


INTRODUCTION
Acute febrile neutrophilic dermatosis is a clinical condition, which is histologically characterized by sterile infiltration of neutrophils throughout the dermis1). This condition may affect various internal organs, such as the lungs, digestive tracts, joints, eye, bone or central nervous system; whereas muscular involvement is extremely rare. It is known in association with various chronic conditions, such as inflammatory bowel disease, as well as with malignancies, particularly acute myeloid leukemia2). Here, we describe a patient whose only clinical manifestations were fever and myositis, without any cutaneous involvement, as the first manifestation of acute myeloid leukemia. With a high index of suspicion for such a condition, the unnecessary use of antibiotics and delayed initiation of chemotherapy would be prevented.
CASE REPORT
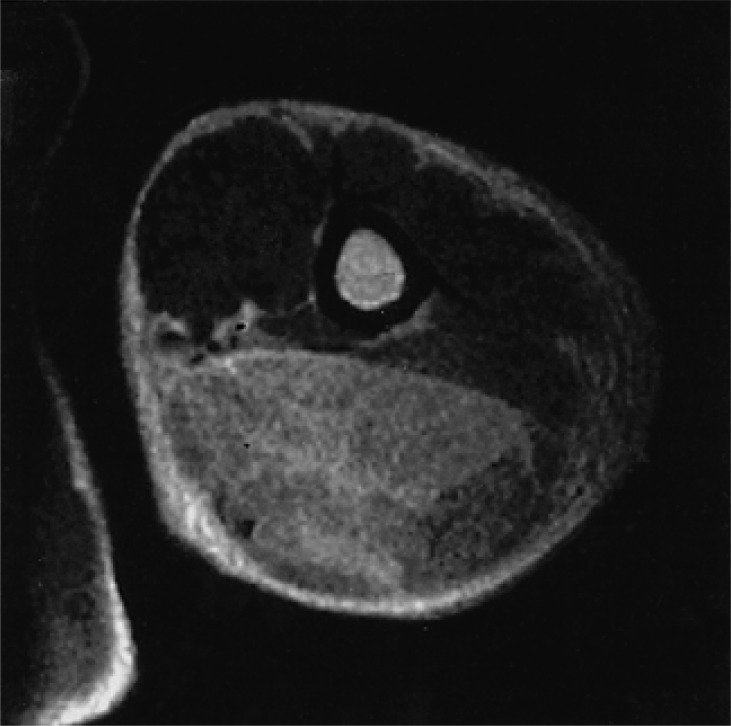
A previously healthy 35-year-old male complained of intermittent fever and myalgia of 1-month duration. On admission, he was febrile (39.2Ōäā), with painful tenderness of the edematous upper arm; however, the overlying skin had no grossly abnormality. Ultrasonography showed a diffusely increased echogenicity in his thickened triceps, brachialis and gluteus muscles. Therefore, a magnetic resonance imaging study was performed (Figure 1).
A confirmatory muscle biopsy was performed on his left triceps and brachialis muscles. These histological specimens showed severe myositis, with predominantly dense infiltration of mature neutrophils, associated disruption of the muscle architecture and tissue necrosis (Figure 2). Microbiological studies and serology for auto-antibodies were negative.
The initial complete blood count revealed an elevated white blood cell count of 20,440/mm3, with a differential count of 7% segmented neutrophils, 22% lymphocytes and 40% blast cells, which were strongly suggestive of leukemia. The serum chemistry studies disclosed an elevated lactate dehydrogenase level of 977 U/L. The patient subsequently underwent a diagnostic bone marrow aspiration and biopsy, which showed replacement of the normal bone marrow with myeloblasts. The flow cytometric findings were positive for CD13, but negative for CD33, CD14 and HLA-DR. Cytogenetic studies showed a normal karyotype (46,XY[20]). PCR of AML1/ETO was negative. On the basis of the flow cytometry and cytogenetic studies, the final diagnosis was confirmed as a M2 subtype of acute myeloid leukemia, with paraneoplastic neutrophilic myositis. Concomitant treatment with corticosteroid and induction chemotherapy was started. The fever, myalgia and swelling of both the upper arms were resolved after 5 days of steroid therapy.
An ultrasonography after 6 weeks of therapy demonstrated resolution of the muscle swelling seen at diagnosis. After the induction chemotherapy, and 2 courses of consolidation, followed by autologous stem cell transplantation, hematological remission was maintained for 15 months. The lack of stem cell sources limited the salvage therapy for the first relapse due to chemotherapy. At present, the patient is on close follow-up in the third hematological relapse. After the initial diagnosis, neither myalgia nor fever reappeared for 36 months.
DISCUSSION
There have been many reports of neutrophilic dermatosis associated with inflammation of the respiratory tract or intestines, and drugs, such as G-CSF, trimethoprim-sulfamethoxazole and all-trans-retinoic acid (ATRA), as well as malignancies3). The association between leukemia and acute febrile neutrophilic dermatosis, also known as Sweet or Sweet-like syndrome, is not a recent observation. There have been numerous clinical and histopathological reports concerning neutrophilic dermatosis in leukemia4).
Extracutaneous involvement, especially articular manifestations, may precede the cutaneous symptoms of neutrophilic dermatosis, but are more often observed during the course of neutrophilic dermatosis. However, muscle involvement is usually considered a more uncommon manifestation of neutrophilic dermatosis. In a series of 136 patients with neutrophilic dermatosis, Moreland et al. reported that fewer than 10% of patients had myalgia5). Although there have been occasional case reports on neutrophilic myositis concurrently observed with dermatosis as the initial manifestation of leukemia, such cases are relatively rare6, 7). There have also been some reports on myositis without cutaneous lesions, which was probably induced by ATRA and aggravated by the use of G-CSF8, 9).
Our case was a clinically uncommon occurrence of acute myeloid leukemia, of which the initial and only manifestation was myositis, without skin involvement. Other muscle disorders (e.g., polymyositis, dermatomyositis or infectious myositis) were excluded, and a diagnosis of neutrophilic myositis could be reasonably made in our patient because of: (1) densely infiltrated mature neutrophils confirmed in the examined specimen (2) the negative findings from the cultures and stains for bacteria and fungi (3) the extensive search for other causes of myositis (i.e., both infectious and connective tissue disorders) that proved negative and (4) the rapid improvements of the fever and arm swelling were observed after the initiation of steroid therapy; whereas, broad-spectrum antibiotic treatment was ineffective. The initiation of chemotherapy for the acute leukemia was delayed for a few days, as time was required to rule out the possibility of infectious causes. Thus, our case indicates the diversity of clinical manifestations included with leukemia.
In conclusion, our case is representative of the rare cases in which acute febrile neutrophilic myositis, without cutaneous involvement, occurred as the initial manifestation, and not during the clinical course, of leukemia. The existence of such cases implies the importance of differential diagnosis of the possible underlying diseases when caring for a patient with the sudden onset of febrile myositis. The most frequent underlying causes of such clinical symptoms are supposed to be any kind of infectious disorder, but hematological disorders, such as leukemia, should not be ruled out as a possibility. Fortunately, our case was diagnosed as paraneoplastic myositis early in the course of his leukemia; the patient had the chance to completely and rapidly recover with the use of corticosteroid therapy.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





