Epidemiology and risk factors associated with avascular necrosis in patients with autoimmune diseases: a nationwide study
Article information

Abstract
Background/Aims
Avascular necrosis (AVN) is a clinical condition characterized by the death of bone components due to interruption in the blood supply. This study aimed to investigate the epidemiology and determine the risk factors for AVN in patients with autoimmune diseases.
Methods
We conducted a population-based retrospective cohort analysis using claims data from the Taiwan National Health Insurance Research Database. A total of 49,636 patients with autoimmune diseases between January 1, 2005 and December 31, 2013 were included. Cox regression analysis was used to identify associated risk factors for the development of AVN.
Results
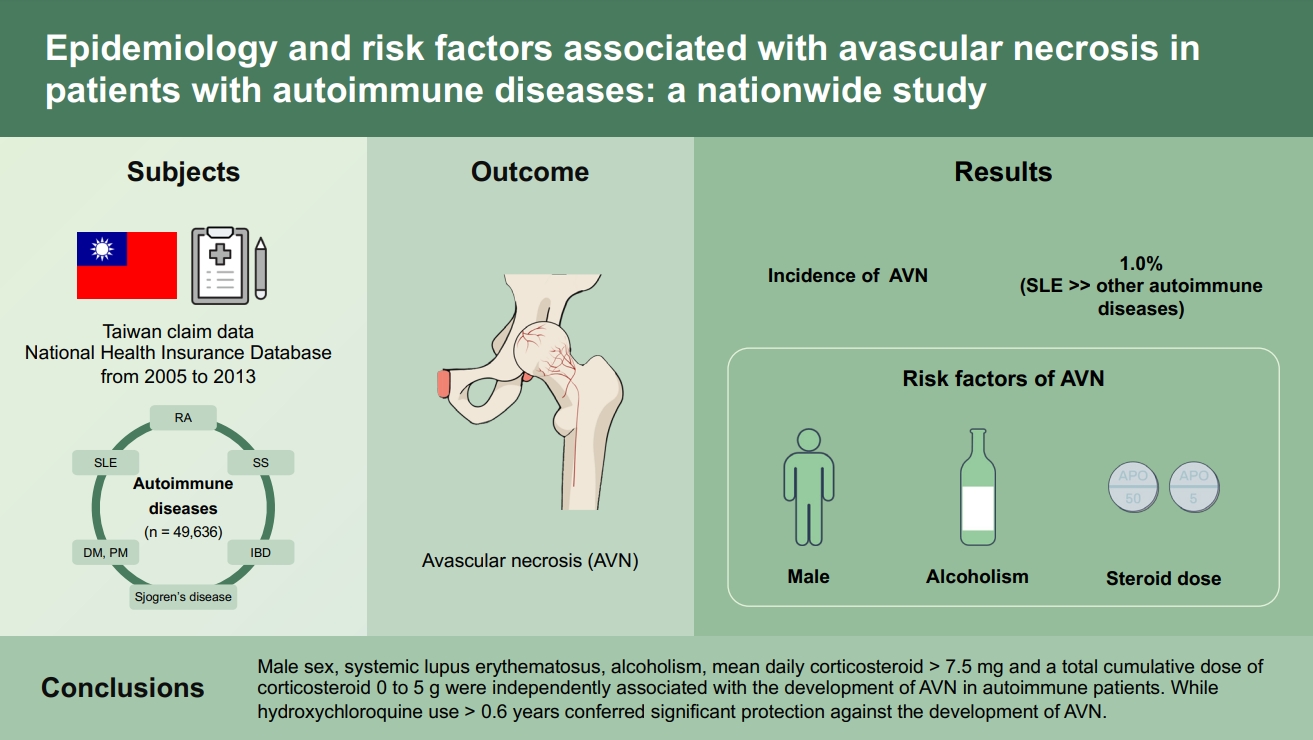
A total of 490/49,636 patients (1.0%) developed symptomatic AVN. The systemic lupus erythematosus patients had a higher risk of AVN compared to other autoimmune diseases. AVN was positively correlated with male sex (p < 0.001), alcoholism (p < 0.001), mean daily prednisolone dosage 7.51 to 30 mg (p < 0.001) and > 30 mg (p < 0.001), and total cumulative prednisolone dose 0 g to 5 g (p = 0.002). However, AVN was inversely correlated with cumulative duration of hydroxychloroquine exposure > 0.6 years (p < 0.001).
Conclusions
Male sex, systemic lupus erythematosus, alcoholism, mean daily corticosteroid > 7.5 mg and a total cumulative dose of corticosteroid 0 to 5 g were independently associated with the development of AVN in autoimmune patients. While hydroxychloroquine use > 0.6 years conferred significant protection against the development of AVN. Clinicians should regularly assess patients with risk factors to enable the early diagnosis of AVN.
INTRODUCTION
Avascular necrosis (AVN) is a clinical condition characterized by the death of bone components due to an interruption in the blood supply to the bone; it predominantly affects younger patients. As the disease progresses, the articular cartilage covering the hip bones collapses leading to osteoarthritis. However, early in the disease process AVN is often asymptomatic and discovered incidentally on radiographs. Therefore, the early diagnosis of AVN depends upon the identification of individuals at risk. The management of AVN primarily depends on the location and severity of the disease. Early detection and appropriate treatment with joint-sparing techniques, such as core decompression and vascularized fibular grafting were reported to be more successful when performed during the early stages of the disease [1–3]. Without treatment, the disease process is almost always progressive. Once irreversible damage occurs, reconstructive surgery, such as hemiarthroplasty or total joint replacement, is often necessary and can lead to significant disability. Therefore, early diagnosis and prompt medical or surgical intervention are essential for improving patient outcomes.
AVN most commonly affects the femoral head and is usually multifocal and symmetric. Other common sites affected include the upper arm, knees, shoulder and ankles. The exact pathogenesis of AVN is unclear so it continues to represent a significant challenge for clinical research. A variety of systemic diseases and clinical conditions are associated with non-traumatic AVN; chronic steroid use [4] and excessive alcohol use are two of the most common causes of AVN. A nationwide epidemiology survey performed in Japan by Fukushima et al. [5] in 2005, reported that systemic glucocorticoid therapy and alcoholism contributed to 51% and 31% of AVN cases, respectively.
Corticosteroids are prescribed to induce remission or reduce morbidity in many autoimmune diseases. The incidence of AVN was significantly higher in patients with systemic lupus erythematosus (SLE) compared with other rheumatic diseases. Klippel et al. [6] previously reported that the incidence of AVN was 8.3%, 3.7%, 3.2%, 2.3%, 2.1%, 0.4%, 0.7%, and 0.4% in patients with SLE, Wegener’s granulomatosis, dermatomyositis (DM)/polymyositis (PM), idiopathic cryoglobulinemia, polyarteritis nodosa, rheumatoid arthritis (RA), juvenile RA and Behçet’s syndrome, respectively.
Demographic factors may influence the development and progression of AVN. To the best of our knowledge, there has been no nationwide study conducted in Taiwan focusing on the prevalence of, and the factors associated with, the development of AVN in patients with autoimmune diseases. Improved understanding of AVN risk factors has therapeutic implications, as early diagnosis and treatment are important for optimizing patient outcomes. The objective of the present study was to investigate the prevalence of symptomatic AVN and the risk factors associated with its development, in a cohort of Taiwanese patients with autoimmune diseases.
METHODS
Data sources
The present study is based on data from the National Health Insurance Research Database (NHIRD), a longitudinal health insurance database provided by the Taiwan National Health Research Institute. Taiwan launched a single-payer National Health Insurance (NHI) program to provide comprehensive health care for all citizens on March 1, 1995. It currently covers > 99% of the population (approximately 23 million people). In order to avoid severe financial load on families with major illness, the NHI specified 30 categories of catastrophic illness, including cancer, chronic mental illness, end-stage renal disease, congenital illness, transplantation and several autoimmune diseases, such as SLE, systemic sclerosis, RA, DM, PM, Sjogren’s syndrome, pemphigus, and inflammatory bowel disease (IBD). Patients with these diseases may apply for catastrophic illness certification which makes them exempt from copayments for treatments for the illness or related conditions within the certificate’s validity period. All applications for catastrophic illness certification are reviewed by experts based on a review of medical records, laboratory studies and imaging studies. Therefore, the diagnosis of a catastrophic illness can be considered to be highly accurate and reliable. The NHIRD includes the entire registry and claims data from the NHI system, which includes demographic data, details of all prescription drugs administered and orders of ambulatory and inpatient care. The NHIRD is completely de-identified and encrypted and only used for research purposes. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes were used to define diseases. The present study used NHIRD datasets on special request, which included claims data from patients with autoimmune diseases between 2005 and 2013. The Institutional Review Board of Taipei Veterans General Hospital approved the present study (IRB No. 2016-08-013CC). As all personal identifying information had been encrypted before the database was released, the review board requirement for written informed consent was waived.
Inclusion and exclusion criteria for the study population
All patients in the catastrophic illness database aged ≥ 18 years, who were diagnosed with an autoimmune disease (ICD-9-CM codes 710.0 for SLE, 714.0, 714.30 to 714.33 for RA, 710.2 for Sjogren’s syndrome, 710.1 for systemic sclerosis, 710.3 for DM, 710.4 for PM, 694.4 for pemphigus and 555, 556, 556.0 to 556.6, 556.8–556.9 for IBD) between January 1, 2005 and December 31, 2013 were selected for the current study. The date of autoimmune disease onset was identified as the date of application for a catastrophic illness certificate. All enrolled index cases were followed from the date of diagnosis with autoimmune disease to the date of a first-time diagnosis with AVN, death, or the end of the study period. Patients with temporary certification of an autoimmune disease, with more than one autoimmune disease or with pre-existing AVN of the bone were excluded from the study.
Definition of AVN and surgical interventions
The study subjects were considered to have newly diagnosed AVN if they had a diagnosis of AVN (ICD-9-CM code 733.4X) in outpatient or inpatient services after the diagnosis of an autoimmune disease. For patients with AVN, the sites of articular disease affected by AVN (ICD-9-CM code 733.40 for aseptic necrosis of bone, site unspecified, 733.41 for aseptic necrosis of the humeral head, 733.42 for aseptic necrosis of the head and neck of the femur, 733.43 for aseptic necrosis of the medial femoral condyle, 733.44 for aseptic necrosis of the talus, 733.45 for aseptic necrosis of the jaw, 733.49 for aseptic necrosis of other sites) were recorded. Patients with AVN who underwent surgical intervention were identified using NHI procedure codes (64238B for core decompression, 64006B for corrective osteotomy, 64002B and 64230B for bone graft, 64169B and 64170B for hemiarthroplasty). The NHI procedure codes for total joint replacement (64162B for total hip replacement, 64163B for total shoulder replacement, 64164B for total knee replacement, 64165B for total elbow replacement, 64166B for total wrist replacement, 64167B for total ankle replacement and 64168B for total finger or toe replacement) were also identified.
Demographic data and comorbidities
The demographic data of the participating patients (including their age at onset of autoimmune disease, sex and age at diagnosis of AVN) was extracted. Patients were classified into three age subgroups: 18 to 44, 45 to 64, and ≥ 65 years. Relevant comorbidities were identified based on ≥ 2 outpatient ICD-9 codes or ≥ 1 inpatient ICD-9 code in their claims data. The following comorbidities including diabetes mellitus (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401–405), hyperlipidemia (ICD-9-CM code 272.0–272.4), gout (ICD-9-CM codes 274.0–274.9), chronic obstructive pulmonary disease (COPD; ICD-9-CM 496), asthma (ICD-9-CM 493), nephrotic syndrome (ICD-9-CM 581.XX), and proteinuria (ICD-9-CM 791.0) were identified. Patients with relevant diagnostic codes for end-stage renal disease (ICD-9-CM 585) in the catastrophic illness registry were identified.
Alcoholism
Alcoholism was defined as alcohol dependence syndrome (ICD-9-CM 303.x), alcoholism (ICD-9-CM V11.3), alcohol abuse (ICD-9-CM 305.0), alcoholic psychosis (ICD-9-CM 291.x), alcoholic polyneuropathy (ICD-9-CM 357.5), alcoholic cardiomyopathy (ICD-9-CM 425.5), alcoholic gastritis (ICD-9-CM 535.3), alcoholic fatty liver (ICD-9-CM 571.0), alcoholic cirrhosis of the liver (ICD-9-CM 571.2) and alcoholic liver damage (ICD-9-CM 571.3).
Corticosteroid, disease-modifying anti-rheumatic drug, and cyclophosphamide use
Corticosteroids and disease-modifying anti-rheumatic drugs (DMARDs) were classified using the NHI drug codes and the anatomical therapeutic chemical (ATC) codes. The systemic corticosteroids (oral or intravenous) administered included betamethasone (ATC code H02AB01), dexamethasone (ATC code H02AB02), methylprednisolone (ATC code H02AB04), paramethasone (ATC code H02AB05), prednisolone (ATC code H02AB06), triamcinolone (ATC code H02AB08), hydrocortisone (ATC code H02AB09) and cortisone (ATC code H02AB10). The cumulative doses of corticosteroids were calculated until the date of last follow-up in patients without AVN and the date of AVN onset in patients who developed AVN. All corticosteroid prescriptions were converted to prednisolone equivalents (1 mg prednisolone = 4 mg hydrocortisone = 5 mg cortisone = 0.8 mg methylprednisolone =0.4 mg paramethasone = 0.8 mg triamcinolone = 0.16 mg betamethasone =0.16 mg of dexamethasone). The mean daily prednisolone dosage was categorized into three groups: low dose (≤ 7.5 mg/day), medium dose (7.51 to 30 mg/day) and high dose (> 30 mg/day). Data on the DMARDs used to treat autoimmune diseases, including sulfasalazine (ATC code A07EC01), methotrexate (ATC code L01BA01), leflunomide (ATC code L04AA13), azathioprine (ATC code L04AX01), cyclosporine (ATC code L04AD01), penicillamine (M01CC01) and hydroxychloroquine (P01BA02), which were prescribed within the follow-up period was extracted for analysis. The hydroxychloroquine cumulative dose (g) and cumulative period of hydroxychloroquine use were calculated. Data on the cyclophosphamides (ATC code L01AA01) administered was also extracted for analysis.
Statistical analysis
Continuous data are presented as the mean ± standard deviation followed by analysis with a Student’s t test. Categorical variables were presented as percentages and compared using Fisher’s exact or chi-square tests. The Cox proportional hazards regression model was used to evaluate the candidate risk factors for AVN development. All pertinent variables, such as age at onset of autoimmune disease, sex, mean daily corticosteroid dosage and comorbidities were initially examined individually by univariate analyses. Variables with a significant association with the development of AVN (p < 0.05) during the univariate analysis were included in the multivariate analysis as covariates. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). A p < 0.05 was considered to indicate a statistically significant difference.
RESULTS
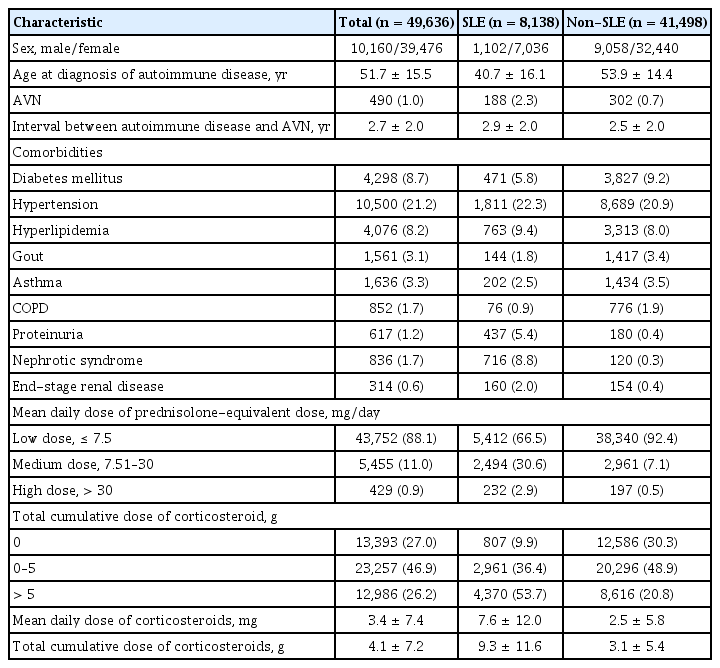
The demographic data and clinical characteristics of the patients are summarized in Table 1 and Supplementary Table 1. A total of 49,636 patients with autoimmune diseases (SLE: 8,138, systemic sclerosis: 1,157, RA: 21,895, DM/PM: 1,237, pemphigus: 856, Sjogren’s syndrome: 14,470 and IBD: 1,883) were recruited into the present study. There were 39,476 females (79.5%) and 10,160 males (20.5%), with a female-to-male ratio of 3.9:1. The majority of autoimmune diseases in the current study occurred in females, except for IBD. The female-to-male ratio was highest in Sjogren’s syndrome (8.8:1), followed by SLE (6.4:1), RA (3.2:1), systemic sclerosis (2.6:1), DM/PM (1.9:1), and pemphigus (1.1:1). The mean age at onset of autoimmune disease was 51.7 ± 15.5 years. A total of 36,243 patients (73.0%) were ever treated with corticosteroids. The mean daily prednisolone dosage was highest in patients with DM/PM (11.6 ± 20.8 mg) followed by patients with pemphigus (7.7 ± 9.0 mg), SLE (7.6 ± 12.0 mg), and systemic sclerosis (3.8 ± 8.4 mg). The percentages of SLE and non-SLE patients who received a mean daily dose of prednisolone > 7.5 mg/day were 33.5% and 7.6%, respectively. The cumulative dose of prednisolone was 9.3 ± 11.6 g in the SLE patients versus 3.1 ± 5.4 g in the non-SLE patients. The SLE patients received a significantly higher daily and cumulative prednisolone dosage compared with the non-SLE patients (p < 0.001).
Demographic characteristics and comorbidities in the patients with autoimmune diseases
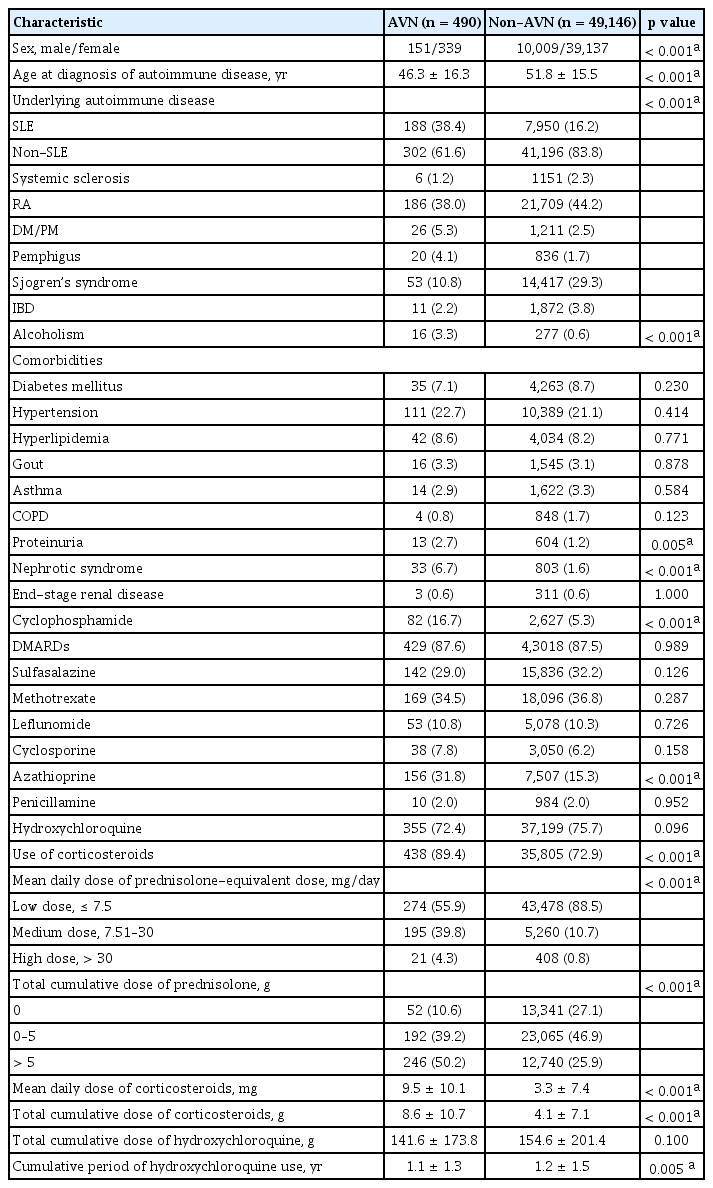
The demographic characteristics and clinical information of patients with and without AVN are summarized in Table 2. A total of 490/49,636 patients (1.0%) developed symptomatic AVN during the follow-up period. Of the AVN patients, 339 (69.2%) were female and 151 (30.8%) were male, with a female-to-male ratio of 2.2:1. Patients with pemphigus and SLE most frequently (2.3%) developed AVN, followed by individuals with DM/PM (2.1%) and RA (0.8%). A significantly higher percentage of SLE patients developed AVN compared with the non-SLE patients (2.3% vs. 0.7%, p < 0.001). The mean age at onset of AVN was 49.0 ± 16.2 years. The mean latency from the date of diagnosis with an autoimmune disease to AVN development was 2.7 ± 2.0 years. Of the patients who developed AVN, 429 (87.6%) had AVN of the hip, 11 (2.2%) had AVN of the femoral condyle, five (1.0%) had AVN of the humerus, three (0.6%) had AVN of the talus, and 42 (8.6%) had AVN at an unspecified site. Of the 490 patients with AVN, 308 (62.9%) underwent surgical interventions, and of these patients 54 (17.5%) underwent core decompression, 12 (3.9%) received a bone graft, 62 (20.1%) had a hemiarthroplasty, and 236 (76.6%) underwent a total arthroplasty. Male sex and a younger age at the onset of autoimmune disease were significantly associated with AVN onset. Hypertension was the most common co-morbidity. The patients with AVN had higher rates of coexisting hypertension, hyperlipidemia, proteinuria, nephrotic syndrome and gout, whereas the patients without AVN had higher rates of diabetes mellitus, asthma, COPD and end-stage renal disease. However, there were no significant differences in diabetes mellitus, hypertension, hyperlipidemia, gout, asthma, COPD, and end-stage renal disease between the AVN and non-AVN groups. Compared with the non-AVN group, the patients with AVN had a significantly increased proportion of comorbidities, including proteinuria and nephrotic syndrome (p < 0.001). Alcoholism was more prevalent in the AVN group (p < 0.001). Of the 490 patients with AVN, 438 (89.4%) had a history of corticosteroid use, 355 (72.4%) received hydroxychloroquine, 82 (16.7%) received cyclophosphamide, 156 (31.8%) received azathioprine, 142 (29.0%) received sulfasalazine, 38 (7.8%) received cyclosporine and 169 (34.5%) received methotrexate. AVN was significantly associated with cyclophosphamide and azathioprine use (p < 0.001). The mean daily doses of corticosteroids equivalent to prednisolone in the patients with AVN and non-AVN were 9.5 ± 10.1 and 3.3 ± 7.4 mg, respectively. The cumulative corticosteroid equivalents to prednisolone in the AVN and non-AVN patients were 8.6 ± 10.7 and 4.1 ± 7.1 g, respectively. Both the mean daily and cumulative corticosteroid dose were significantly higher in the AVN group compared with the non-AVN group. The cumulative duration of hydroxychloroquine exposure in the AVN group was significantly shorter than that in the non-AVN group (1.1 ± 1.3 years vs. 1.2 ± 1.5 years, p = 0.005). The cumulative dose of hydroxychloroquine was lower in the AVN group (141.6 ± 173.8 g vs. 154.6 ± 201.4 g), but the difference did not reach statistical significance.
Comparison of demographic characteristics and comorbidities in the patients with autoimmune diseases with and without AVN
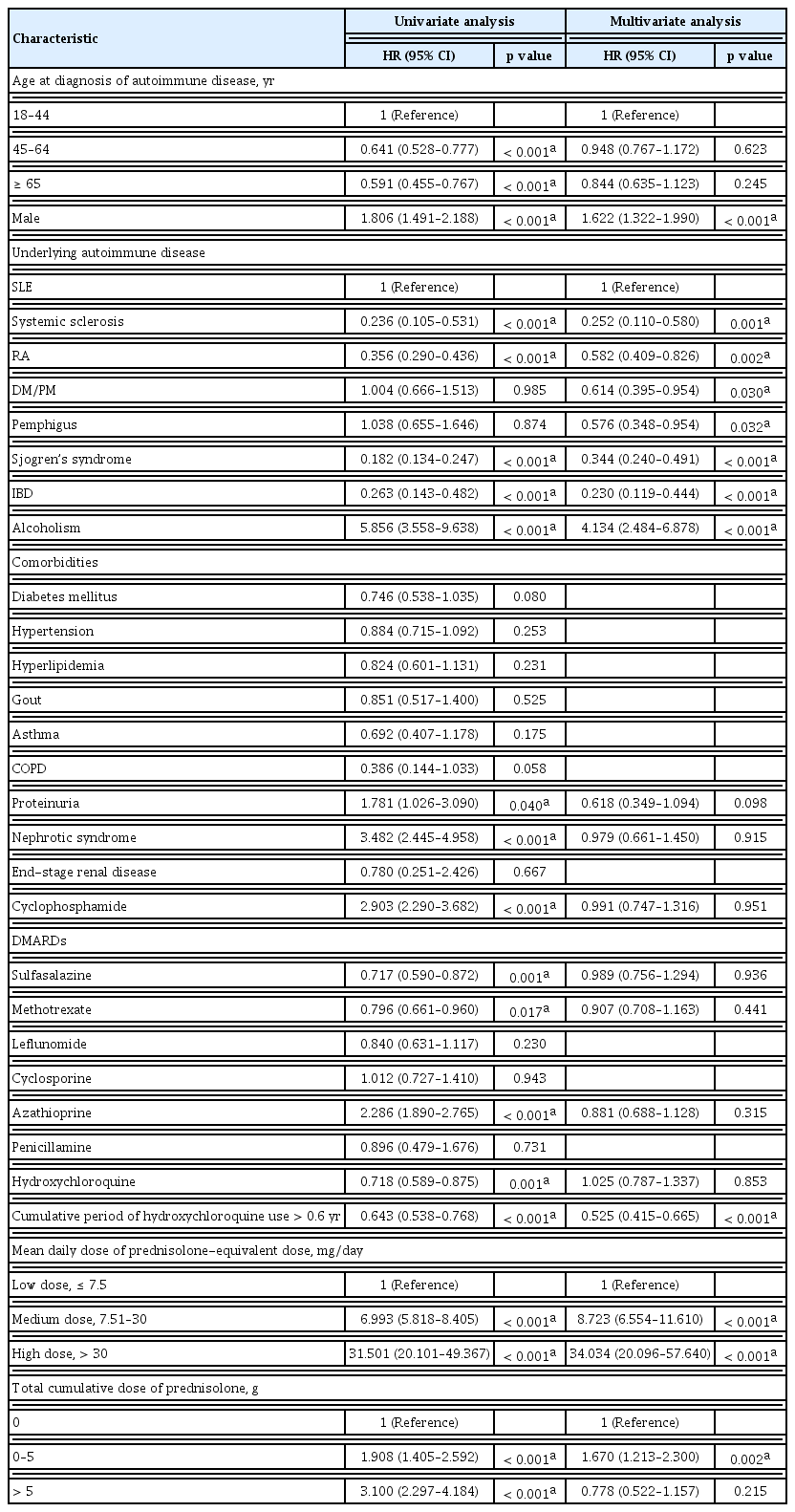
Table 3 presents the results of the univariate and multivariate analyses for associations between various demographic and clinical factors and AVN onset. In the univariate Cox regression analysis, compared to the patients with SLE, the patients with other autoimmune diseases such as systemic sclerosis, RA, Sjogren’s syndrome and IBD had a significantly lower risk of AVN. Male sex, alcoholism, proteinuria, nephrotic syndrome, azathioprine, cyclophosphamide use, a mean daily dose of prednisolone > 7.5 and 30 mg, and a total cumulative dose of prednisolone between 0 to 5 g and > 5 g were positively associated with the development of AVN. Patients aged 45 to 64 years, ≥ 65 years and with a history of sulfasalazine, methotrexate and hydroxychloroquine use were all significantly associated with a lower risk of AVN development. However, diabetes mellitus, hypertension, hyperlipidemia, gout, asthma, COPD, end-stage renal disease, use of leflunomide, cyclosporine and penicillamine were not associated with an increased risk of AVN. In the multivariate Cox regression analysis, the SLE patients had the highest risk of AVN compared to the other autoimmune diseases (systemic sclerosis: hazard ratio [HR], 0.252; 95% confidence interval [CI], 0.110 to 0.580; p = 0.001, RA [HR, 0.582; 95% CI, 0.409 to 0.826; p = 0.002], DM/PM [HR, 0.614; 95% CI, 0.395 to 0.954; p = 0.030], pemphigus [HR, 0.576; 95% CI, 0.348 to 0.954; p = 0.032], Sjogren’s syndrome [HR, 0.344; 95% CI, 0.240 to 0.491; p < 0.001], and IBD [HR, 0.230; 95% CI, 0.119 to 0.444; p < 0.001]). AVN was positively correlated with male sex (HR, 1.622; 95% CI, 1.322 to 1.990; p < 0.001), alcoholism (HR, 4.134; 95% CI, 2.484 to 6.878; p < 0.001), a mean daily prednisolone dosage between 7.51 and 30 mg (HR, 8.723; 95% CI, 6.554 to 11.610; p < 0.001), a mean daily prednisolone dosage > 30 mg (HR, 34.034; 95% CI, 20.096 to 57.640; p < 0.001) and a total cumulative dose of prednisolone between 0 and 5 g (HR, 1.670; 95% CI, 1.213 to 2.300; p = 0.002). However, AVN was inversely correlated with a cumulative duration of hydroxychloroquine exposure > 0.6 years (HR, 0.525; 95% CI, 0.415 to 0.665; p < 0.001).
Cox regression analysis of the associations between AVN and clinical factors in the patients with autoimmune diseases
DISCUSSION
AVN is a disease that causes bone death due to vascular compromise of the affected bones, and ultimately leads to destruction of the joints and loss of function. In the present study, AVN most commonly affected the femoral head, which is consistent with previous studies. The hip is most vulnerable because of the relative lack of a collateral blood supply. The management of AVN depends on its severity, and treatment outcomes are inversely correlated with the disease stage at the time of treatment initiation. It is important to diagnose AVN early to help prevent disability. Milder cases may be resolved using conservative measures, including limited weight bearing and pain medication, however surgical intervention is often necessary in patients with advanced AVN.
In the present study, 62.9% of the patients with AVN eventually required a surgical intervention. The high proportion of patients who underwent surgery highlights the high probability of a late diagnosis and the late stage of AVN in our cohort. A recent large study showed that AVN tends to develop more frequently in males [7]. The male-to-female ratio of AVN varies depending on underlying health problems. A greater male prevalence has been reported among alcohol users, while AVN associated with SLE is more common in females [8,9]. In the current study, 79.5% of the patients with autoimmune diseases were women, and there was a 2.2:1 female-to-male preponderance of AVN development, which is consistent with previous studies [10–12]. However, there was a significantly higher likelihood of developing AVN in the male patients.
The diagnostic imaging procedures used to detect AVN include radiographs, skeletal scintigraphy, computed tomography and magnetic resonance imaging (MRI). MRI has recently emerged as the most sensitive and specific tool for the detection of early lesion AVN. The prevalence rates of non-traumatic AVN in previous literature are diverse, which may be due to their dependence on varying factors including ethnicity, underlying diseases, corticosteroid dosage and the tool used for diagnosis. The prevalence of AVN among SLE patients has been reported to range between 2.1% and 52% [13–18], while the prevalence of asymptomatic AVN detected by screening MRI is generally higher [14,19,20]. The frequency of AVN in SLE patients in the present study was at the lower end of the reported rate, at 2.3%. This may be due to the variability of modalities used to determine AVN. In the present cohort, AVN was diagnosed based on claims data, so only symptomatic patients who underwent AVN evaluation were identified. Asymptomatic AVN is not an uncommon finding in SLE patients receiving high dose corticosteroids [14]. Consequently, the study data may underestimate the frequency of AVN. Furthermore, ethnic differences are potentially associated with the frequency of AVN development.
Unlike the much higher rates of AVN diagnosed by MRI in DM/PM, systemic scleroderma, ulcerative colitis and pemphigus patients, as reported by Shigemura et al. [17], the present study observed that AVN occurred in 2.3%, 0.5%, 0.6% and 2.1% of patients with pemphigus, systemic scleroderma, IBD and DM/PM, respectively. The use of MRI screening for diagnosing AVN and the sample size of non-SLE rheumatologic disorders was small, which may have resulted in the high rate of AVN observed by Shigemura et al. [17]. For pemphigus, the results of the current study are comparable with those of a previous Iranian epidemiology survey (1.93%) [21]. In the present study, the low rate of AVN in patients with RA is similar to a study conducted by Klippel et al. [6].
AVN is a well-recognized complication of SLE, which was first described in 1960 by Dubois and Cozen [22]. The current study revealed that the patients with SLE had the highest risk of AVN compared with other non-SLE autoimmune diseases, which is consistent with most other population-based studies conducted in Western countries. Shigemura et al. [17] reported that SLE patients had a significantly higher risk of developing AVN compared with other collagen diseases, with an odds ratio of 2.6.
Autoimmune diseases are characterized by aberrant immune responses to tissues normally present in the body. Corticosteroids possess anti-inflammatory and immunosuppressive properties; they are therefore widely used to treat a variety of disorders, including autoimmune diseases, transplant recipients, hematological malignancies, asthma, allergic disorders, and nephrotic syndrome. Corticosteroids are the primary treatment for SLE, pemphigus, DM, and PM. However, corticosteroids are also often given as a short-term adjunctive therapy to patients with RA who are waiting for DMARDs to exert their anti-inflammatory effects unless there are life-threatening complications. The results of the present study showed that the total cumulative corticosteroid doses were highest in the DM/PM and SLE patients.
Corticosteroids are well known to predispose patients to AVN [23]. Massardo et al. [24] reported that a daily dose of prednisolone of ≥ 40 mg during the first month of treatment, and methylprednisolone pulse steroid treatment were independent risk factors associated with AVN onset. Mok et al. [25] reported that the cumulative dose of corticosteroids within 4 months was also an important risk factor associated with AVN development. The results of the present study demonstrated that the HRs for AVN in the patients taking medium and high doses of daily corticosteroids were 8.723-fold and 34.034-fold higher, respectively. A total cumulative dose of corticosteroids 0 to 5 g also increased the HR of AVN onset. Conversely, a total cumulative dose of corticosteroids > 5 g did not appear to be an independent risk factor for the development of AVN in the present study.
One reported mechanism underlying AVN onset is intravascular occlusion of the blood vessels, either by thrombotic occlusion (fat or focal clotting due to hypercoagulation) or extraluminal obliteration with increased intraosseous pressure [15,26,27]. Chronic corticosteroid administration promotes fat conversion within the red marrow [28], this is caused by steroid-induced hyperlipidemia or the diversion of mesenchymal stem cells towards an adipocytic lineage [29]. Corticosteroids also reduce femoral head blood flow via their vasoconstrictive effect on the lateral epiphyseal arteries of the femoral head [30], and potentiate vasoconstriction elicited by endothelin-1 [31]. Prolonged and high dose corticosteroid treatment is usually reserved for patients with conditions involving vital organs, such as acute fulminate nephritis, central nervous system diseases, refractory hemolytic anemia or thrombocytopenia in SLE. Therefore, it is difficult to determine whether AVN is directly related to the corticosteroid treatment itself or the severity of the underlying disease, as the majority of patients with active disease are treated with a high dose of corticosteroids. On the other hand, the current study also showed that six patients with SLE who developed AVN had never received corticosteroid treatment. This finding is consistent with a previous study, which found that AVN does occur in SLE patients who have never been exposed to corticosteroids [22,32,33]. In addition, SLE increased the risk of developing AVN compared to other non-SLE autoimmune diseases, such as DM/PM, and other steroid dependent populations, including those with asthma and COPD. These diseases commonly require significant amounts of corticosteroid treatment and this has led to the postulation that additional non-corticosteroid factors specific to the particular disease may account for the progression of AVN. It is likely that additional SLE-specific factors or disease activity may contribute to the development of AVN in SLE patients. Previous studies have reported that AVN was associated with a cushingoid appearance [34], the presence of arthritis [35], vasculitis [7], Raynaud’s phenomenon [7], hematologic diseases [33], gastrointestinal involvement [34] and pleuritis [7,34] in SLE patients. Some studies have proposed that antiphospholipid antibodies are associated with AVN [36], while other studies have not reported this [13]. These risk factors were not calculated in the present study because of a lack of information in the NHIRD.
Besides corticosteroids, the drugs commonly used to treat autoimmune disease include cyclophosphamide and DMARDs, such as azathioprine and hydroxychloroquine. Cyclophosphamide and azathioprine have been reported to be associated with AVN in SLE [35,37]. Cyclophosphamide use is frequently associated with more severe disease. The present study showed that cyclophosphamide and azathioprine use was correlated with the development of AVN, however only in the univariate analysis. It has been documented that hydroxychloroquine use may improve lipid profiles [38,39] and protect against thromboembolisms [39]. However, the protective role of hydroxychloroquine against the development of AVN is controversial [40,41]. Our results demonstrated that hydroxychloroquine use > 0.6 years played a protective role against developing AVN.
Hyperlipidaemia, diabetes mellitus and hypertension are well known side effects of steroid therapy. Dyslipidemia increases the risk of atherosclerosis and arterial thrombosis. Previous studies have indicated that patients with hyperlipidemia are at an increased risk of developing AVN [42]. Some researchers claim that lipid lowering agents, such as statins, decrease the risk of corticosteroid-related AVN [43]. In the current study, neither hyperlipidemia nor diabetes mellitus were found to be independently associated with AVN. Hypertension has been reported to be a significant risk factor for AVN in some studies [34,44,45], while others have found no significant association [7,46]. In the current study, there was no significant association between hypertension and AVN. It is well known that hyperlipidemia and a hypercoagulable state are common in patients with nephrotic syndrome, which may increase their risk of a thromboembolism. Meanwhile, patients with renal involvement complicated by nephrotic syndrome, chronic kidney disease or end-stage renal disease have a higher disease activity and are more likely to need a higher steroid dose. These clinical factors interact with others and contribute to the development of AVN. The majority of previous studies have demonstrated that renal involvement was a risk factor for AVN onset in SLE patients [47]. In the current study, proteinuria and nephrotic syndrome were significantly associated with AVN development, however only in the univariate analysis; they did not show a significant association in the multivariate analysis.
Most published studies on autoimmune disease-related AVN are based on single-institution investigations. To the best of our knowledge, the present study is the first large-scale nationwide population-based cohort study of AVN occurrence in patients with autoimmune diseases. The major strength of the current study is the fact that the identification of autoimmune diseases is highly reliable, due to the NHI assessment of catastrophic illness claims and its population-based design. However, there were certain limitations. First, asymptomatic AVN was not identified as part of the study. Second, radiology reports for AVN, serological data and major organ involvement of the patient’s underlying disease were unavailable from the NHIRD. Another limitation may be that some clinical symptoms, which are suspected of being risk factors associated with AVN development [48] were not included in the analysis. Therefore, SLE disease activity index as a risk factor for AVN development in SLE patients was not available in the current study. Personal information, including family history, trauma, lifestyle, smoking, and body weight were also not available.
Patients with SLE had the highest risk of AVN in this study. Male sex, alcoholism, a high mean daily corticosteroid exposure over 7.5 mg and a total cumulative dose of corticosteroid between 0 and 5 g were independently associated with AVN development in the autoimmune patients. Hydroxychloroquine use > 0.6 years decreased the risk of AVN in the rheumatic patients. Clinicians should monitor high-risk patients regularly to enable the diagnosis of AVN in early stages using high sensitive techniques, such as MRI. Further prospective studies are needed to clarify the factors which may contribute to the development of AVN in autoimmune patients.
KEY MESSAGE
1. Male sex, alcoholism, systemic lupus erythematosus, mean daily corticosteroid > 7.5 mg and a total cumulative dose of corticosteroid between 0 g and 5 g were the key predictors for the development of avascular necrosis (AVN) in autoimmune patients.
2. The use of hydroxychloroquine > 0.6 years played a protective role against developing AVN.
Supplementary Information
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported by a grant from Taipei Veterans General Hospital (V106C-124) in Taiwan.