


To the Editor,
Lead poisoning or plumbism can present with nonspecific signs and symptoms, such as abdominal pain, constipation, irritability, and anemia. The manifestations of lead poisoning can also vary from individual to individual [1]. Unrecognized lead poisoning with symptoms of colicky abdominal pain can be misdiagnosed and lead to an unnecessary gastrointestinal evaluation and abdominal surgery. We experienced a patient with lead poisoning presenting with hemolytic anemia and colicky abdominal pain, which delayed the correct diagnosis of lead poisoning.
A 38-year-old female visited the emergency room with severe colicky abdominal pain and constipation. She had a psychosis that was well controlled by psychiatric treatment. She had a 1-year-old daughter. After the delivery, her bowel habits changed, with alternating constipation and diarrhea. Consequently, she had taken over the counter medicine intermittently. Several days before presentation, her bowel movements had stopped, and nausea and vomiting occurred.
Her abdomen was distended and tender around the umbilicus. The bowel sounds were increased mildly. Her abdominal X-ray showed a dilated colonic loop (Fig. 1). To rule out gastrointestinal obstruction, we ordered abdominopelvic computed tomography, which showed no intraluminal lesion causing bowel obstruction. She was admitted for supportive care of ileus.
The initial laboratory tests showed only normocytic normochromic anemia (hemoglobin 10.7 g/dL) and an elevated bilirubin level (1.97 mg/dL). Two days later, follow-up tests showed progression of the anemia to 8.2 g/dL without evidence of bleeding. In the anemia work-up, marked reticulocytosis (9.15%) was noted. Other laboratory findings were compatible with hemolytic anemia, including a peripheral smear showing polychromasia, elevated lactate dehydrogenase and indirect bilirubin, and decreased haptoglobin. The Coombs test was negative. A diagnosis of Coombs-negative hemolytic anemia was made, and hemoglobin electrophoresis was ordered to work up hemoglobinopathies.
During the evaluation, the abdominal pain resolved spontaneously and the anemia improved to 9.7 g/dL without transfusion. She wanted to be discharged without further evaluation or management. We planned to see her as an outpatient 2 weeks later, but she was lost to follow-up.
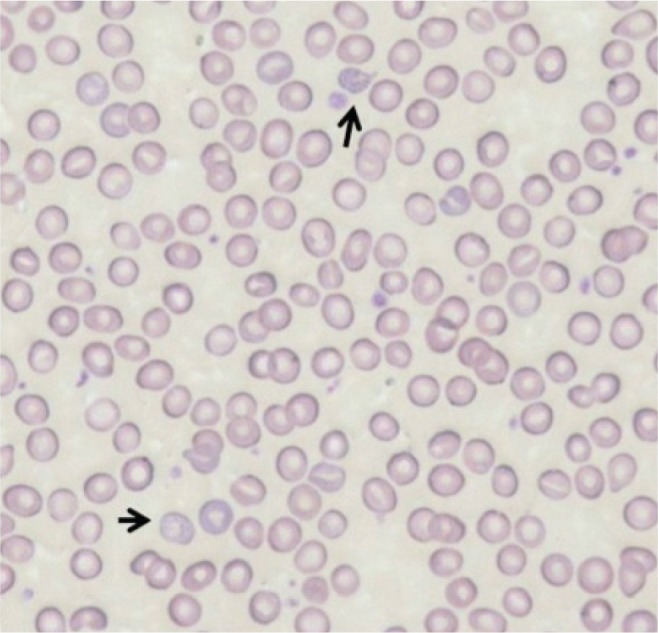
Two months later, she revisited the emergency room with the same symptoms and hemolytic anemia. The previously ordered hemoglobin electrophoresis revealed a normal pattern. We could not identify the cause of the hemolytic anemia, so we reviewed the previous peripheral smears thoroughly and found basophilic stippling on the red blood cells (Fig. 2).
We considered lead poisoning as a cause of hemolytic anemia and the other symptoms and checked the blood lead level. It was 77.8 ┬Ąg/dL. No cause of lead exposure was detected, such as occupation, food, environment, or illicit drugs. Ceramics with lead-containing glaze were not used in her household and none of the family members had jobs that involved handling lead. On repeated questioning, she admitted taking an herbal medicine for 2 weeks for constipation. Without a remaining sample of the medicine, we could not measure it for lead contamination.
After confirming lead poisoning, we started chelation therapy with intravenous calcium edetate disodium for 5 days and penicillamine orally for 4 weeks. Her hemoglobin level and abdominal pain improved after this intervention. She has remained stable, with a hemoglobin level of 12.3 g/dL and lead level of 21.0 ┬Ąg/dL at follow-up.
Lead has been used widely in both households and industry; consequently, environmental lead exposure is widespread. Lead paints, air pollution with industrial fumes and automobile exhaust, contaminated water and soil, and vegetables grown in lead-contaminated soil are among the more common causes. The majority of cases of adult lead poisoning originate from workplace exposure [1]. Inorganic lead is absorbed via the lungs, especially in adults, or from the gastrointestinal tract, which is the main exposure route in children [2]. Lead from herbal medicines is an emerging source of heavy metal poisoning, especially in Asia [3]. Chinese herbal and proprietary medicines are often adulterated with substituted herbs, heavy metals, and Western medicines. The adulterants can include heavy metals, such as lead and cadmium [4].
The Occupational Safety and Health Administration mandates that blood lead levels in workers with occupational level exposure be < 50 ┬Ąg/dL. According to the United States Centers for Disease Control and Prevention, childhood blood lead levels Ōēź 10 ┬Ąg/dL are a cause for concern. There is evidence that blood lead levels as low as 15 ┬Ąg/dL at an early age will result in subsequent psychosis and intellectual dysfunction. Therefore, studies recommended reducing the permissible lead level to Ōēż 10 ┬Ąg/dL in children [2].
The blood lead level correlates with the symptoms at presentation. A lead level below 50 ┬Ąg/dL can cause symptoms such as asthenia, arthralgia, hypertension, headache, and even infertility. Above this level, colicky abdominal pain, kidney dysfunction, hemolytic anemia, and encephalopathy can occur [1]. Measuring the blood lead concentration is the cornerstone of diagnosis, but a careful history remains important.
Lead is an electropositive metal. Its high affinity for negatively charged sulfhydryl groups leads to the inhibition of sulfhydryl-dependent enzymes, such as ╬│-aminolevulinic acid dehydrogenase and ferrochelatase in heme synthesis. This disruption of hemoglobin synthesis leads to the production of free erythrocyte protoporphyrins that can be measured. In addition, lead inhibition of pyrimidine 5'-nucleotidase can cause the degradation of ribosomal RNA in red blood cells, which can cause basophilic stippling in a peripheral smear [4].
Basophilic stippling was an important clue to the diagnosis of lead poisoning in this case. Basophilic stippling in a blood smear suggests lead intoxication, but is nonspecific. We had ordered several peripheral blood smears to evaluate the hemolytic anemia. Nevertheless, only after ruling out hemoglobinopathies were the peripheral smears reviewed thoroughly and we found basophilic stippling on the last slide. Given the maturation period of red blood cells, it might take several months of acute lead intoxication to cause basophilic stippling. This can delay the diagnosis of lead poisoning, just like in this case.
Our patient presented with recurrent abdominal pain as a symptom and hemolytic anemia as a sign. We did not recognize the disease immediately because the pain and hemolytic anemia were seemingly unrelated. Faced with a patient in Korea with Coombs test-negative hemolytic anemia, a thorough history of medicines should be taken and the possibility of lead poisoning should be considered, as enzymopathies and hemoglobinopathies are rare in Korea. The key first step in management is to stop the exposure. The medical treatment consists of chelation therapy.
In summary, lead poisoning shares symptoms with other conditions and is easily missed. Therefore, in the absence of clear causes, physicians must consider plumbism in a patient presenting with both hemolytic anemia and colicky abdominal pain. The importance of a detailed drug history, including alternative medicines, should also be emphasized.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





