


INTRODUCTION
The coronary angiogram (CAG) remains the gold-standard method for assessing coronary artery disease (CAD). However, the CAG has inherent pitfalls, such as only showing the vessel lumen as an X-ray shadow image, created by the injection of contrast medium, and of often visualizing a "side-view." Thus, the apparent degree of coronary stenosis can be affected by the projection angle due to lesion eccentricity. Additionally, diffuse coronary disease, lesion foreshortening, angulations, calcification, and vessel overlap can be challenges in the angiographic assessment of lesion severity. In some cases, an angiographically normal-looking coronary artery actually shows various degrees of atherosclerotic plaque by intravascular ultrasound (IVUS) [1,2].
IVUS is an invasive imaging technique used to visualize coronary cross-sectional anatomy and is superior to CAG in assessing vessel size, calcium content, and lesion severity [3]. It also provides complementary procedural information in lesions requiring percutaneous coronary intervention (PCI) when determining adequate stent sizing, and confirming optimal stent deployment and apposition without edge tearing in real time. Thus, a growing number of interventional cardiologists attain optimal procedural results with reduced complications when using IVUS in PCI.
Although the routine use of IVUS in daily PCI remains controversial, stent optimization by IVUS during stenting procedures, especially in the era of drug-eluting stents (DESs), may have an important role in improving long-term clinical outcomes such as stent restenosis and stent thrombosis [4]. In this review, we focus on the potential roles of IVUS in stent optimization during PCI and its clinical benefits.
REALITY OF STENTING PROCEDURES IN DAILY PRACTICE
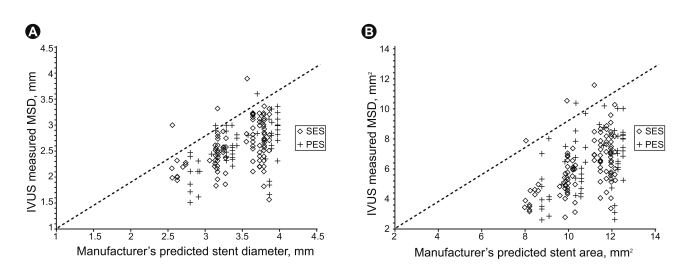
PCI has been the fastest growing method for the treatment of ischemic CAD over the past three decades. Coronary stents have emerged as the predominant form of PCI and are currently used in more than 90% of PCI procedures. Procedural success of PCI is usually determined by visual estimation by the operator, and usually, angiographic success after PCI is defined as the attainment of residual diameter stenosis of less than 30%, which is generally associated with at least a 20% improvement in diameter stenosis and relief of ischemia [5]. However, such subjective estimation of the severity of coronary artery stenosis is thought to be of limited reliability. Previous IVUS studies have demonstrated that visual estimation or quantitative angiographic analyses of vessel dimension for stent deployment appear inaccurate [6-9]. The post-dilatation clinical comparative (POSTIT) trial was designed to assess the achievement of optimal stent deployment by IVUS, according to normal-to-high pressure balloon dilation after bare metal stent implantation. Among 256 patients, only 14% of cases achieved optimal stent deployment with under 12-atmosphere pressure dilation and only 36% even with higher deployment pressures (> 14 atmospheres) [9]. Another IVUS study with an early-generation DES in 200 patients assessed stent expansion depending on the manufacturer's compliance chart as a guideline. In that study, the DES obtained only 75% of predicted minimal stent diameter and 66% of the predicted minimal stent area (MSA) [10] (Fig. 1). Based on these observations, angiographic success cannot always be linked with optimal stent expansion, despite higher pressure balloon inflation during the stenting procedure. In turn, stent optimization using a high-pressure balloon without IVUS guidance also has been associated with an increased risk of arterial perforation, probably secondary to vessel-balloon mismatch [11]. Thus, the operator should consider using IVUS guidance for high-pressure balloon inflation during stent deployment.
Apposition of stent struts to the vessel wall is also an important facet of stent optimization. Adequate stent expansion and adequate stent strut apposition have been reported to be important factors in reducing repeated revascularization due to stent restenosis or stent thrombosis [12,13]. In the DES era, incomplete stent apposition has been regarded as an important local factor in DES failure, probably due to reduced drug delivery to the vessel wall [14-17]. In a recent report, incomplete stent apposition was significantly associated with vessel/stent mismatch rather than stent underexpansion immediately after stent implantation [18]. Thus, adequate stent sizing by IVUS may be clinically important in preventing incomplete stent apposition and in optimizing initial stent deployment.
IMPORTANCE OF STENT OPTIMIZATION
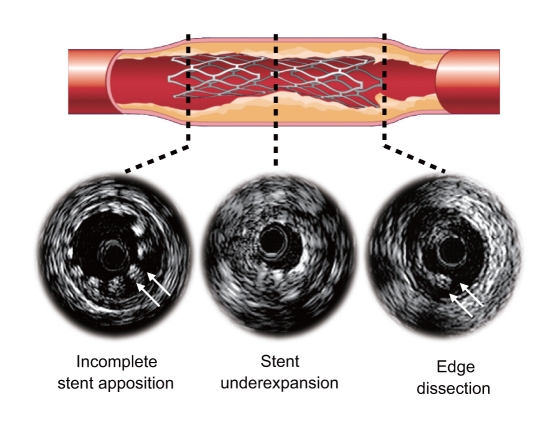
IVUS has been used to detect suboptimal results after apparently angiographically successful stent deployment in both the DES and bare metal stent (BMS) eras (Fig. 2). IVUS predictors that are associated with increased adverse outcomes include smaller MSA, stent underexpansion, stent edge dissection, incomplete stent apposition, and incomplete lesion coverage [19-26]. In the BMS era, a major problem after stent implantation was stent restenosis, and the main mechanism of this phenomenon was a smaller MSA or stent underexpansion [21,26-30]. Several studies in the BMS era showed a beneficial effect of IVUS guidance on post-procedural angiographic results and stent restenosis during long-term follow-up, resulting from a larger MSA with a higher post-dilation balloon pressure [7,19,27,31]. Stent underexpansion, identified by IVUS, can be treated with appropriate post-balloon dilation. IVUS allows more aggressive intervention using a larger diameter balloon with confidence in terms of safety; thus, BMS implantation under IVUS guidance can provide a bigger MSA and more favorable clinical outcomes compared with angiography-guided PCI. DESs have led to a marked reduction in the rate of stent restenosis and the need for repeated revascularization compared with BMSs [32,33]. Because of their efficacy, high-risk lesions and clinical conditions, including bifurcation lesions, long lesions, calcified lesions, left main disease, diabetes, and multivessel disease, are now being treated routinely with DESs [34,35]. Thus, the risk of stent underexpansion, incomplete stent apposition, and incomplete lesion coverage increases and these suboptimal stent deployment conditions have been reported to be potent IVUS predictors of stent restenosis and stent thrombosis [13,17,24], suggesting that stent implantation under IVUS guidance still has a pivotal role even in the DES era. An important aspect of IVUS is determining appropriate reference segments that provide the landing zone for stent deployment. IVUS examination typically reveals a considerable amount of plaque, even in segments of the vessel that appear "normal" on the angiogram, known as "reference vessel" disease. Quantitative IVUS studies have demonstrated that the segment chosen as the "normal" reference site for the calculation of angiographic percent stenosis has an average of 30-50% of its cross-sectional area occupied by plaque [36]. By IVUS, the definition of reference segment is a cross-sectional image adjacent to the lesion that has < 40% plaque burden [37]. A previous study reported the association between clinical outcomes and longitudinal positioning of the stent in 162 consecutive patients with 180 lesions treated with sirolimus-eluting stent (SES) implantation [38]. In that study, stepwise IVUS criteria primarily targeting plaque burden < 50% were shown to be feasible and improved the rates of stent restenosis and target lesion revascularization (TLR) at 8 months follow-up.
HOW TO OPTIMIZE STENT DEPLOYMENT
IVUS is used frequently in PCI, but the use of IVUS cannot be directly related to stent optimization. Definitive guidelines for IVUS-guided stent optimization are not available and it is still performed at the operator's discretion. So, how do we perform stent optimization using IVUS, and what IVUS criteria are acceptable for current practice?
Although many IVUS criteria for stent optimization have been suggested, the basic concepts underlying them can be summarized briefly as minimizing the occurrence of IVUS-related predictors of adverse events after PCI, including stent underexpansion, incomplete stent apposition, edge dissection, and lesion undercoverage.
Stent underexpansion is defined as an area of inadequate stent expansion compared with the adjacent reference segments. However, a consensus definition of "adequate" expansion is still lacking.
In the BMS era, several randomized trials used various IVUS criteria for stent deployment optimization, yielding mixed results. The first large multicenter study, called MUSIC (multicenter ultrasound stenting in coronaries study), sought to define specific criteria for optimal stent deployment and demonstrate the feasibility and safety of IVUS-guided stent optimization [39]. In the MUSIC criteria, "adequate" expansion was defined as > 90% of the average reference cross-sectional area (CSA), or > 100% of a smaller reference CSA with complete apposition and symmetric expansion. Another large multicenter trial was AVID (angiographic versus IVUS direct stent placement); its defined IVUS optimization required complete stent apposition with stent CSA > 90% of the distal reference lumen area [40]. The results of the AVID trial showed a significant benefit of IVUS guidance in vessels 2.5-3.5 mm in size and in saphenous vein graft PCI. The TULIP (thrombotic activity evaluation and effects of ultrasound guidance in long intracoronary stent placement) Study also showed significant angiographic and clinical benefits of IVUS guidance using criteria such as stent CSA > distal reference lumen [41]. In contrast to the results mentioned above, the OPTICUS trial (optimization with IVUS to reduce stent restenosis) using the MUSIC criteria for IVUS guidance did not show a significant difference in 6- or 12-month clinical outcomes [42]. However, in this study, only 56% of stents met all three MUSIC criteria. Many other trials in the BMS era used similar IVUS criteria, and two meta-analyses showed better outcomes of IVUS-guided PCI than angiography-guided PCI, especially in terms of in-stent restenosis and target vessel revascularization (TVR), but not in mortality or myocardial infarction [43,44].
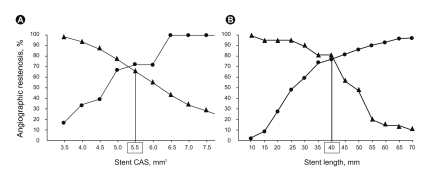
In contrast to the BMS era, for IVUS-guided PCI with DES, few randomized studies showing clinical efficacy, preventing TVR or restenosis, or stent optimization under IVUS guidance have been carried out. In the HOME DES trial, optimal stent deployment was defined as complete apposition of the stent struts, no edge dissection, and adequate stent expansion, defined as either MSA > 5.0 mm2 or > 90% of the distal reference lumen area [45]. In that study, no significant benefit in terms of TVR or clinical events was reported. A similar finding was also noted in the AVIO (angiography versus IVUS optimization) study in which optimal stent expansion was > 70% of the CSA of the chosen balloon [46]. However, attention should be paid to avoid stent underexpansion. Increasing evidence indicates that IVUS-guided PCI may reduce the risk of stent thrombosis (ST) [47]. Stent underexpansion was demonstrated to be one of the major causes of this disastrous complication, although the cause of ST is multifactorial [13,24,48,49]. In a substudy of the SIRIUS trial, adequate patency was defined as a follow-up IVUS MSA > 4.0 mm2. When the adequate post-interventional MSA of SESs was defined as > 5.0 mm2, the positive predictive value of patency was 90%, but the optimal cutoff value of BMS was defined as 6.5 mm [50]. Another study concerning SES failure also supported that MSA < 5.5 mm2 and < 5.0 mm2 were the most important predictors of SES failure (Fig. 3) [22,51]. Even if SES had a considerably lower optimal MSA threshold than BMS, these studies showed that underexpansion remained the main cause of stent failure in DESs; at least a MSA < 5.0 mm should be avoided in non-left main (LM) lesions. In LM lesions, optimal MSA was reported in the MAIN-COMPARE (revascularization for unprotected left main coronary artery stenosis: comparison of percutaneous coronary angioplasty versus surgical revascularization) study to be > 8.7 mm2 to prevent TLR [34].
Edge dissection, which is complicated by lumen narrowing < 4 mm2 or dissection angle Ōēź 60┬░, has been associated with an increased incidence of early ST [49]; thus, additional stents may be needed to prevent ST. However, a minor dissection, detected by IVUS, may not be associated with an increased incidence of ST [52,53]. Although no consensus exists on an optimal strategy, in minor dissection, careful observation without stenting can be helpful.
Overall, the results discussed above encourage ensuring good apposition of stent struts to the vessel wall, such that the stent struts are not surrounded by lumen, adequate stent expansion to obtain MSA at least > 6.5 mm2 for BMSs and > 5.0 mm2 for DESs or MSA > 90% of the distal reference lumen CSA, and lack of major dissections, intramural hematomas, and geographic misses.
OUTCOMES OF IVUS-GUIDED VERSUS ANGIOGRAPHY-GUIDED PCI
Numerous studies have evaluated the clinical benefits of IVUS-guided PCI compared with angiography-guided PCI in the BMS era [41-44]. The OPTICUS trial showed no significant difference between IVUS- and angiography-guided PCI groups in terms of 6- and 12-month rates of death, myocardial infarction (MI), and TLR in 550 patients meeting the MUSIC criteria [42]. In contrast, the TULIP study demonstrated favorable angiographic and clinical outcomes in patients with long coronary lesions (> 20 mm) treated with a BMS (> 3 mm) under IVUS guidance [41]. In a meta-analysis of 2,193 patients from seven randomized trials, the rates of 6-month angiographic restenosis and target vessel revascularization were significantly lower in the IVUS-guided PCI group than the angiography-guided group (22% vs. 29%, p = 0.02 and 13% vs. 18%, p < 0.001, respectively), with no difference in the rates of death (2.4% vs. 1.6%, p = 0.18) or MI (3.6% vs. 4.4%, p = 0.51) [44], consistent with a previous meta-analysis [43].
To date, few studies have investigated the clinical benefits of DES optimization under IVUS guidance compared with that of BMSs. The HOME DES IVUS (long-term health outcome and mortality evaluation after invasive coronary treatment using drug-eluting stents with or without IVUS guidance) study was a randomized trial to investigate clinical outcomes of IVUS-guided PCI with DESs. Although the IVUS-guided strategy resulted in the frequent use of adjunctive balloons and a larger size balloon with higher pressure, no significant difference was observed in major adverse cardiac events or stent thrombosis in the study [45]. A similar retrospective study of IVUS-guided stent optimization also showed no significant difference in the incidence of in-stent restenosis or neointimal volume between IVUS- versus angiography-guided PCI [54]. Conversely, a study with a propensity-matched analysis in 884 patients treated with DESs showed a significant reduction in the stent thrombosis rate at both 30 days (0.5% vs. 1.4%, p = 0.046) and 12 months (0.7% vs. 2.0%, p = 0.014) in the IVUS-guided PCI group [47].
Recently, a large "real world" registry from two Korean centers reported long-term outcomes of both IVUS- and angiography-guided PCI using BMS or DES implantation [55]. In total, 8,371 patients who underwent coronary stenting under IVUS guidance (4,627 patients) or angiography guidance (3,744 patients) were consecutively enrolled, and 3-year adverse clinical outcomes were compared between the groups using a Cox regression model and propensity score matching. In the overall population, the 3-year adjusted incidence of mortality was significantly lower in the IVUS-guided PCI group compared with the angiography-guided PCI group (hazard ratio [HR], 0.70; 95% confidence interval [CI], 0.56 to 0.87; p = 0.001) (Fig. 4). In 2,715 matched pairs of the overall population, the IVUS-guided PCI group also had a lower mortality risk (HR, 0.71; 95% CI, 0.56 to 0.90; p = 0.005). However, IVUS-guided PCI did not influence the rates of myocardial infarction, target-vessel revascularization, or stent thrombosis in the overall or in the 2,715 matched-pair populations. In the DES subpopulation, IVUS guidance significantly reduced the 3-year adjusted mortality rate (HR, 0.55; 95% CI, 0.36 to 0.78; p = 0.001), which was not the case in the BMS subpopulation (HR, 0.79; 95% CI, 0.59 to 1.05; p = 0.10). A propensity score matching analysis of 201 matched patients from the MAIN-COMPARE study also demonstrated the importance of IVUS-guided PCI in unprotected left main disease [34]. In this analysis, significantly lower incidence of 3-year mortality was noted in the IVUS-guided PCI group compared with the angiography-guided PCI group (4.7% vs. 13.6%, p = 0.048), but no significant difference was detected in the rates of TVR or MI. Notably, this benefit was found only for DES, and the benefit in mortality appeared to be primarily associated with reduced sudden cardiac death related to late stent thrombosis. Similar findings were also observed in patients undergoing PCI of non-left main bifurcations with DESs [35]. Taken together, the benefit of IVUS guidance contributed primarily to decreased rates of stent restenosis and repeated revascularization in the BMS era, whereas reduction of the stent thrombosis rate with possible improvement in mortality have predominated in the DES era.
CONCLUSIONS
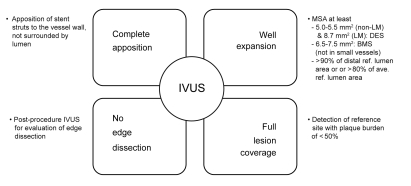
IVUS can provide direct cross-sectional images as well as longitudinal images of the coronary vessel wall. It has also contributed to our understanding of mechanisms in coronary atherosclerotic plaques and provided real-time information at stented segments after coronary interventions. Possible criteria for optimal stent deployment by IVUS are complete stent apposition to the vessel wall, adequate stent expansion, and full lesion coverage without edge dissection (Fig. 5). Recent data suggest that IVUS-guided PCI may reduce long-term mortality when compared with angiography-guided PCI, particularly after DES implantation; thus, the clinical importance of IVUS-guided PCI raised in the BMS era persists in the DES era. Optimization of stent deployment by IVUS during PCI may be considered as a routine practice in daily PCI, especially for complex lesion intervention.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





