


INTRODUCTION
Esophageal variceal hemorrhage (VH) is a grave complication of liver cirrhosis with portal hypertension. The annual incidence of first VH is 5% to 15% per year, leading to significant mortality [1]. Non-selective ╬▓-blocker (NSBB) therapy and endoscopic variceal ligation (EVL) are the primary tools for prophylaxis of esophageal VH [1,2], and meta-analysis shows that NSBB use reduces the risk of VH [3]. Accordingly, current guidelines recommend NSBBs for cirrhotic patients with increased risk of VH [1,2,4]. However, the risk of bleeding is not completely eliminated by NSBBs and a significant number of patients develop VH during NSBB therapy [5-18]. Therefore, it is necessary to identify patients who have increased risk of primary prophylaxis failure.
The hemodynamic response to NSBBs, i.e., a hepatic venous pressure gradient (HVPG) < 12 mmHg or at least 10% to 20 % reduction from baseline pressure, is the most reliable predictor of the efficacy of prophylaxis [5,8,13,19]. However, HVPG cannot be readily measured in routine clinical practice due to its invasive nature. The North Italian Endoscopy Club (NIEC) index and its variations, composed of scores for Child-Pugh class, size of varices and red wale markings, are validated as significant predictors of first esophageal VH [20-23]. However, it is less well defined whether these indices are still valid in predicting primary prophylaxis failure. Non-invasive measurement of liver/spleen stiffness can predict the presence of clinically significant portal hypertension [1], and several studies have demonstrated promising predictive power for VH [24-26]. However, the heterogeneity of studies with respect to etiology, treatment of underlying disease, prophylactic therapy, type of measurement and cut-off values calls for further validation.
Liver volume measurement has been used to predict operative outcomes in decompensated liver diseases [27-29]. Previous studies reported a correlation between liver volume and functional reserve in cirrhotic patients [30-36]. We also demonstrated that liver volume may be utilized as a predictive marker of hepatocellular carcinoma [37]. From these results, it may be speculated that liver volume may reflect the stage of cirrhosis and possibly portal pressure. However, liver volume has not been studied as a surrogate marker for elevated portal pressure or predictor of VH in cirrhotic patients.
The aim of this study was to determine whether liver volume predicts the risk of esophageal VH in patients with liver cirrhosis who are on propranolol as for primary prophylaxis. Since conventional survival analysis using the Kaplan-Meier method may be inappropriate for an alternative outcome (e.g., deaths) [38,39], we adopted a competing-risk analysis model for the assessment of prophylaxis failure.
METHODS
Study design and population
This single center retrospective cohort study enrolled consecutive patients aged over 18 years with liver cirrhosis who visited our tertiary referral center in South Korea between April 2003 and October 2015 and received propranolol for the primary prophylaxis of esophageal VH. The electronic medical records were retrieved from a structured chronic liver disease database (BESTCare) [40]. Liver cirrhosis was defined by ultrasonographic findings of coarse liver echotexture with nodularity plus evidence of portal hypertension (splenomegaly, thrombocytopenia or varices). The following were excluded from the study cohort: (1) duration of propranolol prophylaxis < 6 months, (2) previous history of bleeding and/or EVL before propranolol therapy, and (3) lack of contrast-enhanced liver computed tomography (CT) data within 6 months before or after first propranolol dosage. The necessity for CT was determined at the discretion of the attending physician under diverse clinical settings including poor sonic window, abnormal ╬▒-fetoprotein levels or detection of suspicious nodule(s) with ultrasound that warranted further characterization.
The Institutional Review Board of Seoul National University Bundang Hospital approved this study (IRB No: 1608-359-101). All clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki. Informed consent was waived by the IRB, due to the retrospective observational nature and anonymous analysis of data.
Measurement of outcomes
Screening esophagogastroduodenoscopy was recommended for all cirrhotic patients and esophageal varices were graded as small, medium or large [4]. Propranolol prophylaxis was recommended according to the Baveno IV consensus [41]: (1) presence of medium-large esophageal varices or (2) small varices with red color signs or Child-Pugh class C. Propranolol was administered orally at starting dose of 10 to 40 mg per day and adjusted to achieve 25% reduction in resting heart rate a decrease to 55 beats per minute, a maximum dose of 160 mg, or the maximum tolerable dose [41]. Propranolol was not recommended if patients had contraindications such as bronchial asthma, chronic obstructive pulmonary disease, uncontrolled heart failure, sinus bradycardia < 60/minute or heart block greater than first degree.
The primary end point of analysis was the first esophageal VH, defined by hematemesis or melena with endoscopic evidence of recent or active esophageal VH. Deaths were regarded as a competing risk and treated accordingly, since treatment of deaths as simple censored cases may bias the estimated outcomes. Bleeding other than esophageal VH, i.e., gastric VH or portal hypertensive gastropathy, were treated as censored cases. Patients who received prophylactic EVL while on propranolol were also analyzed as censored cases.
Measurement of liver volume
Liver volume was measured on the cross-sectional images of the portal venous phase of liver CT by using Image J version 1.50i (Research Services Branch, National Institute of Mental Health, Bethesda, MD, USA; http://imagej.nih.gov/ij) as previously reported with minor modifications [42]. Briefly, image slices were downloaded and boundaries of the liver area were using the Versatile Wand Tool plug in (https://imagej.nih.gov/ij/plugins/versatile-wand-tool/index.html). The inferior vena cava and gallbladder were excluded from selection, whereas intra hepatic portal veins were included in the measured areas. The measured area was summed and multiplied by slice thickness to yield the liver volume.
Since body build may affect liver volume [37,43], normal variance was adjusted by calculating the ŌĆ£liver volume indexŌĆØ as an indicator of hepatic shrinkage:
The formula for liver volume was deduced from the body surface area (BSA): formula liver volume (mL) = 893.485 ├Ś BSA ŌĆō 439.169 (mL) [43].
The BSA was estimated with Du BoisŌĆÖ formula: BSA = 0.007184 ├Ś (weight in kg)0.425 ├Ś (height in cm)0.725 [44].
Statistical analysis
All statistical analyses were performed using STATA version 14 (StataCorp, College Station, TX, USA) or R package version 3.3.2. Continuous and categorical variables were analyzed using StudentŌĆÖs t test or the Mann-Whitney rank sum test and chi-square test, respectively. In order to adjust for mortality not associated with esophageal VH during follow-up, competing-risks regression analysis was performed using R package mstate and rms. The cumulative incidence of prophylaxis failure and covariate analysis was estimated using the Fine and GrayŌĆÖs proportional subhazards model [45]. The proportionality of cause-specific hazards was confirmed with the log-log curves (STATA stphplot) for categorical variables and Schoenfeld residuals for continuous variables. Comparison of cumulative incidence with competing-risks was made by stcrreg function of STATA. The rms package of R was used to generate a nomogram from the Cox model with multiple outcomes. Comparison of bleeding prediction models was performed using time-dependent receiver operating characteristic (ROC) analysis with competing risks with the ŌĆ£timeROCŌĆØ package of R.
RESULTS
Baseline patient characteristics and incidence of esophageal VH during primary prophylaxis with propranolol
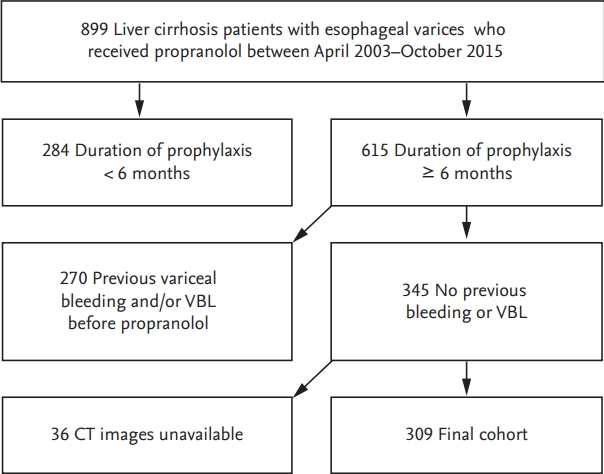
Among 899 patients with liver cirrhosis who received prophylactic propranolol therapy, 590 were excluded and 309 were finally recruited (Fig. 1). Baseline characteristics of the study population are shown in Table 1. The median duration of propranolol prophylaxis was 36 months (interquartile range, 41), and the median dosage of propranolol was 40 mg/day (range, 10 to 240). Eight patients received prophylactic EVL and censored (2.6%). During the study period 37 patients developed esophageal VH (Fig. 2) and 10 patients bled outside of esophagus. The cumulative incidences of prophylaxis failure in the presence of competing risk, i.e., death were 6.2%, 12.0%, 19.2%, 21.9%, and 24.5% at 2, 4, 6, 8, and 10 years, respectively. Patients with prophylaxis failure showed higher frequency of large (F3) varices and red color sign and lower frequency of ascites. Liver and spleen volumes were not significantly different between the two groups. However, liver volume index, an estimated-to-actual liver volume index corrected for patientsŌĆÖ body build, was significantly higher in the prophylaxis failure group, indicating that corrected liver volume was significantly smaller in patients without prophylaxis failure (Table 1).
Liver volume correlate with severity of cirrhosis
The liver volume was significantly smaller in decompensated cirrhosis (1,064 ┬▒ 401 mL vs. 1,198 ┬▒ 408 mL in Child B/C vs. Child A cirrhosis, respectively; p = 0.004). The volume index was also lower in Child B/C cirrhosis (0.727 ┬▒ 0.290 vs. 0.802 ┬▒ 0.223, p = 0.011). The liver volume index showed better correlation with Model for End-Stage Liver Disease (MELD) score than simple liver volume (PearsonŌĆÖs correlation coefficient, ŌĆō0.241 vs. ŌĆō0.191, p < 0.001).
Liver volume index as an independent predictor of propranolol prophylaxis failure
Competing-risks regression analysis showed that variceal size, red color signs, absence of ascites and high liver volume index > 1.0 were significant predictors of esophageal VH during prophylactic propranolol therapy, whereas Child-Pugh or MELD scores were not predictive of prophylaxis failure (Table 2). Subgroup analysis showed that the subdistribution hazard ratio was higher in patients with high volume index in non-alcoholic cirrhosis (5.05; 95% confidence interval [CI], 2.14 to 11.90; p < 0.001), but the volume index was not significant predictor in alcoholic cirrhosis (1.19; 95% CI, 0.33 to 4.28; p = 0.788). Covariate analysis by Fine and Gray model showed that large varices, absence of ascites and high liver volume index remained independent predictors of propranolol prophylaxis failure. Neither simple liver volume nor spleen volume predicted bleeding risk.
Development of a predictive model for propranolol prophylaxis failure
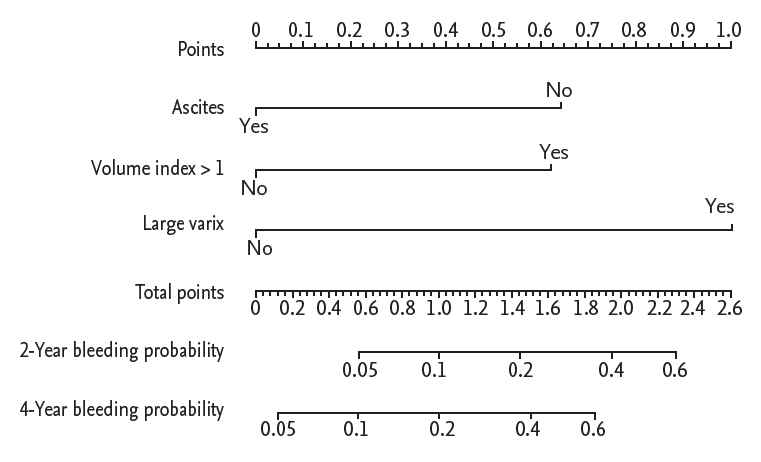
A nomogram was developed from the independent Cox models for predicting propranolol prophylaxis failure (Fig. 3). The nomogram scores for large varices, absence of ascites and high liver volume index were 1, 0.64, and 0.62, respectively. Discrimination analysis showed that patients with a nomogram score > 0.6 showed significantly higher incidence of prophylaxis failure compared to patients with low scores (subdistribution hazard ratio, 7.54; 95% CI, 2.88 to 19.73; p < 0.001) (Fig. 4).
We then compared the performance of the nomogram-based prediction model with that of the previously validated NIEC index and revised NIEC index [20,23]. Time-dependent ROC analysis revealed that the nomogram-based risk score had significantly better discriminatory power compared to that of the NIEC index or revised NIEC index in predicting propranolol prophylaxis failure at 6 and 8 years (Fig. 5).
DISCUSSION
Current guidelines recommend primary prophylaxis with NSBB for patients with risk factors [1,2,4], but 2.5% to 20% of patients still develop esophageal VH despite NSBB prophylaxis (Table 3). Our cohort showed 6.2% and 12.0% prophylaxis failure rates at 2 and 4 years, respectively, similar to previous reports. If patients at high-risk for prophylaxis failure can be identified in advance, more active intervention such as enhanced surveillance, HVPG-directed NSBB titration or prophylactic EVL may be justified.
Various combinations of clinical and hemodynamic parameters have been reported as predictors of prophylaxis failure (Table 3), but none has been universally accepted. In this study, we found that large variceal size (F3 varix), absence of ascites and liver volume index > 1 were independent predictors of prophylaxis failure in cirrhotic patients on propranolol therapy for esophageal VH prevention. Variceal size but not liver volume has been previously reported as a predictor of prophylaxis failure (Table 3). In this study, high liver volume index and absence of ascites were associated with increased risk of prophylaxis failure.
Our data indicate that propranolol prophylaxis failure is less frequent in patients with more advanced cirrhosis, i.e., small liver volume and/or presence of ascites. Although seemingly counter-intuitive, our data is in line with the recent study from United States veterans hospitals in which presence of hepatic encephalopathy, another indicator of decompensation, was associated with lower risk for prophylaxis failure [18]. The exact mechanism(s) of this finding is not clear. We suppose that although the risk of initial bleeding may be higher in patients with smaller liver volume and/or ascites, these patients may experience greater prophylactic effect of NSBB, i.e., more profound drop in portal pressure, leading to lower risk for bleeding while on NSBB. Since propranolol undergoes first pass metabolism in the liver [46], increasing intra- and extrahepatic portosystemic shunt in leads to increased bioavailability of propranolol, which may in turn potentiate reduction of portal pressure. If small liver volume index can predict portosystemic shunt more accurately compared to Child-Pugh score or MELD score, then volume index may be a better predictor of NSBB response, as indicated in our multivariate analysis. However, this explanation is only speculative because we did not measure the actual portal pressure in our patients. Further studies will be needed to confirm the potentially differential response to NSBB between compensated and decompensated cirrhosis.
There have been concerns regarding the use of NSBB in decompensated cirrhosis with ascites [47,48], advocating the concept of ŌĆ£window hypothesis for ╬▓-blockersŌĆØ: NSBB may be harmful in the end-stage cirrhosis with refractory ascites [49]. However, contradicting results exist and recent meta-analyses indicate that NSBB does not increase mortality in decompensated cirrhosis [50,51]. It is also possible that the favorable hemodynamic effect of NSBB in patients with small volume index may not be necessarily translated to survival improvement. The effect of NSBB on the overall survival of patients with small liver volume and/or ascites may warrant further prospective studies. In the meantime, since prophylactic EVL may not be free of risks, we believe that these patients may choose NSBB for primary prophylaxis, with special attention to cardiac compensatory reserve [49].
Time-dependent ROC analysis with competing-risks showed that our model based on liver volume index had better predictive power compared to that of the conventional and revised NIEC index. The revised NIEC index indicates that the weight of the Child-Pugh score is limited [23]. Serum albumin, bilirubin, and prothrombin time may show fluctuation during the course of cirrhosis, so that the liver volume index may be an alternative marker for severity of cirrhosis. Compared to previous reports of volumetric, our measurement method utilized the semi-automatic selection plug-in of Image J freeware which allows reproducible measurements with ease [42]. Typical measurement of one patient took 5 to 10 minutes in experienced hands by using the edge-detecting tool. Our method can be implemented in any picture archiving and communication systems without additional analysis tools. We also reported that our semi-automatic method show good reproducibility with minimal inter-observer variation [37].
There are several limitations in this study. First, HVPG was not measured in our cohort, so that the correlation between portal pressure and liver volume is speculative at this stage. Further studies are needed to elucidate the relationship between liver volume and portal pressure in cirrhotic patients. Second, since this was a retrospective single-center cohort study, prospective validation studies are needed to determine the predictive power of the volume index in a larger population. Third, we did not access liver and spleen stiffness which may stratify the risks of prophylaxis failure. Examination of the relationship between liver volume and liver stiffness measurement may be warranted with respect to the hemodynamic response to NSBB in further studies. Fourth, the median dosage of propranolol was at the lower recommended end (40 to 80 mg/day) [1]. Competing risks analysis showed that propranolol dosage was not a significant predictor (Table 2), but patients with relatively preserved liver volume may have benefited from higher dose of propranolol.
In conclusion, liver volume index is an independent predictor of first VH and a nomogram-based volume score stratifies the bleeding risks in patients on propranolol prophylaxis.
KEY MESSAGE
1. Computed tomography-measured liver volume is an independent predictor of first variceal bleeding in cirrhotic patients on propranolol prophylaxis, along with variceal size and absence of ascites.
2. A nomogram based on liver volume can reliably estimate the probability of first variceal bleeding in cirrhotic patients on propranolol prophylaxis.
3. The nomogram-derived volume score has superior predictive performance compared to conventional predictors such as North Italian Endoscopy Club (NIEC) score and revised NIEC score.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





