 ┬▒ 0.06 mg/dL, p < 0.05) and BUN (AA, 36 ┬▒ 3.4 mg/dL vs. VH, 17 ┬▒ 3 mg/dL, p < 0.05) were significantly higher in the AA group than the VH group. Whereas SCr did not increase in the HM group and only a mild increase of BUN was observed (23 ┬▒ 1 mg/dL, p < 0.05 vs. the VH group).
Histopathology of the kidneys of AA- or HM-treated mice
As shown in Fig. 1C and 1D, the short-term study revealed a similar severity of renal tubular necrosis in the HM and AA groups (2.3 ┬▒ 0.3 vs. 3.2 ┬▒ 0.3, p > 0.05). The long-term study also indicated a similar extent of tissue injury in the HM and AA groups (1.9 ┬▒ 0.2 vs. 3.3 ┬▒ 0.4, p > 0.05) (Fig. 1E). The NGAL expression in HM (14 ┬▒ 2 per field) and AA (15.5 ┬▒ 1 per field) groups were increased compared to the VH (0.8 ┬▒ 0.02 per field) group (p < 0.05) in the short-term study. Also in the long-term study, the NGAL expression in HM (29.5 ┬▒ 2.9 per field) and AA (43.8 ┬▒ 11.3 per field) groups were increased compared to the VH (4.3 ┬▒ 2.5 per field) group (p < 0.05). However, there was no significant difference between the AA and HM groups in short- and long-term studies (Fig. 1F and 1G).
Oxidative stress in the kidneys of AA- or HM-treated mice
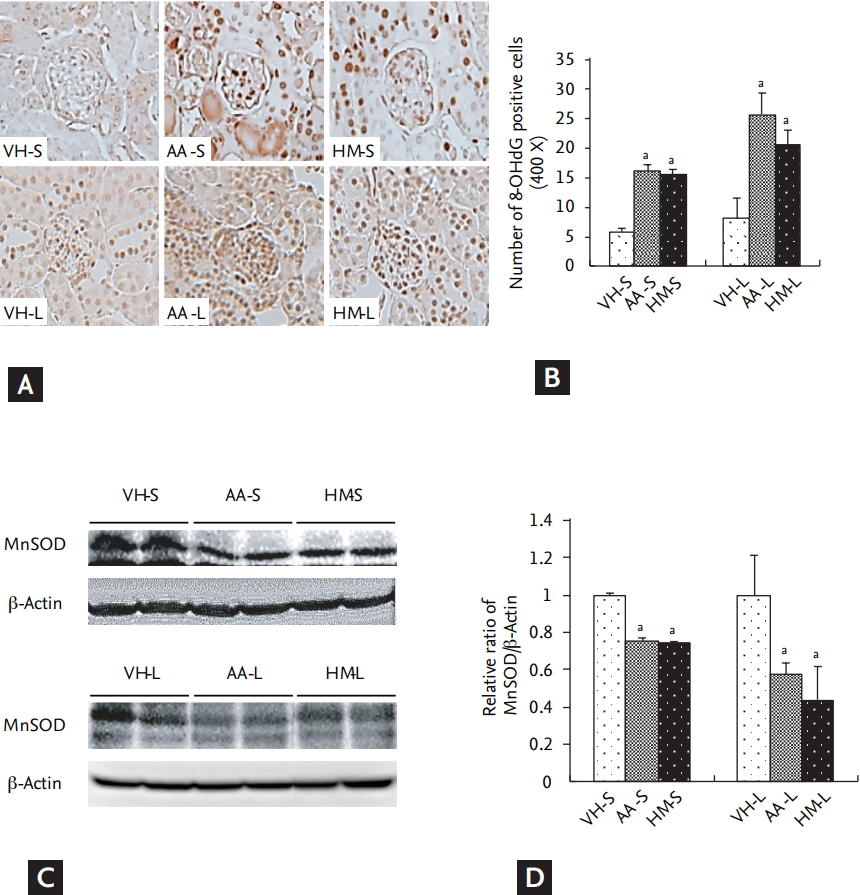
To compare the oxidative stress induced by HM and AA treatments, we measured 8-OHdG and MnSOD in the treatment groups. In the short-term study, the expression of 8-OHdG was significantly higher in the HM (15.6 ┬▒ 0.8 per field) and AA (16.2 ┬▒ 1 per field) groups than in the VH (5.8 ┬▒ 0.6 per field)-treated group (p < 0.05), but there was no significant difference between the HM and AA groups. Similar findings were observed in the longterm study (Fig. 2A and 2B).
In short-term study, the relative expression of MnSOD was lower in the HM (0.74 ┬▒ 0.01 folds) and AA (0.75 ┬▒ 0.02 folds) groups than the VH group (p < 0.05), but there was no significant difference between the HM and AA groups. Similar findings were observed in the longterm study (Fig. 2C and 2D).
Mitochondrial injury in the kidneys of AA- or HM-treated mice
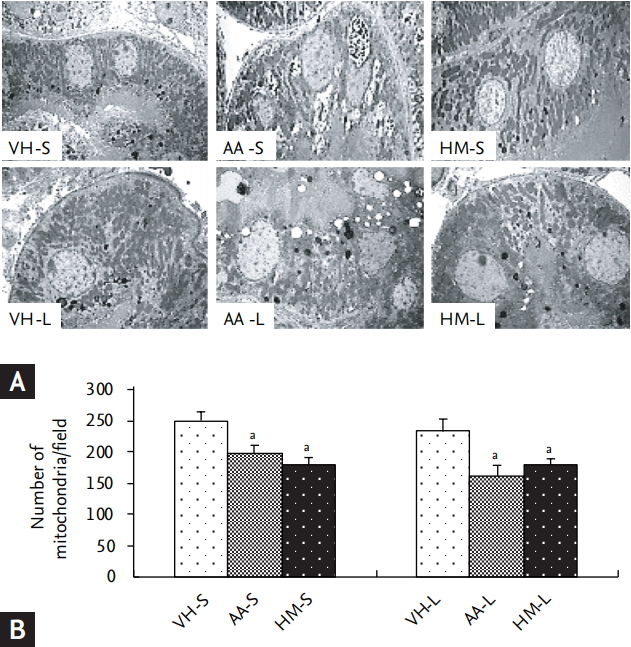
In the AA- and HM-treated groups, proximal tubular cells exhibited severe injury, with altered brush border, cell detachment, and extensive cytoplasmic vacuolization compared with VH treatment (Fig. 3A). The number of mitochondria was lower in both the AA and HM group than the VH group, but there was no significant difference between the AA and HM groups in the short-term (197 ┬▒ 14 per field vs. 180 ┬▒ 12 per field) and long-term (162 ┬▒ 17 per field vs. 180 ┬▒ 10 per field) studies (Fig. 3B).
Apoptosis in the kidney of AA- and HM-treated mice
The number of TUNEL-positive cells (Fig. 4A and 4B) in the HM and AA groups were markedly higher than the VH group in the short-term (6.8 ┬▒ 0.4 per field in the AA group and 6.0 ┬▒ 0.3 per field in the HM group vs. 1.2 ┬▒ 0.8 per field in the VH group, p < 0.05 vs. VH groups) and long-terms studies (13.6 ┬▒ 3.5 per field in the AA group and 11.4 ┬▒ 3.8 per field in the HM group vs. 0.7 ┬▒ 1.2 per field in the VH group, p < 0.05 vs. VH groups). However, there was no significant difference between the AA and HM groups in both studies. Fig. 4C and 4D shows the immunoblotting for active caspase-3. The active caspase-3 expression in the HM or AA groups were increased compared to the VH group in both short-term (2.8 ┬▒ 0.6 folds in the AA group and 3.3 ┬▒ 0.4 folds in the HM group, p < 0.05 vs. VH group) and long-term studies (4.2 ┬▒ 0.2 folds in the AA group and 1.8 ┬▒ 0.1 folds in the HM group, p < 0.05 vs. VH group). Between HM and AA groups, there was no difference between two groups in short-term study, but HM group was lower than the AA group in long-term study.
DISCUSSION
In our study, we aimed to determine whether the presence of AA in a HM was a major factor in renal injury. To determine this, we performed an experimental study in mice to compare the nephrotoxic potential of HM containing AA and the AA compound administered alone. The results of our study clearly demonstrated that HM containing AA caused similar nephrotoxicity to that of AA, and that AA concentration in HM was the major determinant of the severity of renal injury.
The purpose of short-term study was to test the acute toxic effects of HM. Based on AA dose in reported experimental model of acute AAN [6,8], we treated HM or AA (5 mg/kg) intraperitoneally in mice for 5 days. As expected, HM administration resulted in the typical features of acute kidney injury (AKI), including marked deterioration of renal function and acute tubular necrosis; moreover, the severity occurred at a similar level to that observed after administration of AA. In addition, the expression of NGAL, a biomarker of AKI, was increased in HM-treated mice and was comparable to the expression in AA-treated mice. This finding was consistent with previous reports that a high-dose AA caused AKI and that the major pathological finding was acute tubular necrosis [8-10].
We designed the long-term study to evaluate the chronic toxicity of HM based on the patientŌĆÖs prescription. We calculated the daily AA exposure from the prescribed dose and administered the same treatment duration as described in the patientŌĆÖs medical history. The long-term study revealed mild renal dysfunction, tubular atrophy and dilatation, and increased NGAL expression in both the HM and AA groups, with no significant difference between two groups. These findings suggested that long-term exposure to low-dose AA resulted in CKD. Collectively, AAN can present as AKI or CKD according to the concentration of AA or duration treatment of HM; this may be supported by a clinical report indicating that AAN results in a wide range of renal dysfunction based on the exposed dose and treatment duration [4].
In long-term study, we could not develop renal fibrosis, common histologic finding of AAN [11], and it seems to be related to the treatment duration. We stopped experiment earlier (at day 30) than initial schedule (6 weeks) because of poor condition of experimental animals. Thus, we could observe only tubular injury (atrophy and dilatation). In this point, we expect that renal fibrosis can be developed with longer treatment. Another consideration in the long-term study is the discrepancy between pathology and renal function in the HM group. In spite of pathologic change (increased tubular atrophy and dilatation, and NGAL expression), renal function was normal (Scr, 0.22 mg/dL). The reason for normal renal function in the HM group is unclear, but we speculate that antioxidant component in HM may reduce the nephrotoxic potential of AA [12].
The pathophysiological mechanisms through which AA induces renal injury are still largely unknown, but oxidative stress is reported as a common mechanism of AAN [13,14]. Therefore, we compared the oxidative stress and the resulting cell death in HM- and AA-treated mice. In this study, we found that HM exerted a similar degree of oxidative stress (8-OHdG and MnSOD) and apoptotic cell death (TUNEL-positive cells and activated caspase-3) compared with AA; similarly, mitochondrial damage induced by HM was also similar to that induced by the administration of AA alone in both the short-term and long-term studies. These findings confirmed that, in terms of oxidative stress, HM induces a similar degree of injury to AA, suggesting that oxidative stress induced by HM resulted in mitochondrial damage, apoptosis, and caspase-3 activation, which may lead to progressive tubular atrophy and interstitial fibrosis [11,14].
The results in our study illustrate the comparable nephrotoxicity of HM and AA; however, there are some limitations. First, there might be a selection bias as the HM obtained from a single source. Second, we did not consider species-specific toxicity of AA [15]. Therefore, the results of our study in mice should be interpreted with caution in humans. Third, the AA dose (0.073 mg/kg, twice a day) for long-term study was lower than dose (4 or 5 mg/kg) for experimental AAN. But, our study suggests that long-term exposure to low dose AA can develop AAN.
In conclusion, HM containing AA had a similar nephrotoxic potential to that of AA.
KEY MESSAGE
1. The nephrotoxic potential of herbal medicine containing aristolochic acid is similar to that of aristolochic acid itself.
2. The concentration of aristolochic acid in herbal medicine is the major determinant of the severity of renal injury.
3. Long-term exposure to low dose aristolochic acid can develop aristolochic acid nephropathy.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





