Clinical efficacy of adjuvant chemotherapy in stage IB (< 4 cm) non-small cell lung cancer patients with high-risk factors
Article information

Abstract
Background/Aims
Adjuvant chemotherapy is the standard of care for resected stage II–IIIA non-small cell lung cancer (NCSLC). The efficacy of adjuvant chemotherapy in stage IB (< 4 cm) NSCLC with high-risk factors is controversial.
Methods
This retrospective multicenter study included 285 stage IB NSCLC patients with high-risk factors according to the 8th edition tumor, node, metastasis (TNM) classification from four academic hospitals. High-risk factors included visceral pleural invasion, vascular invasion, lymphatic invasion, lung neuroendocrine tumors, and micropapillary histology patterns.
Results
Of the 285 patients, 127 (44.6%) were included in the adjuvant chemotherapy group and 158 (55.4%) were included in the non-adjuvant chemotherapy group. The median follow-up was 41.5 months. Patients in the adjuvant chemotherapy group had a significantly reduced recurrence rate and risk of mortality than those in the non-adjuvant chemotherapy group (hazards ratio, 0.408; 95% confidence interval, 0.221 to 0.754; p = 0.004 and hazards ratio, 0.176; 95% confidence interval, 0.057 to 0.546; p = 0.003, respectively). Adjuvant chemotherapy should be particularly considered for the high-risk factors such as visceral pleural involvement or vascular invasion. Based on the subgroup analysis, adjuvant chemotherapy should be considered when visceral pleural involvement is present, even if the tumor size is < 3 cm.
Conclusions
Adjuvant chemotherapy may be useful for patients with stage IB NSCLC with high-risk factors and is more relevant for patients with visceral pleural involvement or vascular invasion.

INTRODUCTION
Treatment of non-small-cell lung cancer (NSCLC) is constantly evolving with the development of targeted therapy and immunotherapy [1]. Surgical resection is the standard of treatment of early-stage NSCLC; however, the recurrence rate is 20% to 50% in early-stage NSCLC after complete resection, and most would eventually die due to the disease [2]. Adjuvant chemotherapy is essential for patients at a high-risk of recurrence.
Several clinical trials have been conducted on the efficacy and safety of adjuvant chemotherapy in early-stage NSCLC; however, no trials have assessed its efficacy and safety in stage IB NSCLC with high-risk factors [3,4]. Most previous clinical trials on adjuvant chemotherapy have used the tumor, node, metastasis (TNM) classification 7th edition. In the 8th edition of TNM staging for lung cancer, the T2a classification was revised from tumor measuring 5 cm to tumor measuring 4 cm. Thus, clinical studies on stage IB (< 4 cm) patients according to the 8th edition are needed.
The efficacy of adjuvant chemotherapy in stage IB NSCLC with high-risk factors is unclear [5–7]. The National Comprehensive Cancer Network (NCCN) guidelines state that high-risk factors alone should not be an indication for adjuvant chemotherapy and may be considered when determining the primary treatment with adjuvant chemotherapy. However, several factors are considered high-risk factors, and it is unknown whether there is a risk difference between them. Therefore, this is a currently a debated issue, and there is a lack of information regarding the need for adjuvant chemotherapy in such patients. Hence, we aimed to analyze the clinical effects of adjuvant chemotherapy in stage IB (< 4 cm) NSCLC with high-risk factors under various conditions.
METHODS
Study design and participants
We retrospectively reviewed the medical records from four academic hospitals and found that 285 pathologic T2aN0M0 stage IB (< 4 cm) NSCLC patients who had high-risk factors. We included patients who were admitted from January 2008 to May 2018 (Fig. 1). All patients underwent lobectomy and complete lymph node dissection, and none of them underwent pneumonectomy, bilobectomy, segmentectomy, or wedge resection. All patients underwent R0 resection, and there was no evidence of cancer in the lymph node (N0). Pathologic stages were based on the TNM classification of the International Union Against Cancer, 8th edition. Patients who received neoadjuvant therapy, radiotherapy, or non-platinum-based adjuvant chemotherapy were excluded.

Flowchart of analyzed stage IB non-small cell lung cancer patients with high-risk factors. NCSLC, non-small cell lung cancer.
The NCCN guidelines have mentioned six high-risk factors. Of the six high-risk factors, we included those of stage Ib NSCLC, so we excluded those of “in tumor size > 4 cm.” And, patients who had undergone wedge resection and those who had an unknown lymph node status (Nx) were also excluded as they limited accurate stage evaluation. Since a micropapillary pattern is a pathological predictor of recurrence, it was considered a high-risk factor in this study [8–10]. Furthermore, previous studies have shown that lymphatic invasion is associated with recurrence [11,12]. Therefore, we included the following five high-risk factors: visceral pleural involvement, micropapillary pattern, lymphatic invasion, vascular invasion, and lung neuroendocrine tumors. Chest computed tomography (CT) were performed every 3 to 6 months for the first 2 years after diagnosis and thereafter every 6 months for 5 years or until death. When recurrences were suspected, a chest CT and/or positron emission tomography (PET) was performed regardless of the timing. Comorbidities and smoking history were recorded at the time of surgery.
Adjuvant chemotherapy was initiated within 2 months of surgery. The following five platinum-based regimens were used: paclitaxel-carboplatin (48.8%), paclitaxel-cisplatin (14.2%), vinorelbine-cisplatin (22.8%), vinorelbine-carboplatin (11.0%), and pemetrexed-cisplatin (3.1%). Only patients who completed four cycles were included in the study. The cycles were given every 3 weeks, but the term of cycle and dose were adjusted according to the patient’s general condition and side effects.
Our study was approved by the Institutional Review Board of all four academic hospitals (Korea University Guro Hospital IRB Number [2018GR0244], Korea University Anam Hospital IRB Number [2019AN0350], Catholic University Hospital IRB Number [SC20RID10014], and Hanyang University Hospital IRB Number [HYUH 2019-03-008]). The need for patient consent was waived because of the retrospective study design.
Statistical analysis
Data were analyzed using SPSS for Windows version 20 (IBM Co., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as number and percentage. We divided the patients into two groups depending on the use of adjuvant chemotherapy (adjuvant chemotherapy group and no adjuvant chemotherapy group [control group]). Continuous variables were compared using the Student’s t test, while categorical variables were compared using the chi-square or Fisher’s exact test. Fisher’s exact test was used when the expected number of events was < 5.
Recurrence-free survival (RFS) was calculated from the date of surgery to the date of the first recurrence evaluated by chest CT or PET/CT. Overall survival (OS) was calculated from the date of surgery to the date of death from any cause. The Kaplan-Meier method and log-rank test were used for analyzing RFS and OS. The multivariate Cox proportional hazards model analysis was performed for analyzing hazard ratio (HR). The multivariate analysis was performed using a backward elimination procedure for variables with p < 0.2 in the univariate analysis. A p < 0.05 was considered statistically significant.
We also analyzed the HR of adjuvant chemotherapy in every subgroup. Subgroup analysis was performed only in groups with at least 200 patients. Multivariate analysis was performed using the Cox proportional hazards model in the subgroup analysis. Cox proportional hazards model was also conducted using a backward elimination procedure for variables with p < 0.2 in the univariate analysis.
RESULTS
Baseline characteristics
Of the 285 patients, 127 (44.6%) were included in the adjuvant chemotherapy group and 158 (55.4%) were included in the control group. The mean and median follow-up duration were 40.2 ± 18.1 and 41.5 months, respectively. There were no differences between the groups, except age, visceral pleural involvement, and lymphatic invasion (Table 1). Patients in the adjuvant chemotherapy group were younger than those in the control group (p < 0.001). The proportion of men and women in both groups was similar. Of the 285 patients, 61% patients were non-smokers and < 10% patients were current smokers. Further, 83% (n = 237) patients had adenocarcinoma, and ‘others’ included NSCLC not otherwise specified and adeno-squamous carcinoma. In addition, 28% (n = 81) patients had tumors measuring > 3 cm in diameter. Visceral pleural involvement was the most common high-risk factor in both groups, and visceral pleural involvement and lymphatic invasion were more frequent in the adjuvant chemotherapy group than in the control group (p = 0.004, p = 0.047, respectively).

Baseline characteristics
Recurrence-free survival
Recurrence was observed in 11.8% (15/127) and 24.1% (38/158) patients in the adjuvant chemotherapy and the control groups, respectively. In the Kaplan-Meier survival curves and log-rank test, the 5-year RFS was 81.8% in the adjuvant chemotherapy group and 66.8% in the control group (p = 0.008) (Fig. 2A).
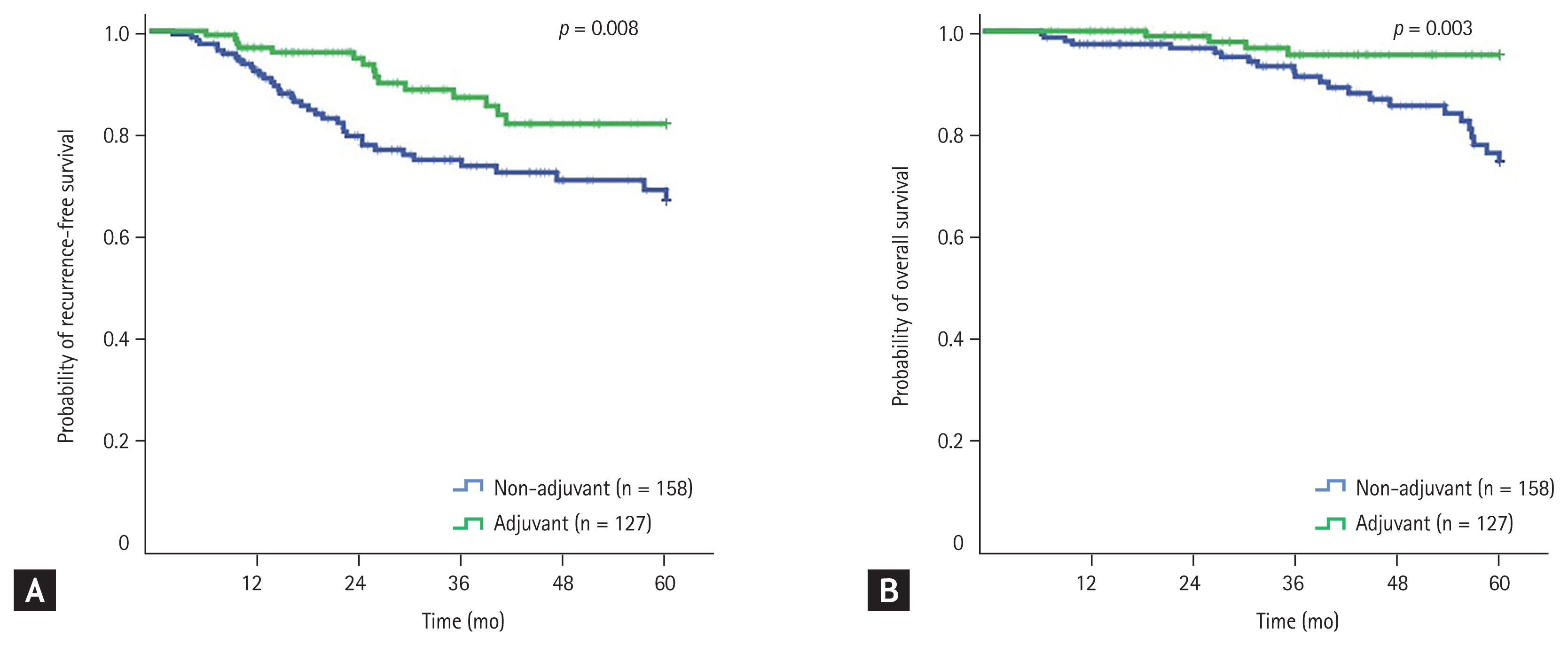
(A) Kaplan-Meier curve for recurrence-free survival. (B) Kaplan-Meier curve for overall survival.
In the univariate analysis, the adjuvant chemotherapy group and female patients had a lower risk of recurrence than the control group and male patients (p = 0.010, p = 0.045, respectively) (Table 2). In the multivariate analysis, the adjuvant chemotherapy group had a lower risk of recurrence than the control group (HR, 0.408; 95% confidence interval [CI], 0.221 to 0.754; p = 0.004). Among the other parameters, vascular invasion was associated with a higher risk of recurrence (HR, 2.561; 95% CI, 1.171 to 5.601; p = 0.018).
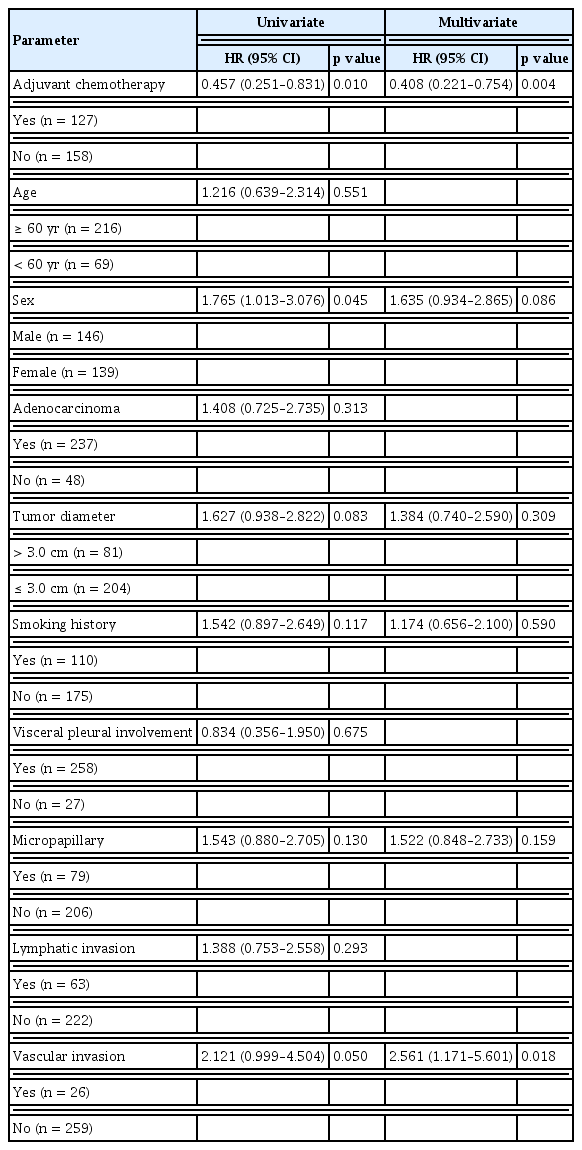
Risk factors for recurrence-free survival
Overall survival
The mortality rate was 3.1% (4/127) and 14.6% (23/158) in the adjuvant chemotherapy and control groups, respectively. In the Kaplan-Meier survival curves and log-rank test, the 5-year RFS was 95.4% and 74.6% in the adjuvant chemotherapy and control groups, respectively (p = 0.003) (Fig. 2B).
In the univariate analysis, the risk of death was lower in the adjuvant chemotherapy group, female patients, non-adenocarcinoma, and non-smokers (p = 0.007, p = 0.002, p = 0.022, p < 0.001, respectively) (Table 3). In the multivariate analysis, the risk of death was lower in the adjuvant chemotherapy group than in the control group (HR, 0.176; 95% CI, 0.057 to 0.546; p = 0.003). Among the other parameters, male patients, smoking history and vascular invasion increased the risk of death (p = 0.007, p < 0.001, p = 0.006, respectively).

Risk factors for overall survival
Subgroup analysis
Visceral pleural involvement, adenocarcinoma, tumor size ≤ 3 cm, and visceral pleural involvement plus tumor size ≤ 3 cm subgroups had > 200 patients (Table 4). In all the four subgroups, the risk of recurrence and death was lower in the adjuvant chemotherapy than in the control group.

Subgroup analysis through multivariate analysis by Cox hazard model
DISCUSSION
Our study analyzed the efficacy of adjuvant chemotherapy in stage IB NSCLC patients with high-risk factors based on the TNM 8th edition. We showed that adjuvant chemotherapy is beneficial in such patient group and significantly reduced the risk of recurrence and mortality. Among the various high-risk factors, adjuvant chemotherapy should be particularly considered in the presence of visceral pleural involvement or vascular invasion. Based on the subgroup analyses, adjuvant chemotherapy should be considered when visceral pleural involvement is present, even if the tumor size is < 3 cm.
Various factors are considered high-risk factors in stage IB NSCLC [13]. The NCCN guidelines, in particular, classify lung neuroendocrine tumors, vascular invasion, wedge resection, tumor size > 4 cm, and visceral pleural involvement as high-risk factors. Other studies have suggested that lymphatic invasion, micropapillary, and solid patterns as high-risk factors [9,12,14]. Pathohistological patterns have been shown to influence the sensitivity of chemotherapy and prognosis of adenocarcinomas [8,10]. In our study, only the presence of micropapillary patterns, and not the solid patterns, were analyzed. However, our study did not prove that the micropapillary pattern was an independent risk factor. However, as these were not quantified, it was difficult to accurately analysis the role of micropapillary patterns in our patients. Further work including quantitative analyses and the inclusion of additional pathological patterns is required.
Tumor size is a well-known prognostic factor of cancer [15,16]. Also, visceral pleural involvement has been considered very important among the various high-risk factors [17]. In our analysis, adjuvant chemotherapy was useful even if the tumor size was < 3 cm. Adjuvant chemotherapy should be actively considered when there is visceral pleural involvement, even if the tumor size were small.
The use of adjuvant chemotherapy in resected NSCLC has already been demonstrated in many randomized clinical trials (RCTs) [18,19]. However, most RCTs have used the 7th edition TNM classification and not the current 8th edition. Also, its usefulness in stage IB NSCLC with high-risk factors has yet been studied. The NCCN guidelines also state that high-risk factors are not an absolute indication for adjuvant chemotherapy in stage IB. This raises confusion in clinical practice, as the use of adjuvant chemotherapy relies on the clinician’s judgment. Previous RCTs have studied the practice of platinum-based adjuvant chemotherapy in stage IB NSCLC based on the TNM 7th edition. In the Cancer and Leukemia Group B 9633 study on paclitaxel plus carboplatin, adjuvant chemotherapy was helpful for tumors measuring > 4 cm, but not for those measuring < 4 cm (HR, 1.12; 90% CI, 0.75 to 1.07; p = 0.32) [4]. However, when re-analyzing the patient population based on the TNM 8th edition, this study included only a small number of patients with stage IB NSCLC and did not analyze high-risk factors.
The effect of adjuvant chemotherapy on completely resected stage IB–IIIA NSCLCs was demonstrated in the Adjuvant Navelbine International Trialist Association (ANITA) trial using vinorelbine plus cisplatin [3]. However, adjuvant chemotherapy was found to be useful mainly in patients with lymph node metastasis. In addition, the vinorelbine plus cisplatin regimen was useful mainly in adenocarcinomas, and this study emphasized the importance of regimen selection according to tumor cell type [20]. The study included 301 stage IB NSCLC patients using the 7th edition TNM classification, but did not prove efficacy of adjuvant chemotherapy (HR, 1.10; 95% CI, 0.76 to 1.57), and also did not analyze high-risk factors.
A retrospective study showed the usefulness of adjuvant chemotherapy in stage IB NSCLC (HR, 0.428; 95% CI, 0.184 to 0.998; p = 0.049) [21]; however, it included patients with tumor sizes ≥ 4 cm based on TNM 7th edition or without high-risk factors. Additionally, pleural and lymphovascular invasion were analyzed but no statistically significant results were found. Large-scale studies targeting only patients with stage IB NSCLC with high-risk factors are rare.
Our study has several limitations. First, this was a retrospective study. There were differences in age and presence of high-risk factors between the two groups. In addition, we did not analyze the Eastern Cooperative Oncology Group performance for all patients; only those in the adjuvant chemotherapy group were assessed. The cause of death was also not classified, which may have led to better OS p values. The difference in OS may also be due to differences in age and general physical condition of patients. However, the control group had fewer risk factors than the adjuvant chemotherapy group, and demonstrated prolonged RFS and OS. Therefore, even if the baseline characteristic differed between the two groups, our results seemed meaningful. Second, the toxicity and dose intensity of chemotherapy were not evaluated. Only one hospital evaluated the toxicity; and of the 45 patients, grade 3 to 4 neutropenia was present in 75.6%, and grade 3 to 4 anemia or thrombocytopenia was not present. Hospitalization due to neutropenic fever occurred in 24.4% of patients, and there was no chemotherapy-related death. The patient data collection period of our paper was about 10 years (2008 to 2018). Data on dose intensity of some patients could not be accurately found. Third, quantitative evaluation of micropapillary patterns was not possible, and only their presence was assessed. Fourth, morphology patterns such as solid, acinar, papillary, and lepidic patterns could not be statistically analyzed because this was only evaluated in two hospitals. Fifth, we used only regimens favored for adenocarcinoma, which were not sensitive to squamous carcinoma or neuroendocrine carcinoma; thus, their evaluation was limited.
In conclusion, although this was a retrospective study, it was large-scaled and multi-centered involving 285 patients. We have shown that adjuvant chemotherapy prolongs RFS and OS in stage IB NSCLC with high-risk factors. Among the various high-risk factors, adjuvant chemotherapy should be particularly considered in the presence of visceral pleural involvement or vascular invasion. Further research with large-scale randomized controlled trials is needed.
KEY MESSAGE
1. Efficacy of adjuvant chemotherapy in stage IB non-small cell lung cancer (NCSLC) with high-risk factors remains controversial.
2. Lung neuroendocrine tumors, vascular or lymphatic invasion, micropapillary and solid patterns, and visceral pleural involvement are high-risk factors.
3. Platinum-based doublet adjuvant therapy increased the recurrence-free and overall survival of stage IB NSCLC patients with high-risk factors.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.