Current findings of kidney biopsy including nephropathy associated with hypertension and diabetes mellitus in Korea
Article information
 , the Korean GlomeruloNEphritis sTudy (KoGNET) Group
, the Korean GlomeruloNEphritis sTudy (KoGNET) GroupAbstract
Background/Aims
This study aimed to investigate long-term temporal trends and outcomes of biopsy-proven kidney diseases in a multicenter kidney biopsy cohort, focusing on hypertension and diabetes, the leading causes of end-stage kidney disease (ESKD).
Methods
The study included a total of 21,426 patients who underwent kidney biopsy from 1979 to 2018 in 18 hospitals in Korea. We selected subgroups of adults with diabetes (n = 2,813) or clinically presumed hypertensive nephrosclerosis (HT-N, n = 2,917). Clinical, demographic, and laboratory data were collected in conjunction with pathologic findings. The prevalence of pathologically confirmed kidney diseases over time and their associations with clinical outcomes were evaluated.
Results
The prevalence of biopsy-proven diabetic nephropathy (DN) has increased significantly from 2.5% to 6.0% in the total cohort in the recent 30 years with an increase in the prevalence of diabetes. Approximately 68% of total diabetic patients had non-diabetic renal disease (NDRD); the proportion was retained since 2000s. DN showed a significantly higher risk of ESKD than NDRD (hazard ratio [HR], 1.59; 95% confidence interval [CI], 1.35 to 1.88). The prevalence of biopsy-proven HT-N remained < 2% in the total cohort for several decades. There was no difference in risks of ESKD between patients with or without biopsy-proven HT-N (HR, 0.93; 95% CI, 0.54 to 1.59).
Conclusions
In recent decades, the prevalence of diabetes and DN has significantly increased in the kidney biopsy cohort, showing an increased risk of ESKD. Despite the large numbers of patients meeting the clinical criteria of HT-N, most of those were diagnosed with pathologic diagnoses other than HT-N.
INTRODUCTION
Kidney biopsy has remained a golden standard for the diagnosis of renal parenchymal diseases despite recent efforts to develop non-invasive diagnostic approaches [1,2]. The usefulness of kidney biopsy includes providing evidence for diagnosis, prognosis, and response to therapy of different kidney diseases [3]. In particular, kidney biopsy registries encompass many kinds of kidney diseases and can display their epidemiology and clinicopathologic associations [4]. Previous kidney biopsy cohort studies demonstrated different prevalence of several types of glomerulonephritis (GN) according to ethnicities and geographic regions [5]. Nevertheless, the majority of these studies were single-center studies with a small number of patients and a short follow-up period [6-8]. As a result, knowledge of temporal trends in the diagnosis of biopsy-proven kidney diseases is insufficient and inconsistent between studies. For several decades, there have been substantial changes in comorbidities such as diabetes, obesity, and hypertension, medications, and lifestyles, all of which could affect the prevalence of biopsy-proven kidney diseases. The global prevalence of diabetes increased dramatically from 4.3% in 1980 to 9.0% in 2014 [9], and in a systemic review, the recent prevalence of hypertension was reported as high as 26.4% worldwide [10]. Hypertension and diabetes are well known as two of the leading etiologies of end-stage kidney disease (ESKD) [11]. Although histological findings of diabetic nephropathy (DN) and hypertensive nephrosclerosis (HT-N) have been described in detail and classified in previous studies [12-14], the cause of chronic kidney disease (CKD) is clinically diagnosed without kidney biopsy in many diabetic and hypertensive patients. Furthermore, a considerable number of patients with diabetes or hypertension were found to have pathologic diagnoses other than DN or HT-N in kidney biopsy [15,16]. Therefore, hypertension- and diabetes-related ESKD may be overestimated, and the actual contributions of diabetes and hypertension to CKD could be biased. Although kidney biopsy has not been performed routinely to confirm HT-N or DN, kidney biopsy is now more frequently performed in diabetic and hypertensive patients. Therefore, in this study, we aimed to investigate the long-term temporal trends and outcomes of pathologically diagnosed kidney diseases in multicenter kidney biopsy registries, especially including kidney diseases related to diabetes and hypertension.
METHODS
Study population and data collection
We initially screened 21,617 patients with native kidney biopsy between 1979 and 2018 from 18 hospitals throughout Korea, retrospectively. First, in a total of 21,426 patients after excluding 191 patients with renal cancer or tumor, we investigated clinical characteristics and overall trends of biopsy-confirmed kidney diseases (Supplementary Fig. 1). Second, we selected two subgroups of adult patients with diabetes (n = 2,813) or clinically presumed HT-N (n = 2,917) after excluding 976 children aged < 18 years and 237 patients with missing age at kidney biopsy to explore the pathologic diagnoses and their associations with clinical outcomes in each group. Kidney biopsy was performed with ultrasonography-guided percutaneous biopsy, and the results were interpreted by a renal pathologist in each hospital. The clinical data at the time of biopsy and the last follow-up were queried into the hospital information system (HIS) with the primary keys of the patients’ identification number and date of kidney biopsy at each hospital. All 18 centers have an HIS, and data were scanned and saved before launching the HIS. Five trained research nurses had recorded the predefined parameters on the template database file based on the queried information, and one of nephrologists of this research had cleansed the data for analysis. Data of final outcomes, incidences of ESKD and death, were gathered from each hospital’s HIS, the ESKD registry of the Korean Society of Nephrology which was started in 1980, and the Statistics of Korea, and were merged based on the national identification number. The follow-up duration was 110.6 ± 105.0 months for ESKD and 119.4 ± 106.6 months for death.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital (B-1707/408-106) and the other 17 centers. Written consent was waived by the IRB because of the retrospective nature of the study.
Definitions of covariates
Diabetes mellitus was defined as random glucose level ≥ 200 mg/dL, hemoglobin A1c ≥ 6.5%, taking antidiabetic medication, or diagnosed by the physician. Hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, taking antihypertensive medication to control blood pressure, or diagnosed by the physician. The estimated glomerular filtration rate (eGFR) was calculated using the original Modification of Diet in Renal Disease equation for adults and the height-independent equation for children [17]. Nephrotic syndrome was defined as urine protein-to-creatinine ratio (UPCR) ≥ 3.5 g/g and serum albumin < 3.0 g/dL. For the comparison between clinical and pathologic entity of HT-N, we used the following clinical diagnostic criteria of HT-N: (1) presence of hypertension, (2) no diabetes, (3) no evidence of vasculitis and lupus nephritis (LN), (4) low-grade proteinuria defined as UPCR < 2.0 g/g, which was similar to those in previous studies [16,18]. Clinically diagnosed HT-N patients were divided into three groups: biopsy-proven HT-N without other pathologic diagnoses, pathologic diagnoses other than HT-N (non-HT-N), and biopsy-proven HT-N combined with other pathologic diagnoses (mixed). The pathologic diagnosis of diabetic patients was grouped into pure DN, non-diabetic renal disease (NDRD), and NDRD superimposed on DN (NDRD/DN).
Pathologic diagnosis
We primarily adopted the findings and diagnosis by the pathologist in each hospital. We enrolled all pathologic diagnoses to describe the overall trends based on the results of renal biopsies, including data of light microscopic examination, immunofluorescent microscopic examination, and electron microscopic examination. Among 21,426 patients, 777 have two pathologic diagnoses; therefore, we analyzed a total of 22,203 diagnoses. All pathologic diagnoses are shown in Table 1. We defined primary GN as IgA nephropathy (IGAN), minimal change disease (MCD), membranous nephropathy (MN), focal segmental glomerulosclerosis (FSGS), membranoproliferative glomerulonephritis (MPGN), and C3 glomerulopathy (C3G) regardless of the pathogenesis.
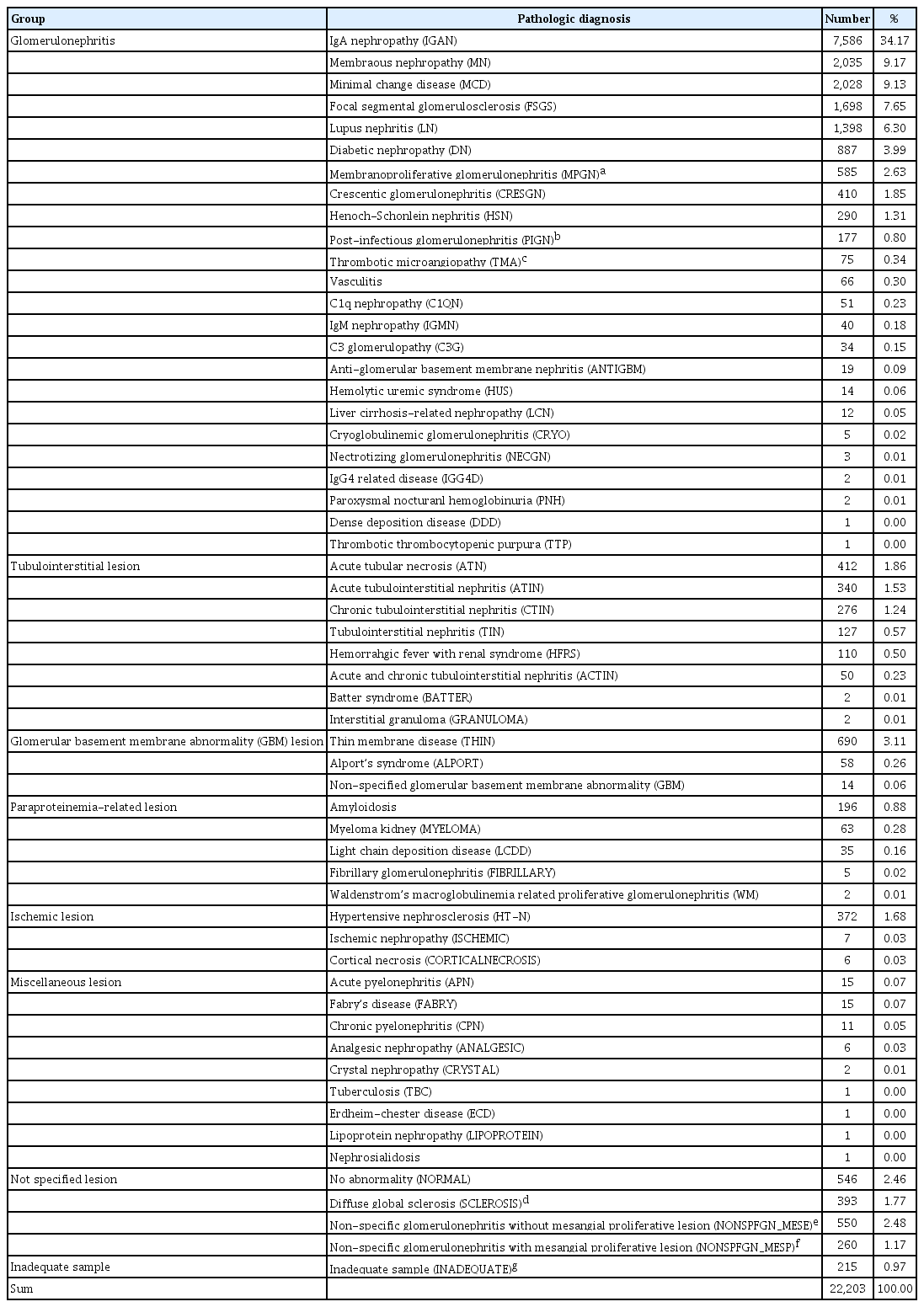
Pathologic diagnoses of 21,426 patients with native kidney biopsy.
Statistical analysis
All analyses were performed using IBM SPSS Statistics version 25.0 (IBM Co., Armonk, NY, USA) and R software version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were reported as mean ± standard deviation for continuous variables or frequency for categorical variables. Differences in continuous variables were analyzed by t test and one-way analysis of variance (ANOVA) test and, in categorical variables, by chi-square test. Multiple comparisons were performed using Tukey-Kramer post hoc test. The independent risk factors to estimate the final outcomes were assessed by Cox hazard proportional model adjusted for related variables. The proportion of missingness of variables is shown in Supplementary Table 1, and multiple imputation by chained equation with classifications and regression trees was used for handling missing data. Complete case analyses were also performed as sensitivity analyses. Clinical characteristics and outcomes of patients with biopsy-proven HT-N were compared with those of patients without HT-N using propensity score matching for related covariates. The standardized mean difference was estimated to examine the balance of covariate distribution between the matched cohorts. Two-sided p values were reported with 0.05 taken as the level of statistical significance.
RESULTS
Overall trends of pathologic diagnosis during 40 years
Overall temporal trends in clinical characteristics of the enrolled participants are shown in Table 2. Among 21,426 patients, 11,565 (54.0%) were men, 976 (4.6%) were children aged < 18 years, and the mean age was 42.1 ± 17.7 years. There were 10,659 (53.0%) hypertensive patients and 2,813 (14.0%) diabetic patients. Nearly one-fourth of patients had eGFR < 45 mL/min/1.73 m2 at the time of biopsy. The average incidence of kidney biopsy during 40 years was 11.59 per million population/year. The most frequent pathologic diagnosis was IGAN (34.17%, n = 7,586), followed by MN (9.17%, n = 2,035), MCD (9.13%, n = 2,028), FSGS (7.65%, n = 1,698), LN (6.30%, n = 1,398), DN (3.99%, n = 887), and MPGN and C3G (2.79%, n = 619); therefore, the prevalence of primary GN was 62.90%. Over the follow-up period, the frequency of biopsy in older patients gradually increased, and the frequency of biopsy in diabetic patients increased rapidly from 2.0% in 1979 to 1989 to 17.9% in 2010 to 2018. The mean eGFR of the participants was higher after 2000 than that in the previous study period. Nephrotic syndrome was found in approximately 17.5% of patients with kidney biopsy. Proteinuria levels and the proportion of nephrotic syndrome at the time of biopsy decreased after 2000.

Temporal trends in patient characteristics and the incidence of kidney biopsy
The prevalence of IGAN increased from 19.9% (1979 to 1989) to 38.0% (2000 to 2009) and then stabilized at approximately 35% (Fig. 1A). The prevalence of MCD, MN, and FSGS barely changed since 1990. However, the prevalence of MPGN decreased from 4.7% to 5.7% (1979 to 1999) to 2.3% (2010 to 2018). The prevalence of LN also decreased from 13.6% (1990 to 1999) to 4.9% (2010 to 2018). IGAN was the most frequent GN in all age groups, except in patients aged ≥ 70 years, among whom MN was the most frequent GN (Fig. 1B). MCD was the second most frequent pathologic diagnosis in patients aged < 20 years and showed a second peak of incidence in patients in their sixties. The frequency of MN was increased in patients aged > 40 years and was the most frequent diagnosis in patients aged ≥ 70 years. Crescentic GN was among the top five GN in patients aged ≥ 70 years. The most frequent primary GN with nephrotic range proteinuria was MN (19.2%), followed by MCD (17.6%), IGAN (15.6%), FSGS (9.9%), and DN (7.8%) (Fig. 1C).
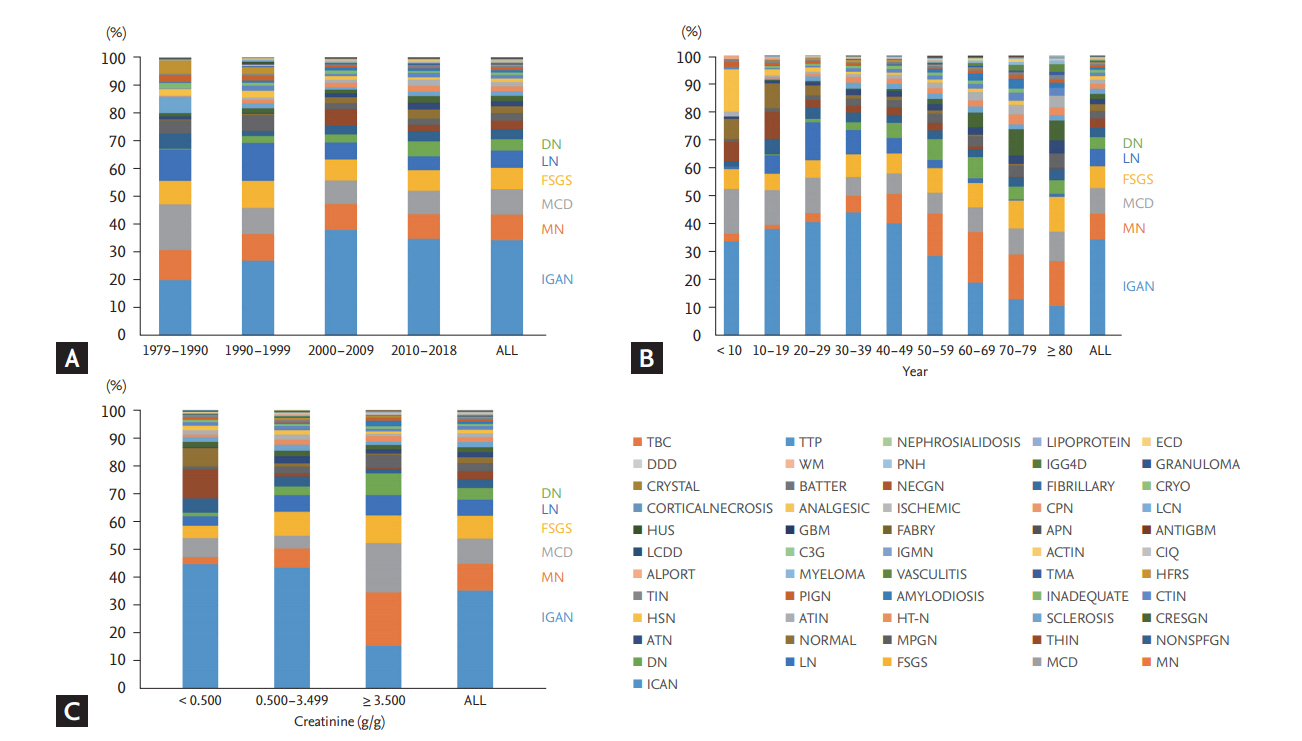
Trends of pathologic diagnosis in kidney biopsy during the past 40 years in Korea. (A) Pathologic diagnosis according to periods. (B) Pathologic diagnosis according to age at kidney biopsy. (C) Pathologic diagnosis according to urine protein-to-creatinine ratio. DN, diabetic nephropathy; LN, lupus nephritis; FSGS, focal segmental glomerulosclerosis; MCD, minimal change disease; MN, membranous nephropathy; IGAN, IgA nephropathy; TBC, tuberculosis; TTP, thrombotic thrombocytopenic purpura; ECD, Erdheim-chester disease; DDD, dense deposition disease; WM, Waldenstrom’s macroglobulinemia; PNH, paroxysmal nocturanl hemoglobinuria; IGG4D, IgG4 related disease; NECGN, nectrotizing glomerulonephritis; CRYO, cryoglobulinemic glomerulonephritis; CPN, chronic pyelonephritis; LCN, liver cirrhosis-related nephropathy; HUS, hemolytic uremic syndrome; GBM, glomerular basement membrane; APN, acute pyelonephritis; LCDD, light chain deposition disease; C3G, C3 glomerulopathy; IGMN, IgM nephropathy; TMA, thrombotic microangiopathy; HFRS, hemorrahgic fever with renal syndrome; TIN, tubulointerstitial nephritis; PIGN, post-infectious glomerulonephritis; CTIN, chronic tubulointerstitial nephritis; HSN, Henoch-Schonlein nephritis; ATIN, acute tubulointerstitial nephritis; HT-N, hypertensive nephrosclerosis; CRESGN, crescentic glomerulonephritis; ATN, acute tubular necrosis; MPGN, membranoproliferative glomerulonephritis; THIN, thin membrane disease; NONSPFGN, non-specific glomerulonephritis.
Pathology and prognosis of kidney diseases in diabetic patients
Among 2,813 diabetic patients, DN and NDRD were present in 881 (31.3%) and 1,932 (68.7%) patients, respectively. Among DN patients, pure DN was detected in 790 (28.1%) patients and NDRD/DN was found in 91 (3.2%) patients. The most common NDRD was IGAN (23.1%), followed by MN (14.5%), FSGS (11.0%), MCD (7.5%), and MPGN (4.2%) (Supplementary Table 2). Frequencies of MPGN and FSGS were relatively higher in NDRD patients than in non-diabetic patients considering age at kidney biopsy. In patients with NDRD/DN, renal pathologies other than DN were IGAN (37.4%), acute tubular necrosis (8.8%), FSGS (8.8%), tubulointerstitial nephritis (5.5%), and MPGN (5.5%). Since 1990s, as the number of diabetic patients who underwent kidney biopsy continuously increased, the proportion of biopsy-proven DN also increased by over 2-fold, i.e., from 2.5% to 3.0% (1990 to 2009) to 6.0% (2015 to 2018) (Fig. 2A). The proportion of patients with DN among those with diabetes who underwent kidney biopsy was higher in 1990s than in 2000s (44.8% vs. 26.3%, p = 0.001 by chi-square test) (Fig. 2B), but no significant change has been observed since 2000. The prevalence of NDRD has been more than double that of DN since 2000s. The clinical characteristics of diabetic patients according to the presence of DN are shown in Table 3. Pure DN patients showed higher blood pressure and more severe renal impairment and proteinuria. Pure DN was associated with 1.59-fold higher risks (95% confidence interval [CI], 1.35 to 1.88) of incident ESKD than NDRD (p < 0.001) (Table 4), which was consistent with the results of the complete case analyses (Supplementary Table 3). However, the risk of mortality was not different between pure DN and NDRD. Other risk factors of incident ESKD in diabetic patients were older age, male sex, hypertension, SBP, eGFR, serum albumin, and hemoglobin (Supplementary Table 4). The appropriate level of SBP was < 130 mmHg on the day after admission for kidney biopsy.

Temporal trends of renal pathologic diagnosis in diabetic patients. (A) Annual proportions of pure diabetic nephropathy (DN), non-diabetic renal disease (NDRD)/DN, NDRD in the total study cohort. (B) Annual proportions of DN (pure DN plus NDRD/DN) and other pathologic diagnoses in total diabetic patients. FSGS, focal segmental glomerulosclerosis; IGAN, IgA nephropathy; MCD, minimal change disease; MN, membranous nephropathy; MPGN, membranoproliferative glomerulonephritis.

Clinical characteristics of diabetic patients with kidney biopsy
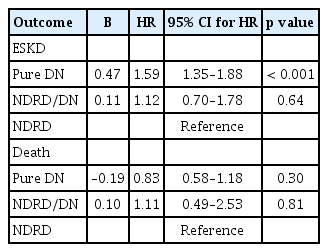
Associations between biopsy-proven diagnosis and clinical outcomes in diabetic patients
Pathology and prognosis of kidney diseases in patients with clinical HT-N
First, we examined the correlation between HT-N diagnosed by clinical criteria and biopsy-proven HT-N (Supplementary Table 5). All patients with biopsy-proven HT-N had hypertension, but only 5% of the patients who met the clinical criteria including low-grade proteinuria (criteria 3) were pathologically diagnosed with HT-N. Moreover, most of the biopsy-proven HT-N patients did not meet the clinical criteria; sensitivities were as low as 39%. In a total of 2,927 adult patients who met the clinical criteria, there were 142 subjects with biopsy-proven HT-N and 2,785 with non-HT-N (Supplementary Table 6). Of the 142 patients with biopsy-proven HT-N, 103 (72.5%) had only biopsy-proven HT-N with no other pathologic diagnosis. The most common biopsy-proven kidney disease in non-HT-N patients was IGAN (54.4%), followed by FSGS (10.0%), MN (5.0%), and MCD (5.0%); IGAN and FSGS were found more frequently in clinical HT-N patients than in the total cohort.
The proportion of clinical HT-N has ranged from 5% to 20% of the total cohort during the study period and showed an increasing trend after the 2000s with an increase in an annual biopsy rate (Fig. 3A). Biopsy-proven HT-N has been observed since 1990s when the prevalence of hypertension in Korea increased obviously than before. Nevertheless, the prevalence of biopsy-proven HT-N remained quite low (approximately 5% of clinical HT-N patients and less than 2% of the total cohort) until the recent years. A majority of clinical HT-N patients were diagnosed with non-HT-N based on the kidney biopsy. Of these patients, distributions of specific kidney diseases over time were similar to those in the total cohort; an increase in IGAN and a decrease in MPGN incidence were found (Fig. 3B).
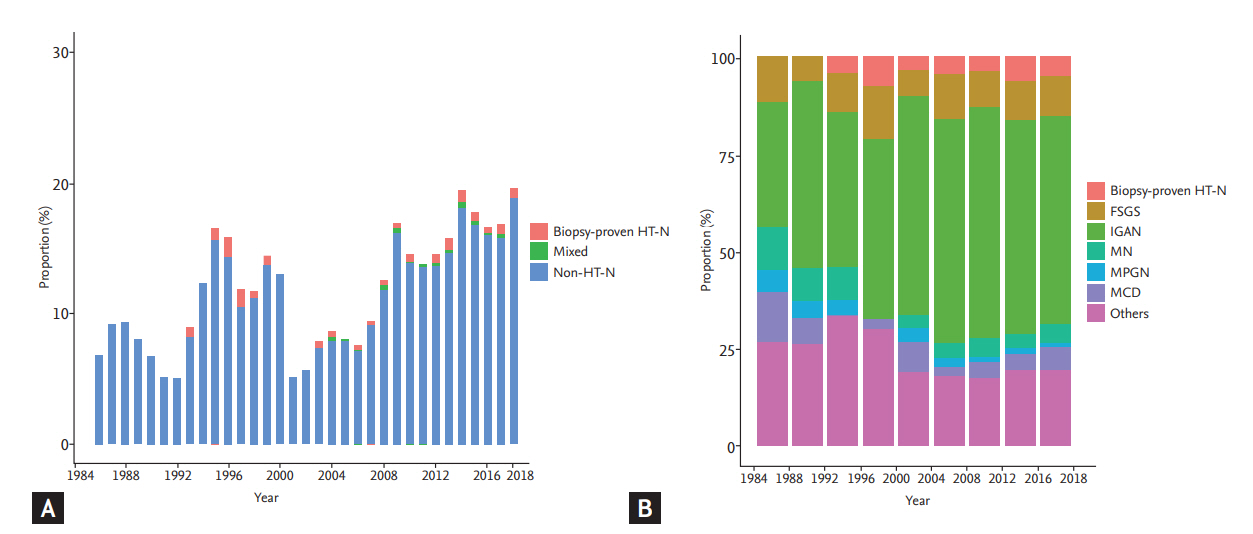
Temporal trends of renal pathologic diagnosis in patients with clinical hypertensive nephrosclerosis (HT-N). (A) Annual proportions of biopsy-proven HT-N (with no other pathologic diagnosis), mixed (HT-N combined with other pathologic diagnoses), and non-HT-N (pathologic diagnoses other than HT-N) in the total study cohort. (B) Annual proportions of biopsy-proven HT-N and other pathologic diagnoses in patients with clinical HT-N. FSGS, focal segmental glomerulosclerosis; IGAN, IgA nephropathy; MN, membranous nephropathy; MPGN, membranoproliferative glomerulonephritis; MCD, minimal change disease.
Table 5 shows the characteristics of the pathologic subgroups in clinical HT-N patients. Patients with biopsy-proven HT-N showed significantly lower eGFR and hemoglobin levels compared with non-HT-N patients. In a multivariable Cox proportional hazards model, the risk of ESKD development was not different between biopsy-proven HT-N and non-HT-N (hazard ratio [HR], 0.93; 95% CI, 0.54 to 1.59; p = 0.78) (Table 6), which was similar to the results of the complete case analysis (Supplementary Table 7). The risk factors of ESKD in clinical HT-N patients included eGFR, hemoglobin, and UPCR (Supplementary Table 8). For further assessment of outcomes of HT-N, we matched 103 patients with biopsy-proven HT-N and 206 non-HT-N patients using 1:2 propensity score matching for all relevant covariates (Supplementary Table 9). The standardized mean difference was less than 0.1 for all covariates after matching (Supplementary Table 10). The multivariable-adjusted Cox analysis in the matched group was consistent with the results before matching (HR, 0.92; 95% CI, 0.49 to 1.71; p = 0.78). The risk of death could not be assessed due to the small number of observed events in HT-N patients.
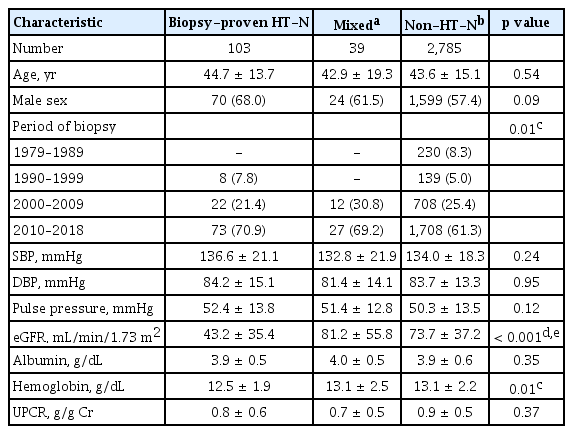
Clinical characteristics of patients with clinical HT-N

Associations between pathologic diagnoses and ESKD development in patients with clinical HT-N
DISCUSSION
To our knowledge, this is the first multicenter-based study of kidney biopsy in Korea, which included a large number of participants with long-term follow-up. Our findings revealed the spectrum and temporal trends over 40 years in biopsy-proven DN and hypertension-related kidney disease, as well as primary or secondary GN. The incidence of kidney biopsy in diabetic patients has increased substantially in the recent 30 years, and the incidence of DN has also increased. The ratio of the number of patients with biopsy-proven DN and NDRD did not change over the recent two decades. DN showed significantly higher risk for incident ESKD than NDRD. Biopsy-proven HT-N accounted for only a small proportion of clinical HT-N patients, and since the 1990s, its prevalence has not changed significantly. No significant difference was found in the risks of ESKD between biopsy-proven HT-N and non-HT-N. For other GNs, the prevalence of IGAN gradually increased, while those of LN and MPGN decreased in the past decades.
To date, there have been several studies of kidney biopsy registry in various regions, population, and institutions. Nevertheless, these studies have mostly described only the prevalence of biopsy-proven primary or secondary GNs during the follow-up period ranging from 3 to 20 years [6,19-23]. In the late twentieth and early twenty-first centuries, globally, lifestyle and socioeconomic status have changed substantially, accompanying the change in the prevalence of chronic diseases such as hypertension and diabetes. Particularly, the number of diabetic patients worldwide has nearly quadrupled between 1980 and 2014 [9]. Similar epidemiology of diabetes has been reported in the Korean population [24]. In a systematic analysis for the Global Burden of Disease Study 2013, the age-standardized rates for CKD due to diabetes increased globally by 10.6% between 1990 and 2013 [25]. Our findings suggest that the increasing incidence of diabetes has a significant effect on kidney diseases and outcome. From 1990 to 2018, the proportion of DN in total biopsy-proven kidney diseases increased over by two-fold. Moreover, the risk for incident ESKD in DN was significantly higher than in NDRD, which was consistent with other studies [26,27]. Indeed, in Korea, the most common cause of ESKD was GN in the early 1990s, but diabetes has been the most common cause since 1993 [28]. According to a nationwide survey by the Korean Society of Nephrology in 2014, 48% of ESKD was attributable to diabetes [28], which is similar in different countries [29,30]. Since the pathologic classification of DN was proposed in 2010, there has been a growing interest in the role of kidney biopsy in diabetic patients [12]. However, the reported prevalence of DN in kidney biopsy studies was similar or lower than that of NDRD; in studies including more than 100 diabetic patients, the proportion of DN ranges from 35% to 40% and NDRD from 40% to 50% [5,31]. In part, this high prevalence of NDRD could be attributed to the indication of kidney biopsy in diabetic patients. Nevertheless, in a cohort of diabetic patients with albuminuria, more than 20% of patients had NDRD confirmed by kidney biopsy [32,33]. Many diabetic patients are referred to the nephrologists at a late stage of CKD and clinically diagnosed with DN without kidney biopsy. Therefore, a large number of advanced CKD cases in diabetic patients may be caused by NDRD, and it may be an overestimate that 50% of new ESKD results from DN.
In this study, the proportion of NDRD in diabetic patients was relatively higher (68%) and temporally unchanged since the 2000s. This indicates that, for diabetic patients, renal biopsies have been performed very selectively, and the biopsy pattern and indication have not changed for recent decades in Korea. Patients with NDRD could benefit from specific therapeutic interventions for kidney diseases [26,34]. However, currently, there is no effective clinical tool for identifying NDRD without biopsy. Kidney biopsy is mainly performed in patients who have clinical features different from those of DN described in the Kidney Disease Outcomes Quality Initiative (KDOQI) guideline [35], such as nephrotic syndrome, proteinuria without diabetic retinopathy, and short duration of diabetes. Several studies have examined the predictive factors for NDRD [15,36] and proposed diagnostic models to distinguish between DN and NDRD [37,38], but no significant improvement has yet been made. In this regard, further studies are needed to reduce the gap between clinical and pathologic diagnoses and to increase timely and appropriate kidney biopsy in diabetic patients.
On the other hand, the prevalence of hypertension in Korea increased from 19.8% in 1990 to approximately 28% since 1998 [39]. Similarly, the proportion of hypertension as an underlying cause of ESKD in Korea has increased from less than 10% in 1980s to 16.0% in 1992 and then remained at 16.0% to 21.4% [28]. Hypertension has been the second most common cause of ESKD since 2000. In our study, although biopsy-proven HT-N was found more frequently since the 1990s than before, the proportion remained less than 2% of the entire biopsy cohort. Likewise, in other biopsy studies, the prevalence of HT-N was also as low as 2.5% to 9% [40-42]. In clinical practice, HT-N is usually diagnosed without kidney biopsy in non-diabetic patients with reduced GFR, hypertension, and low level or absence of proteinuria [43]. Kidney biopsy in hypertensive patients is selectively performed in cases such as those with increasing proteinuria, hematuria, and azotemia. Nevertheless, as shown in our results, the number of biopsy-proven HT-N is considered too small. Only 5% of clinically diagnosed HT-N patients had biopsy-proven HT-N. Similarly, in a study of 47 patients who met the clinical criteria of HT-N and underwent kidney biopsy, many cases had possible immune-complex-mediated GNs other than HT-N [44]. Actually, HT-N has been criticized as a vague umbrella term that does not correlate well with pathological findings such as arteriolar hyalinization and sclerosis [45]. Our findings indicate that the clinical criteria of HT-N are not adequate for providing pathologic diagnosis. Therefore, a substantial number of ESKD attributed to hypertension may be accompanied by other kidney diseases such as chronic GN. In addition, biopsy-proven HT-N showed no difference in risks for incident ESKD compared with non-HT-N. To date, studies of the prognosis in biopsy-proven HT-N are still limited. Recently, Ovrehus et al. [46] revealed that risks of ESKD and mortality for biopsy-proven HT-N did not differ from those for GNs, but significantly lower than those for DN. These findings suggest that the overall renal outcome of HT-N was not as poor as expected from the data in ESKD registries.
Among primary or secondary GNs, the most common GN in Korea has been IGAN, followed by MN, MCD, FSGS, and LN. This is similar to other populations in Asia such as Japan and China [47,48]. The prevalence of IGAN increased from 1990 to 2009 and then stabilized, and the prevalence of MPGN gradually decreased during the past decades, as shown in other single-center studies in Korea [8,19]. A decrease in MPGN may be caused by decreased infection and improvement in sanitation and socioeconomic status [49]. In addition, our findings showed a decrease in the prevalence of LN, which may result from early and effective therapeutic intervention, which hindered the development of LN [50].
In the present study, we explored the current and past spectrum and temporal trends of kidney diseases, focusing on hypertension and diabetes, the leading causes of CKD at the present era. To date, many studies have reported that the major cause of ESKD has changed from GN to diabetes and hypertension in the past decades. Although pathologic findings of DN and HT-N were found more commonly than decades ago, our findings indicate that a relatively large proportion of cases in patients with diabetes or hypertension might be attributed to other kidney diseases such as GN. This supports the need to consider kidney biopsy more actively for proper diagnostic approaches in patients with diabetes or clinical HT-N. Fortunately, kidney biopsy has increasingly been performed in patients with low-grade proteinuria or normal renal function; thus, histological diagnosis can be made earlier than before. Kidney biopsy for patients with clinically presumed DN or HT-N could provide early accurate diagnosis and appropriate management.
This study has limitations. First, despite the multicenter design, only the Korean population is included. Generalization to other populations is difficult. Ethnic factors are important in the prognosis of HT-N [51], but predispositions such as African American with apolipoprotein L1 variants could not be assess in this study. Second, since our study is based on retrospective data from the kidney biopsy registry, clinical variables such as laboratory tests and medications are limited. In particular, some important variables, such as duration of diabetes, presence of diabetic retinopathy, and hematuria were not available. Third, it may be unclear whether hypertension at the time of biopsy precedes kidney disease in hypertensive patients. However, in a real clinical setting, many hypertensive patients are referred for suspicion of kidney diseases without long-term follow-up.
In conclusion, our multicenter cohort study of kidney biopsy over 40 years showed that the incidence of DN has been rapidly increasing during the recent 30 years, contributing to ESKD development. However, NDRD was also consistently present in a majority of diabetic patients with kidney biopsy. Biopsy-proven HT-N was present in only a few of clinical HT-N patients, and the incidence remained unchanged since the 1990s. DN was associated with a higher risk of ESKD than NDRD, but biopsy-proven HT-N did not differ from non-HT-N in the risk of ESKD. Considering the high prevalence of NDRD or nonHT-N, further investigations are needed to determine the role of kidney biopsy in these populations.
KEY MESSAGE
1. In the recent 30 years in Korea, kidney biopsy has been increasingly performed in diabetic patients and biopsy-proven diabetic nephropathy have been found more frequently, which was associated with a higher risk of end-stage kidney disease (ESKD).
2. Biopsy-proven hypertensive nephrosclerosis (HT-N) has been found in a small proportion of patients with clinically presumed HT-N and did not differ from non-HT-N in the risk of ESKD.
3. Considering the high prevalence of non-diabetic renal disease or non-HT-N, further investigations for the role and indication of kidney biopsy might be needed.
Supplementary Materials
Supplementary Table 3.
Associations between biopsy-proven diagnosis and clinical outcomes in complete cases of diabetic patients (n = 2,078)
Supplementary Table 5.
Diagnostic indices of the clinical criteria of HT-N to distinguish biopsy-proven HT-N in total cohort.
Supplementary Table 7.
Associations between pathologic diagnoses and ESKD development in complete cases of patients with clinical HT-N
Supplementary Table 9.
Clinical characteristics of matched cohort among patients with biopsy-proven HT-N or non-HT-N
Notes
No potential conflict of interest relevant to this article was reported.