Steps to understanding diabetes kidney disease: a focus on metabolomics
Article information

Abstract
Diabetic nephropathy (DN), a leading cause of chronic kidney disease and end-stage kidney disease (ESKD), poses global health challenges given its increasing prevalence. DN increases the risk of mortality and cardiovascular events. Early identification and appropriate DN management are crucial. However, current diagnostic methods rely on general traditional markers, highlighting the need for DN-specific diagnostics. Metabolomics, the study of small molecules produced by metabolic activity, promises to identify specific biomarkers that distinguish DN from other kidney diseases, decode the underlying disease mechanisms, and predict the disease course. Profound changes in metabolic pathways are apparent in individuals with DN, alterations in the tricarboxylic acid cycle and amino acid and lipid metabolism, suggestive of mitochondrial dysfunction. Metabolomics aids prediction of chronic kidney disease progression; several metabolites serve as indicators of renal functional decline and the risk of ESKD. Integration of such information with other omics data will further enhance our understanding of DN, paving the way to personalized treatment. In summary, metabolomics and multi-omics offer valuable insights into DN and are promising diagnostic and prognostic tools.
INTRODUCTION
Diabetic nephropathy (DN) is the predominant cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD). The prevalence of DN is increasing not only in Korea but also globally [1,2]. Individuals with CKD and ESKD are at heightened risk of all-cause mortality and cardiovascular events [3,4]. Patients with diabetes mellitus (DM) undergoing dialysis experience a shorter duration of survival than those without DM undergoing dialysis [5]. Early identification and effective management of DN are crucial to prevent progressive kidney dysfunction and ESKD. Ongoing pharmaceutical research seeks to provide new therapeutic options for diabetic kidney disease (DKD) [6,7]. However, the lack of specific indicators of DM-induced kidney damage poses challenges. Current assessments rely on general markers, such as albuminuria and the estimated glomerular filtration rate (eGFR), which reveal kidney damage caused by various conditions including DM [8]. There is a need for specific methods that diagnose kidney damage associated with DM. DN alone does not fully account for kidney failure in patients with DM [9]; DN affects only approximately 40% of patients with type 1 or 2 DM [10]. Although changes in diabetic retinopathy (DR) are indicative of DN, they do not consistently precede the condition in patients with type 2 DM [11]. Only 60–65% of type 2 DM cases exhibit DN nephropathy [12]. Thus, the low negative predictive value of DR poses challenges to the diagnosis of DN. Although kidney biopsy can confirm DN, its invasiveness, and impracticality for repeat biopsies over an extended period limit its utility. Notably, the rate of renal function decline in patients with DN varies considerably even among individuals with similar baseline renal function [13]. Given these challenges, additional biomarkers are needed to better diagnose and predict the progression of DN.
Metabolomics is one of the omics research fields that systematically study small organic metabolites generated or consumed during metabolic processes [14,15]. The aim is to comprehensively understand why certain compounds are produced via metabolic activities, measure changes in their levels, and use the data to gain insights into the status and functionality of biological systems. As human diseases and pathological conditions are associated with metabolic changes, interest is growing in the use of metabolomics to discover diagnostic biomarkers and potential therapeutic targets [16,17]. Metabolomics may reveal the mechanisms underlying disease, identify valuable biomarkers, aid drug development, and assess environmental toxicity. Metabolomics researchers are active in various fields associated with kidney disease, including acute kidney injury, CKD, hemodialysis, peritoneal dialysis, and kidney allograft rejection [18–20]. In terms of kidney disease research, metabolomics encompasses biomarker discovery, insights into the various pathophysiologies, support for personalized medicine, monitoring of treatment responses, and investigation of the effects of nutrition. Changes in various metabolic pathways are apparent in DM and DN patients, in which metabolic abnormalities may play a central role [21,22]. Metabolomics aids our understanding of complex metabolic changes, permits early diagnosis, and predicts DN prognosis. This review explores the applications of metabolomics, particularly the advantages afforded in terms of diagnosing DN and predicting CKD progression in individuals with DN.
NOVEL APPROACHES DISTINGUISHING DN FROM NON-DN
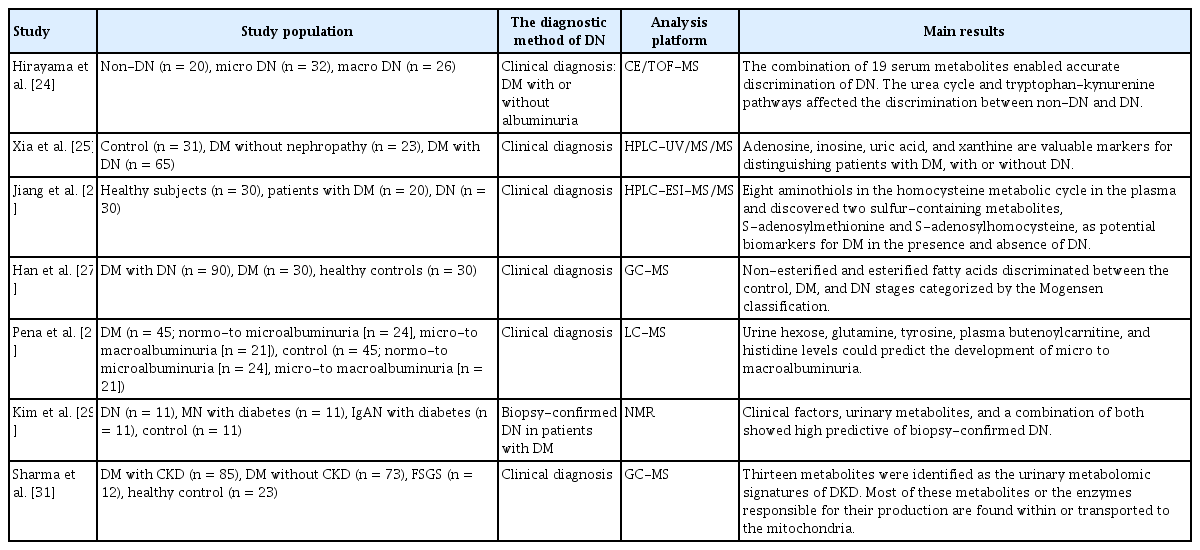
When diabetics exhibit a decline in kidney function or proteinuria, it does not necessarily mean that they have DN. Other glomerular diseases concurrent with diabetes may explain the observations. In particular, DN is less likely when diabetes is of short duration, active urinary sediments are present, kidney function declines rapidly, or DR is absent [11]. Several studies have sought to use metabolomics to differentiate DN from other renal diseases in DM patients (Table 1) [23]. Hirayama et al. [24] used capillary electrophoresis-mass spectrometry (CE-MS) to show that the levels of 19 serum metabolites distinguished non-DN and DN status. Metabolites of the urea cycle and tryptophan–kynurenine pathways were particularly important in this regard. Using liquid chromatography-mass spectrometry (LC-MS), Xia et al. [25] reported that adenosine, inosine, uric acid, and xanthine levels were useful to distinguish patients with DM with versus without DN. Jiang et al. [26] used LC-tandem MS to simultaneously quantify the levels of eight plasma aminothiols in the homocysteine metabolic cycle and discovered that two sulfur-containing metabolites, S-adenosylmethionine and S-adenosylhomocysteine, were potential DM biomarkers in patients with or without DN. Han et al. [27] showed that the levels of non-esterified and esterified fatty acids discriminated among controls, DM patients, and patients with DN categorized using the Mogensen classification. Metabolites associated with inflammation were affected in all three groups. Pena et al. [28] found that urine hexose, glutamine, and tyrosine levels, and plasma butenoylcarnitine and histidine concentrations, predicted progression from micro- to macro-albuminuria. In most previous studies, DN was clinically diagnosed. However, the recent DIAMOND study targeted patients with biopsy-confirmed DN and found that integration of clinical factors with urinary metabolite levels accurately predicted biopsy-confirmed DN in patients with type 2 DM [29]. The cited authors compared the urinary metabolomic profiles of patients with type 2 DM with biopsy-confirmed DN, DM with immunoglobulin A nephropathy (IgAN), DM with membranous nephropathy (MN), and a healthy control group (living donors scheduled for kidney transplantation). Four urinary metabolites (alanine, choline, N-phenylacetylglycine, and trigonelline) quantitated via non-targeted nuclear magnetic resonance (NMR) spectroscopy exhibited projection scores > 1 and areas under the curves > 0.7 (all p < 0.05); all were predictive of DN. Clinical factors (age, the presence of DR, DM duration, and the hemoglobin A1c [HbA1c] level), the concentrations of urinary metabolites, and the combination of clinical and metabolic markers were highly predictive of biopsy-confirmed DN status.
Metabolomic studies distinguishing DN from non-DN
Recent DN metabolomic studies have reported significant alterations in several metabolic pathways including the tricarboxylic acid (TCA) cycle, amino acid and lipid metabolism, the urea cycle, and nucleotide metabolism [30]. Sharma et al. [31] coupled targeted metabolomic evaluation with systems biology tools to gain insights into the complex mechanism of DN. They compared the metabolomic profiles of diabetics with and without CKD, patients with focal segmental glomerular sclerosis, and healthy controls. Thirteen metabolites served as urinary metabolomic signatures of DKD. Most metabolites (or the enzymes responsible for their production) were always within the cytoplasm or were transported from the cytoplasm to mitochondria. Thus, it was suggested that mitochondrial dysfunction might be associated with DKD.
PREDICTION OF PROGRESSIVE KIDNEY DYSFUNCTION IN DIABETICS
Several metabolomics studies have sought to predict the progression and prognosis of DN (Table 2). In a nested case–control study with 840 participants, the levels of 12 biomarkers were significantly associated with a rapid decline in the eGFR after adjusting for covariates (baseline eGFR, albuminuria, and HbA1c level) [32]. In a study on the 1,001 type 1 and 2 DM patients in the Chronic Renal Insufficiency Cohort (CRIC), the levels of the urine metabolites 3-methylcrotonyglycine and 3-hydroxyisobutyrate (3-HIBA) were significantly negatively associated with the eGFR slope after adjusting for the above covariates [33]. In contrast, the citric and aconitic acid levels were positively associated with the eGFR slope. Also, the 3-HIBA and aconitic acid levels were associated with a higher and lower risk of kidney failure, respectively and the need for kidney replacement therapy. The cited authors suggested that the TCA cycle and amino acid metabolism, which affect mitochondrial function and angiogenesis, may be related to DN. Kwon et al. [34], in a targeted NMR metabolomics study on Korean diabetics, showed that urine myoinositol was a novel prognostic biomarker of DKD. The level increased as the DKD progressed. The predictive effects were additive to those of the eGFR and proteinuria status (conventional markers of renal dysfunction). Niewczas et al. [35] reported that abnormal plasma concentrations of specific metabolites correlated with the risk of progression to ESKD in patients with early stage DN. Their nested case–control study included 40 patients and 40 controls who had progressed to ESKD and remained alive without ESKD. The plasma levels of several baseline uremic solutes and essential amino acids, measured by MS-based global metabolomic profiling, were associated with ESKD progression, as were the gut microbiome status and fatty acid and amino acid metabolism. Of the six polyol uremic solutes significantly associated with ESKD progression, the plasma myoinositol level was the most strongly correlated after adjusting for clinical covariates (eGFR, albuminuria, and HbA1c level). Although albuminuria is prognostic of CKD progression, some DM patients exhibit progressive GFR decline even in the absence of albuminuria [36,37]. One metabolomic study enrolled non-proteinuric type 2 DM patients with or without a low eGFR (eGFR < 60 mL/min/1.73 m2). The levels of 11 gas chromatography-MS and 19 LC-MS urinary metabolites were strongly associated with a low eGFR. However, no adjustments were made for clinical covariates of DN progression. One recent study used a combination of non-targeted metabolomic assays and a comprehensive machine learning approach to predict CKD progression in patients with DKD [38]. A non-targeted metabolomic analysis of plasma and urine samples from 135 patients with stage 3 CKD and DM was used to predict DN progression. A deep learning method indicated that the systolic blood pressure, albuminuria, levels of six identified metabolites, and three unidentified metabolites, including urinary 1-methylpyridin-1-ium (NMP), were potential markers of rapid kidney function decline. The cited authors suggested that machine learning might identify potential biomarkers not detected using traditional statistical approaches.

Metabolomic studies predicting DN progression
Experiments on animals with diabetes revealed that oral glycine alleviated renal oxidative stress by reducing Nox4 expression [39]. In diabetic rats treated with glycine, mesangial expansion was attenuated, the levels of fibrosis markers were reduced, and oxidative stress was reduced. A meta-analysis of the metabolomic differences between 1,875 DKD patients and 4,503 controls identified 60 differentially expressed metabolites, of which five were essential [40]. Compared to controls, DKD patients exhibited significant decreases in the levels of glycine, aconitic acid, glycolic acid, and uracil, but they also had significantly higher cysteine levels; this suggests that DKD patients experience disrupted amino acid, lipid, and pyrimidine metabolism. Although attempts to suppress DN progression by controlling specific metabolites are still limited, these results may help suppress DN progression through continued research.
METABOLOMIC PROFILES OF DR: EVIDENCE FROM OTHER DIABETIC MICROVASCULAR COMPLICATIONS
Several micro- and macrovascular complications may develop in diabetics. DR is a major long-term complication (20% of DM patients) [41], and DR and DN may share metabolic pathways. Several studies have evaluated the metabolomic profiles of diabetics with DR [42]. The metabolites of patients with and without DR differed significantly; the fumaric acid, cytidine, uridine, and acetic acid levels correlated with DR status [43], as did dysregulation of pyrimidine, arginine, and proline metabolism. Chen et al. [44] described the plasma metabolomic profiles of 40 DR cases and controls. After adjusting for recognized risk factors, the metabolite markers were significant and consistently reliable predictors. The pentose phosphate pathway has been identified as a major metabolomic dysregulation associated with DR. Recently, Yun et al. [45] described the metabolomic profiles associated with DR development and progression in diabetics. The levels of 16 metabolites were affected in those with both nonproliferative and proliferative DR, of which three (total DMA, tryptophan, and kynurenine levels) served as indicators of DR progression in diabetics. Tomofuji et al. [46] evaluated the serum metabolites of diabetics with both retinal and renal complications. The levels of five metabolites, including N-acetylneuraminic acid, served as metabolomic signatures associated with both complications. N-acetylneuraminic acid, a primary human sialic acid, has been linked to both DKD and DR [47,48]. An association was observed between the N-acetylneuraminic acid level and the myocardial infarction risk [49]. The N-acetylneuraminic acid concentration may explain the shared etiologies of retinal, renal, and cardiovascular complications in diabetics; the metabolomic features of those with diabetic complications may be shared.
IMPROVING THE EVIDENCE: INTEGRATION AND COLLABORATION WITH OTHER OMICS
With technological advancements, multi-omics techniques, in addition to metabolomics are improving and can provide personalized precision medicine. Therefore, by merging multi-omics data, including genomics, transcriptomics, proteomics, and metabolomics, researchers may thoroughly understand DN. The use of genomics and epigenetics techniques can provide significant insights into the genetic factors that render individuals susceptible to DN [50]. Transcriptomics ensures a thorough understanding of gene expression patterns and the molecular pathways involved in DN. Proteomics identifies proteins associated with DN, suggesting potential DN biomarkers and therapeutic targets. Metabolomics studies the small molecules, metabolites, and metabolic pathways involved in DN progression. A comprehensive approach would facilitate the development of novel medications and enable customized DN treatments. Sha et al. [51] used multi-omics data, including transcriptome, proteome, and metabolome data derived using kidney biopsies and mouse DN models to show that lipid metabolism was significantly disrupted during DN pathogenesis and progression. Another study integrated metabolomic, lipidomic, and genome-wide single-nucleotide polymorphism data to identify diabetics at high risk of DKD [52]. That study used machine learning models to augment traditional methods and a protein–protein interaction network analysis to identify the molecular mechanisms. Omics data integration facilitates network-based analysis, revealing complex relationships among DN-relevant genes, proteins, and metabolites. However, translation of such insights to the clinic remains challenging given the lack of experimental validation in animal models or clinical trials. It is important to integrate multi-omics data with detailed clinical information to identify DN patient subgroups who require personalized treatment. Advances in multi-omics analysis will enhance our understanding of DN and reveal new drug targets.
LIMITATIONS OF CURRENT METABOLOMICS
Metabolomics researchers define metabolite profiles that foster an understanding of physiological status, disease status, and drug actions. However, several limitations are evident; there are pre-analytical, analytical, and post-analytical issues [53]. Metabolites have very diverse and complex structures, making data interpretation difficult. Some metabolites are unstable, and their levels change during sample processing and storage. No single analytical technique exhibits the specificity and sensitivity required to identify and quantify the entire metabolome of a single biological entity [54]. Standard operating procedures are essential; metabolite detection must be accurate and consistent if metabolomics are to be clinically relevant. Such procedures minimize analytical and batch-to-batch variability during metabolomics workflow [55]. Metabolomics research requires advanced statistical techniques and systems biology information to process and analyze large-scale data. Several methods of analysis are used to interpret data, and attempts are made to reduce the false positives by applying a false discovery rate in untargeted metabolomics [56]. Biological variations among individuals and groups are common, and it can be difficult to determine whether changes in the levels of specific metabolites are attributable to individual differences or environmental factors. Various external factors, such as environmental factors and eating habits, can affect the metabolites.
Metabolomic studies have identified several metabolites that may serve as novel biomarkers of DN. However, there is a limitation in that no consistent single metabolites has been presented. The identification of consistent single metabolites for distinguishing DN remains a challenge due to the disease’s complexity and patient variability. This emphasizes the need for further studies integrating comprehensive metabolomic profiling with multi-omics approaches. Moreover, considering patient heterogeneity is essential. Individual genetic background, the disease stage, co-existing conditions, and lifestyle choices all influence metabolic profiles. Future studies should include diverse patient cohorts and employ stratified analyses to discover biomarkers relevant in specific subgroups. Continued efforts are required to discover metabolites that better predict DN diagnosis and progression in clinical practice.
CONCLUSION
Novel biomarkers can be utilized for early detection and prediction of DN progression. Metabolomic and multi-omics techniques may aid patient-tailored DN management in future.
Notes
CRedit authorship contributions
Hyo Jin Kim: conceptualization, investigation, writing - original draft; Sang Heon Song: conceptualization, methodology, writing - review & editing, supervision
Conflicts of interest
The authors disclose no conflicts.
Funding
None