


To the Editor,
Acute myocarditis associated with a normal left ventricular (LV) ejection fraction is challenging to diagnose. Echocardiography is the initial imaging modality used, but diagnostic accuracy is limited, especially in patients with chest pain in whom LV function and size are almost always normal [1]. The current reference standard for noninvasive diagnosis of myocarditis is cardiac magnetic resonance (CMR) imaging [2]. Here we describe a case of a 19-year-old man who presented with severe chest pain that mimicked acute coronary syndrome but was subsequently diagnosed with acute regional myocarditis by two-dimensional (2D) speckle echocardiography. The patient was successfully treated medically for myocarditis.
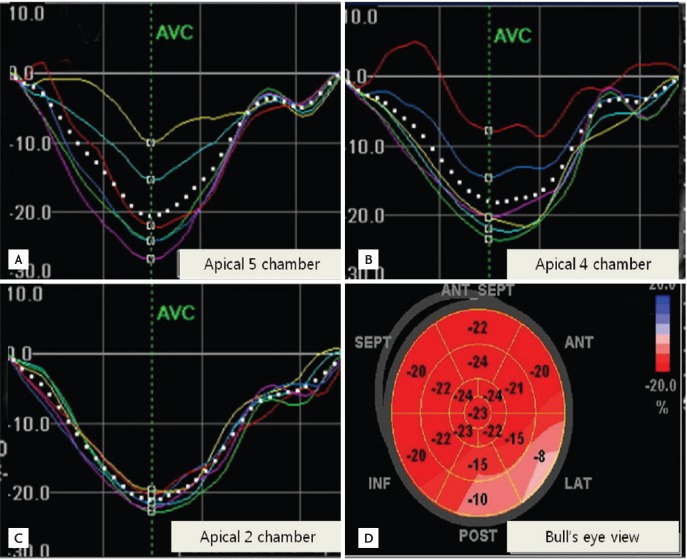
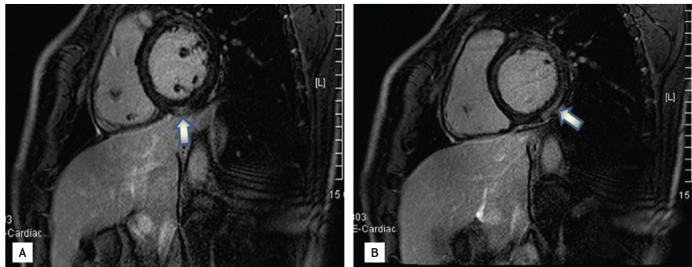
A 19-year-old male with no cardiovascular risk factors was admitted due to chest discomfort and fever. On admission, blood pressure, heart rate and body temperature were 140/65 mmHg, 92 beats per minute, and 38Ōäā, respectively. Initial electrocardiography showed upwardly concave ST elevations in II, III, and aVF leads, with no reciprocal change in the anterior chest lead. Laboratory tests revealed elevated serum C-reactive protein (CRP) and cardiac biomarker (CRP, 1.5 mg/L; creatine kinase [CK], 616 IU/L; CK-MB, 53.0 IU/L; and troponin-I, 4.81 ng/mL). A 2D-echocardiogram showed normal regional wall motion with preserved LV systolic and diastolic function, but automated function imaging, which was assessed by a 2D speckle-tracking imaging (STI), showed a decreased peak in the systolic longitudinal strain of the basal inferior and lateral walls (Fig. 1D, Bull's eye view) and the circumferential strain also decreased in the basal inferior and lateral walls (Fig. 2). Strain curves showed that abnormal longitudinal systolic shortening was detected by strain echocardiography in the lateral and posterior wall, where there were abnormalities indicating longitudinal strain such as a reduced systolic shortening and a postsystolic peak (Fig. 1A, yellow line; Fig. 1B, red line); however, longitudinal systolic shortening in the anterior, inferior and septal walls was normal (Fig. 1C). This pattern was also observed in the circumferential strain curve (Fig. 2). Elevated cardiac biomarkers and decreased regional peak systolic strain usually suggest regional coronary ischemia. However, in this patient, ischemic disease was extremely unlikely due to his young age, lack of family history of coronary artery disease, and lack of regional wall motion abnormalities on the conventional 2D echocardiogram, despite a decreased regional peak longitudinal strain. Therefore, conservative treatment was initiated, including pain medications and diuretics, rather than invasive procedures such as a coronary angiography or myocardial biopsy. To confirm the diagnosis and to examine the change in the myocardium, CMR imaging was performed on the day following admission. Gadolinium-enhanced CMR on the fifth day of admission demonstrated subepicardial delayed hyperenhancement at the basal inferior, lateral wall and the mid lateral wall on short axis, 10 minutes after the enhancement of the image in accordance with myocarditis (Fig. 3). Surprisingly, abnormalities in automated functional imaging and strain curve analysis correlate closely with findings on CMR imaging. Antigen tests for cosackie and influenza viruses were positive. With the suspicion of acute viral myocarditis associated with influenza, we prescribed tamiflu (Genentech, Basel, Switzerland) for 5 days. The patient's clinical signs resolved along with the normalization of the ST segment changes and the serum CK level.
Acute myocarditis has myriad presentations, and often mimics acute coronary syndrome at initial presentation. CMR imaging and myocardial biopsy at the initial acute presentation is not feasible for a differential diagnosis and cannot confirm myocarditis. However, conventional 2D echocardiography, plus strain imaging were crucial in this case to determine the best course of treatment. This case demonstrated that decreased myocardial strain as assessed by 2D speckle echocardiography and different strain curve pattern such as reduction in systolic shortening and postsystolic peak may lead clinicians to the accurate diagnosis of acute myocarditis in patients with chest pain and elevated cardiac biomarkers, but normal wall motion, mimicking acute coronary syndrome.
Although the diagnosis of myocarditis has traditionally required a histologic diagnosis, according to the classic Dallas criteria, new diagnostic strategies such as CMR can strongly indicate and diagnose myocarditis. CMR imaging can characterize tissue according to water content and changes in contrast kinetics, which allows visualization of the entire myocardium. Thus, it is well suited to detect patchy myocarditic lesions [3]. Recently, CMR imaging has become the noninvasive diagnostic tool of choice to diagnose myocarditis, and is recommended in patients whose symptoms suggest this condition [2]. However, CMR does have some disadvantages, notably its high cost and the time needed to perform it; therefore, it is not feasible in an acute emergency setting.
Conventional 2D echocardiography has traditionally played a limited role in the diagnostic armamentarium for acute myocarditis due to the lack of specific distinguishing features and/or apparently normal examinations encountered in less severe forms of myocarditis [1]. Nevertheless, segmental and global wall motion abnormalities do occur, and patterns of hypertrophic, dilated, and restrictive cardiomyopathy have been reported in histologically proven myocarditis [1]. The advent of novel echocardiographic modalities, such as strain echocardiography, has dramatically expanded the scope of echocardiography, which provides an accurate bedside assessment of regional contractility and can identify longitudinal myocardial dysfunction derived from edema in acute myocarditis [4,5].
Particularly for myocardial damage of only the epicardial layer of the ventricular wall during acute myocarditis, Doppler echocardiography can identify longitudinal segmental myocardial dysfunction derived from edema [5]. These newer techniques are more efficacious than conventional echocardiography in the diagnosis of myocarditis.
Interestingly, decreased myocardial longitudinal strain and circumferential strain assessed by the 2D speckle tracking technique, in the absence of wall motion abnormalities, may represent a useful additional diagnostic finding in acute regional myocarditis, while longitudinal segmental myocardial dysfunction derived from edema also supports the diagnosis. This methodological improvement allowed us to evaluate myocardial damage using CMR rather than subjecting the patient to invasive methods such as coronary angiography.
In conclusion, in young patients with chest pain who have elevated cardiac biomarkers and dynamic EKG changes but who do not fit the signalment for coronary disease, 2D STI analysis, including longitudinal and circumferential strain, can help physicians to diagnose acute myocarditis and to devise an appropriate treatment plan.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





