


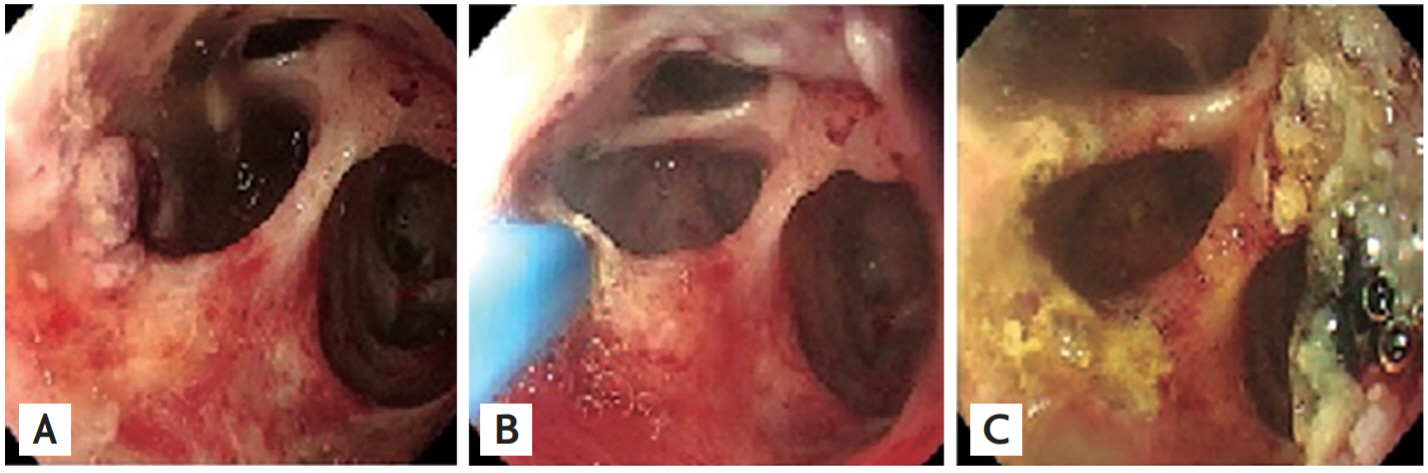
An 81-year-old man was admitted for abdominal pain, fever, and jaundice. Contrast enhanced computed tomography (CT) showed marked dilation of both intra- and extrahepatic ducts (Fig. 1A). Endoscopic retrograde cholangiopancreatogram suggested a diagnosis of intraductal papillary mucinous neoplasm from the bile duct (IPMN-B) due to abundant mucin that exuded from papilla and common bile duct dilatation with an amorphous filling defect (Fig. 1B). Direct per-oral cholangioscopy using a conventional upper endoscope (GIFQ260J, Olympus, Tokyo, Japan) was planned. Cholangioscopy revealed multiple exophytic papillary protrusions consistent with IPMN-B involving the left intrahepatic ducts and hilar portion, but an uninvolved right intrahepatic duct (Fig. 2A). Cholangioscopy-directed biopsy was performed and papillary epithelial neoplasm with intermediate grade of dysplasia was diagnosed histologically. Argon plasma coagulation (APC) was performed at papillary lesions to reduce tumor burden with the goal of reducing mucin production. The lesions were successfully ablated by three sessions of APC performed over 8 days at 40 W, pulsed, effect 1, and 1.0/min flow (Fig. 2B and 2C). One month later, CT showed marked improvements of intra-andextrahepatic duct dilations, and at 8 months after treatment the patient was still healthy without abdominal pain or recurrent cholangitis.
This case raises two aspects of clinical interest. First, no previous case report has been issued of a successfully diagnosed IPMN-B patient treated by direct per-oral cholangioscopy using a conventional upper endoscope. Second, no clear guideline has been issued regarding the palliative treatment of IPMN-B, and thus, we hope our experience may aid considerations of palliative treatment for similar patients.
In patients with IPMN-B, recurrent cholangitis is the most problematic situation, despite endoscopic biliary drainage. In our patient, APC reduced mucin production and effectively ablated almost all tumor tissues; the ablation of all tumor tissues was impossible because scope movement was limited in the bile duct.
Written informed consents were obtained.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





