Weight change and microvascular outcomes in patients with new-onset diabetes: a nationwide cohort study
Article information
Abstract
Background/Aims
Because weight control is important in treatment of type 2 diabetes, it is essential to understand the associations between weight change and the risk of microvascular complications among patients with type 2 diabetes. We examined whether weight changes early after new-onset diabetes have an impact on the clinical outcomes of diabetic nephropathy and retinopathy.
Methods
Using the Korean National Health Insurance Service-National Health Screening Cohort database, 181,872 patients newly diagnosed with type 2 diabetes who were free of end-stage renal disease (ESRD) and proliferative diabetic retinopathy (PDR) during 2007 to 2012 were followed to the end of 2016. Weight change was defined as the difference in body weight from the time of diabetes diagnosis to 2 years later.
Results
We identified 180 cases of ESRD and 780 cases of PDR followed up for a median of 5.5 years from the index year at 2 years after diagnosis. Those with 5% to 10% weight gain showed a significantly higher hazard ratio (HR) for ESRD, compared with those with ≤ 5% weight change after adjusting for several confounding factors, including the baseline estimated glomerular filtration rate (HR, 1.75; 95% confidence interval [CI], 1.14 to 2.70). Those with ≥ 10% weight loss showed the lowest HR for PDR (HR, 0.52; 95% CI, 0.33 to 0.83), whereas those with ≥ 10% weight gain showed the highest HR for PDR (HR, 3.20; 95% CI, 2.51 to 4.08).
Conclusions
Weight gain after new-onset diabetes was associated with increased risk of ESRD and PDR whereas weight loss with decreased risk of PDR, but not ESRD.

INTRODUCTION
According to the increasing incidence of diabetes and the aging population, the main microvascular complications of diabetes—diabetic nephropathy (DN) and diabetic retinopathy (DR)—have become leading causes of end-stage renal disease (ESRD) and blindness, respectively. In DN, complex factors including hemodynamic changes, inflammation and hyperglycaemia aggravate renal function and lead to ESRD, which requires dialysis or transplantation. DR threatens all individuals with diabetes, leading to vision loss with severe proliferative DR (PDR) and a significant negative impact on quality of life [1–3]. Thus, DN and DR are multifactorial progressive microvascular complications of diabetes with irreversible poor outcomes. Mounting evidence has demonstrated that the diabetic milieu leads to increased local expression of inflammatory molecules, such as cytokines, chemokines and growth factors, and involves various expression changes in several inflammatory mediators in the development of DN and DR [2,4–6]. Because the retinal artery shares a common anatomical structure, risk factors and pathogenic mechanisms for organ dysfunction with those of arteries in the kidney, it is not surprising that diabetes-related exposure to inflammatory cascades is a common pathogenic mechanism [7–10].
Obesity may amplify a pro-inflammatory metabolic milieu [11,12]; thus, we can assume that weight gain may trigger the inflammatory cascade in patients with diabetes, and weight reduction may reverse the results. In experimental models, caloric restriction has shown antioxidant effects mediated by the induction of mitochondrial biogenesis and antioxidant enzymes and a reduction in free radical mitochondrial leakage during oxidative phosphorylation [13]. In addition, recent studies have revealed the beneficial impact of food control and exercise therapy on the composition of body physiologic factors in patients with chronic kidney disease (CKD) [14,15]. Because obesity is common among people with type 2 diabetes and weight control is a key management of diabetes, it is essential to understand the associations between weight change and the risk of microvascular complications such as DN and DR among patients with type 2 diabetes. Here, we investigated the association between weight change early after new-onset diabetes and the risk of ESRD or PDR using a nationwide population-based cohort.
METHODS
Data source and study population
In South Korea, the National Health Insurance System is the only insurer and managed by the government, providing regular health check-up programs to the public. Those enrolled in the health insurance service are recommended to undergo health check-ups at least biennially. In the current study, we included subjects (aged ≥ 30 years) who underwent a health examination between 2007 and 2012. Of these, we included only subjects with newly diagnosed diabetes who started taking diabetic medications within 1 year of their health check-up. We defined newly diagnosed diabetes patients as follows: (1) fasting blood glucose ≥ 126 mg/dL measured at a health examination during 2007 to 2012 and < 126 mg/dL during 2002 to 2006; (2) no previous history of any antidiabetic medications; (3) started taking diabetic medications within 1 year of the health examination under ICD-10 codes E11–14 [16–18]. Among the 326,650 newly diagnosed diabetic subjects, 184,720 underwent a second health examination during 2009 to 2014 (index year). We excluded subjects having ESRD, PDR or malignancy prior to the index year. The final study population consisted of 181,872 subjects (Fig. 1). This study was conducted according to the Declaration of Helsinki and approved by the Institutional Review Board of College of Medicine, The Catholic University of Korea (IRB No. SC18ZES10045). Because anonymized and deidentified information was used for the analyses, informed consent was not required.
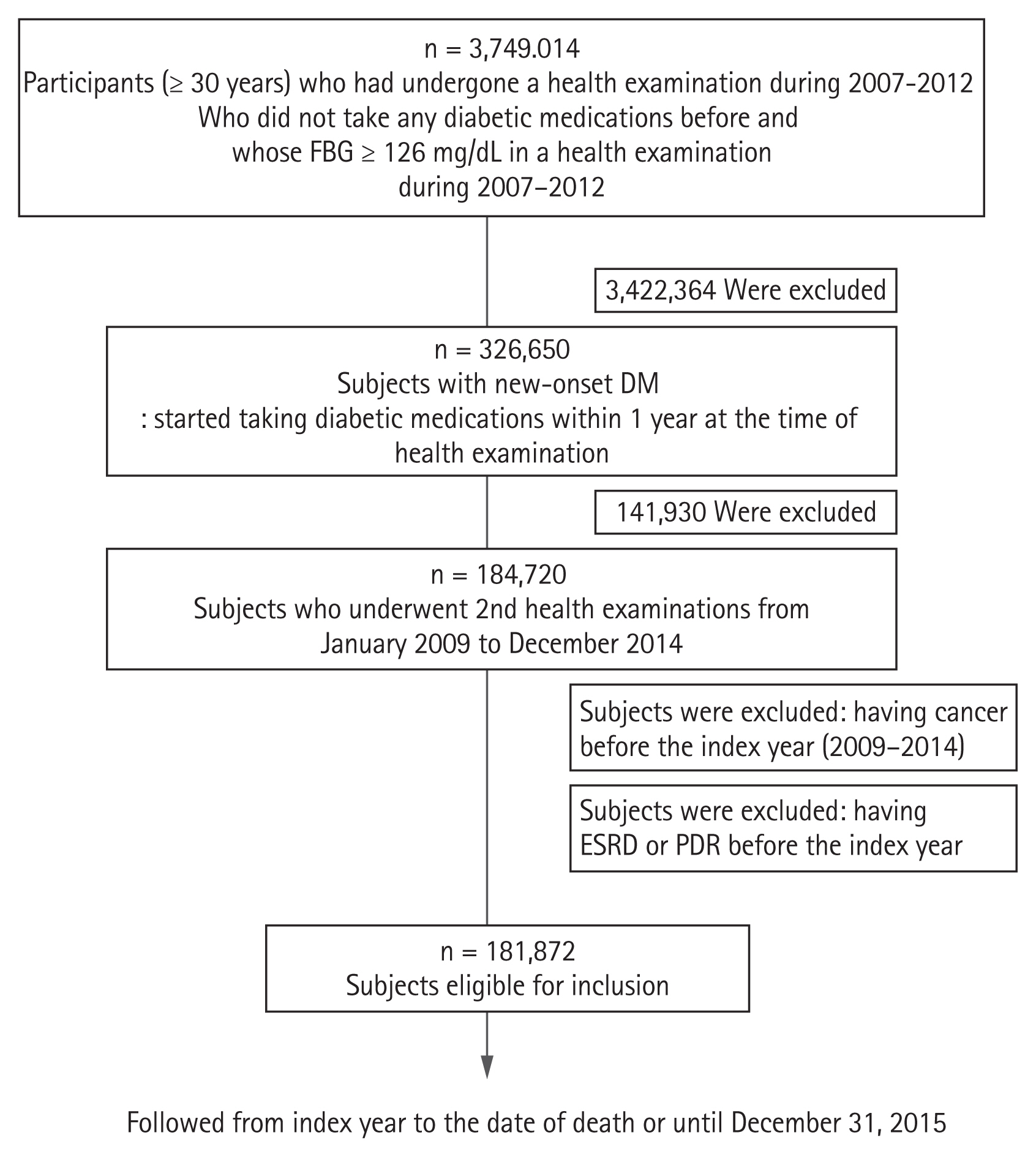
Flowchart of study population. FBG, fasting blood glucose; DM, diabetes mellitus; ESRD, end-stage renal disease; PDR, proliferative diabetic retinopathy.
Definitions of weight change
We calculated weight changes over a 2-year interval according to the difference in weight values between the first and second health exams, expressed as a percentage. We divided the individuals into five subgroups as follows: ≥ 10% weight loss, 5% to 10% weight loss, ≤ 5% weight change, 5% to 10% weight gain, and ≥ 10% weight gain.
Assessment of other variables
Blood samples for the measurements of serum glucose, creatinine (Cr) and total cholesterol levels were drawn after an overnight fast. The estimated glomerular filtration rate (eGFR) was calculated using the abbreviated Modification of Diet in Renal Disease formula: 175 × serum Cr (mg/dL) − 1.154 × age (year) − 0.203 × (0.742 if female). Low glomerular filtration rate was defined as an eGFR < 60 mL/min/1.73 m2 according to the U.S. National Kidney Foundation guidelines. Hypertension was defined according to the presence of at least one claim per year under ICD-10 codes I10 or I11 and at least one claim per year for the prescription of an antihypertensive agent or systolic/diastolic blood pressure (BP) ≥ 140/90 mmHg [16]. Dyslipidaemia was defined according to the presence of at least one claim per year under ICD-10 code E78 and at least one claim per year for the prescription of lipid-lowering agent or total cholesterol level ≥ 240 mg/dL [16,19].
Study outcomes and follow-up
The end points of the study were newly diagnosed ESRD or PDR. The incidence of ESRD was defined by a combination of the ICD-10 code (N18 to 19, Z49, Z94.0, Z99.2) and initiation of renal replacement therapy and/or kidney transplantation during hospitalization. All medical care expenses for dialysis were reimbursed using the Korean Health Insurance Review and Assessment Service database. These patients were also registered as special medical aid beneficiaries. Therefore, we were able to identify every ESRD patient in the South Korean population and analyse the data of all ESRD patients who had started dialysis [20]. Codes for treatment or medical expense claims included R3280 for kidney transplantation, O7011 to O7020 or V001 for haemodialysis, and O7071 to O7075 or V003 for peritoneal dialysis. We excluded individuals without previous CKD who had a transplant or dialysis code on the same date as an acute renal failure code. Subjects on continuous renal replacement therapy or acute peritoneal dialysis were also excluded [19,20]. PDR was defined by the procedure code S5160 or S5161 for pan-retinal photocoagulation in patients already diagnosed with DR (diagnostic code H36.0) [16]. The study population was followed from baseline at the index year to the date of ESRD or PDR diagnosis, or until December 31, 2016, whichever came first.
Statistical analysis
Baseline characteristics are presented as mean ± standard deviation or number (%). Participants were classified into five weight change categories. The incidence of primary outcomes was calculated by dividing the number of incident cases by the total follow-up duration (person-years). The disease-free probability of primary outcomes according to weight change subgroup was calculated using Kaplan-Meier curves, and the log-rank test was performed to analyse differences among the groups. Hazard ratios (HRs) and 95% confidence intervals (CIs) for ESRD and PDR were calculated using the Cox proportional hazards model for each weight change category. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and a p < 0.05 was considered to indicate significance.
RESULTS
Baseline characteristics of study population
The mean age of total study population was 56.3 years and 65.1% was male, and mean body mass index (BMI) and eGFR were 25.4 kg/m2 and 89.9 mL/min/1.73 m2, respectively. The baseline characteristics of the participants according to weight change over the 2-year period after the diagnosis of diabetes are listed in Table 1. At 2 years following the diabetes diagnosis, 68.3% of the par ticipants showed < 5% weight change, whereas 19.1% had ≥ 5% weight loss and 12.6% had ≥ 5% weight gain. The individuals with ≥ 10% weight gain were younger, more to be male, and tended to have a higher baseline BMI, height, waist circumference. Also, those with ≥ 10% weight gain were more likely to be a current smoker and a heavy drinker, and to have higher BP, fasting glucose level and higher prevalence of dyslipidemia.
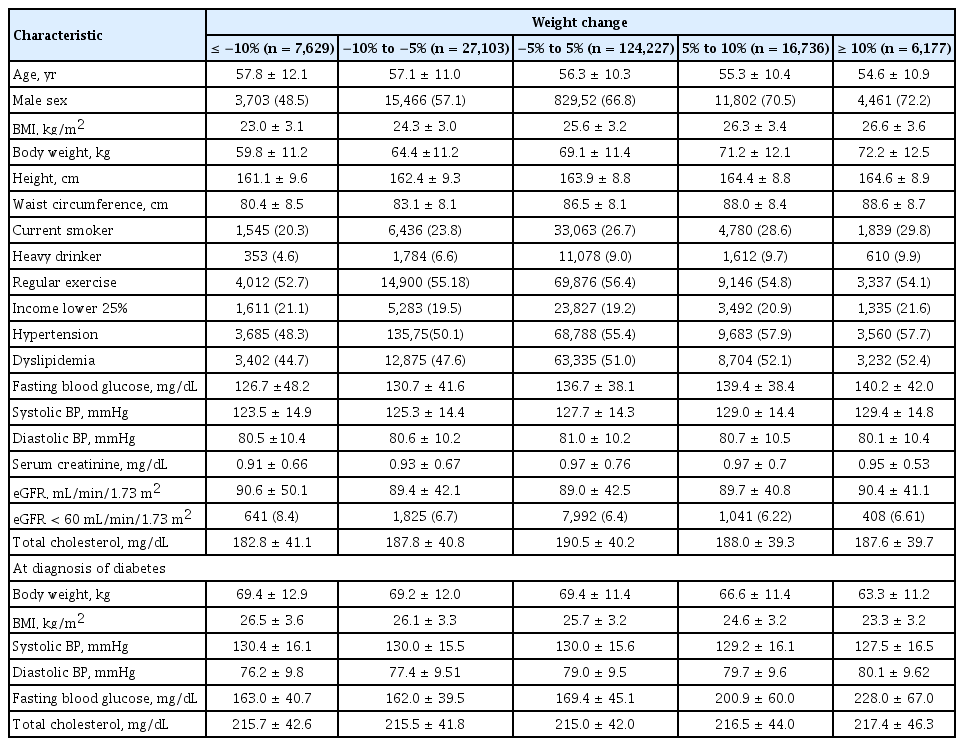
Baseline characteristics of study subjects according to the weight changes status
Risk of incident ESRD and PDR according to weight change group after diabetes diagnosis
There were 180 cases of ESRD (0.10%) and 780 cases of PDR (0.43%) during a median follow-up of 5.5 years from the index year at 2 years after newly diagnosed diabetes. Table 2 shows the HRs (95% CIs) of ESRD and PDR by the body weight change in patients with new-onset diabetes. Those with 5% to 10% weight gain had a significantly higher HR for ESRD, compared with those with < 5% weight change, after adjusting for several confounding factors, including BMI and the baseline eGFR (HR, 1.75; 95% CI, 1.14 to 2.70). In the case of PDR, those with ≥ 10% weight loss showed the lowest HR for PDR (HR, 0.52; 95% CI, 0.33 to 0.83), whereas those with ≥ 10% weight gain the highest HR for PDR (HR, 3.20; 95% CI, 2.51 to 4.08) (Fig. 2).

HRs and 95% CIs of clinical outcomes (ESRD and PDR) according to the weight changes status among the patients with new-onset type 2 diabetes
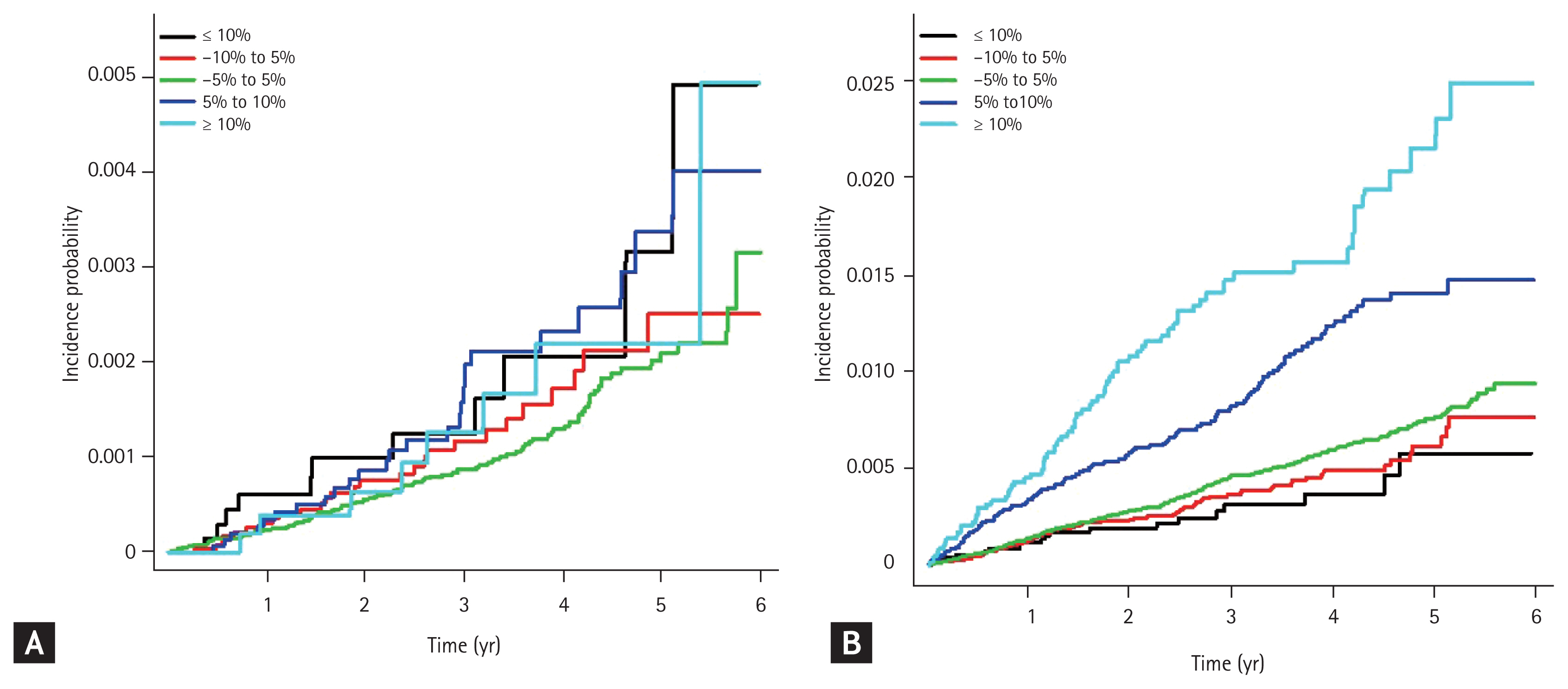
Kaplan-Meier estimates of cumulative incidence of (A) end-stage renal disease and (B) proliferative diabetic retinopathy among patients with newly diagnosed diabetes by the weight change categories.
Subgroup analysis
To evaluate the effect modifiers affecting the relationships between weight change and risk of ESRD and PDR, we conducted a stratified analysis using several factors such age, sex, smoking, drinking and exercise habits, income status, presence or absence of hypertension, dyslipidaemia or abdominal obesity, BMI and fasting glucose level (Fig. 3). Higher adjusted HRs for ESRD were associated with non-obesity (BMI < 25 kg/m2) and fasting blood glucose level ≥ 126 mg/dL in group with ≥ 5% weight gain, compared those with < 5% weight change, albeit there was no significant p for interaction. In the case of PDR, ≥ 5% weight gain remained predictive of worse survival and ≥ 5% weight loss better survival in compared with the < 5% weight change group in stratified analysis. The associations between weight change and risk of incident ESRD and PDR were not affected by the potential confounding factors.
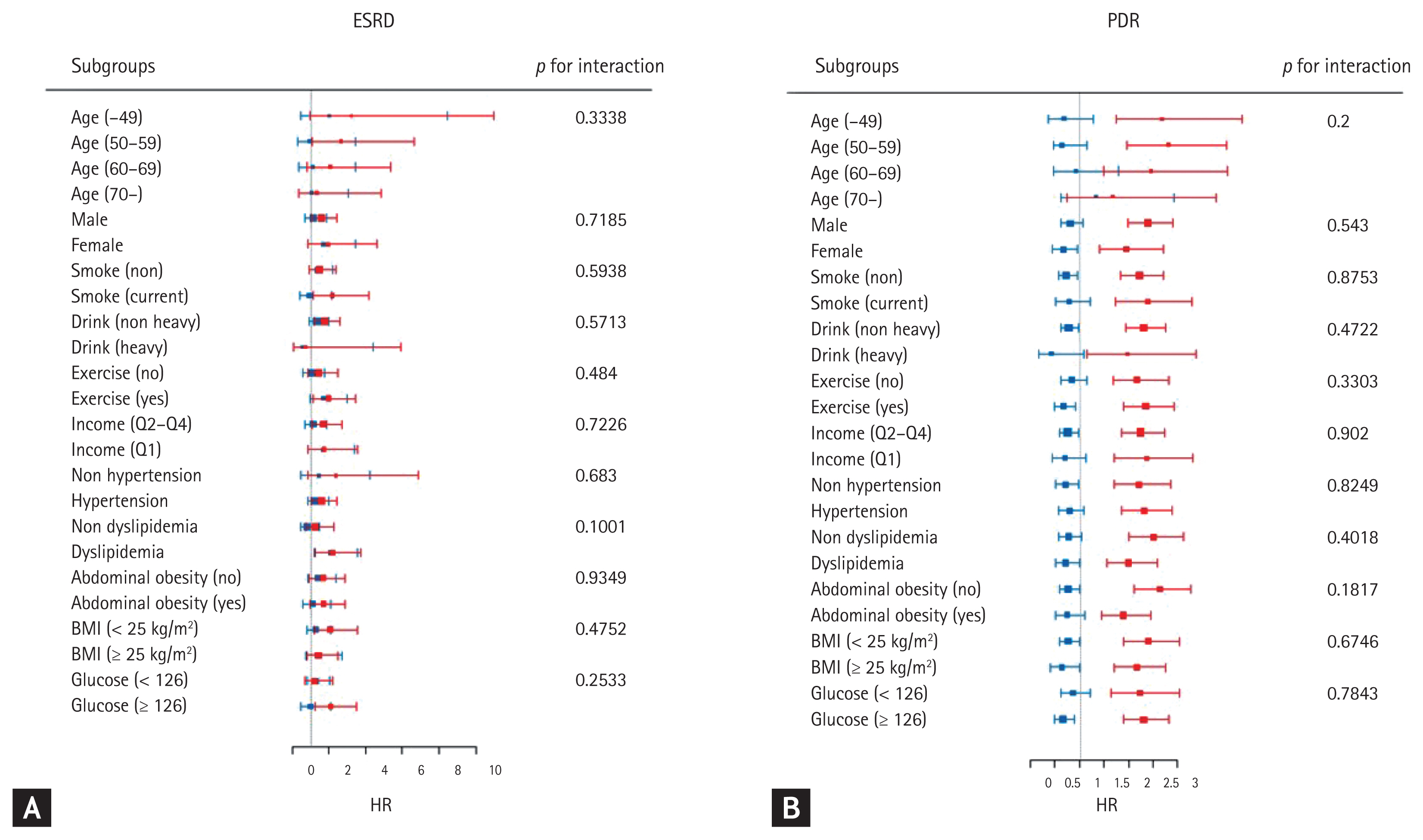
Subgroup analysis of association between the weight change categories and end-stage renal disease (ESRD) and proliferative diabetic retinopathy (PDR) stratified by age, sex, body mass index (BMI) and the presence of comorbidities. Hazard ratio (HR) and 95% confidence intervals of (A) ESRD and (B) PDR by the weight change categories. Blue square means HR of patients with ≥ 5% weight loss for ESRD and PDR compared with those with < 5% weight change as reference. Red square indicates HR of patients with ≥ 5% weight gain for ESRD and PDR compared with those with < 5% weight change. Adjusted for age, sex, BMI, alcohol drinking, smoking, regular exercise, income status, presence of hypertension and dyslipidemia, abdominal obesity, fasting glucose category, and estimated glomerular filtration rate.
DISCUSSION
In the present population-based study, weight change early after diabetes diagnosis was associated with the risk of ESRD and PDR. Weight gain during the 2 years after new-onset diabetes showed the higher risk of two microvascular complications of diabetes–ESRD and PDR, even after adjusting for confounding factors. Meanwhile, greater weight loss had an inverse association with the incidence of PDR, but not ESRD.
The current findings of association between greater weight gain and the risk of ESRD in new-onset diabetes can be explained by similar mechanisms of obesity-related renal outcomes. Obesity-related kidney injury has focused on changes in intrarenal hemodynamics, namely glomerular hyperfiltration, which is augmented by an increased extracellular volume and sodium reabsorption in the proximal tubule and altered tubuloglomerular feedback [11,21,22]. Over time, continued obesity-induced hyperfiltration contributes to thickening of the glomerular basement membrane and mesangial sclerosis, ultimately leading to renal function decline [23,24]. Thus, Impact of obesity on renal outcomes has been extensively focused in previous reports [25,26]. In a study of more than 100,000 screened individuals in Japan, the risk of ESRD was increased in subjects with a BMI > 25 kg/m2 [25]. Similarly, in a United States population, an increase in BMI led to a proportional increase in ESRD incidence over a median follow-up of 21 years [26]. As gradual weight gain eventually link to obesity, we can explain the impact of weight gain on renal function in the current study. However, weight loss early after diabetes diagnosis did not show a beneficial effect on renal outcomes in our study. This is inconsistent with the results of the Look Action for Health in Diabetes (AHEAD) study or effect of bariatric surgery, which suggested that in obese and overweight people with type 2 diabetes, weight reduction through intensive lifestyle interventions improves the microvascular complication of DN [27,28]. Data from these previous studies supported a direct effect of significant weight reduction on kidney function independent of the effects of diabetes and hypertension [29]. The ultimate difference is that the Look AHEAD study was an intervention study, whereas the current study was observational. Thus, weight loss can be indirectly caused by a combination of other comorbidities such as poor outcome of CKD-linked malnutrition [30–32], rather than active lifestyle modifications by each individual.
Meanwhile, our study found significant positive relationships between weight change after new-onset diabetes and PDR: the subjects with weight gain have more risk of PDR, whereas those with weigh loss had less risk of PDR. A number of previous studies have evaluated the association between obesity and DR; however, the findings are inconclusive [33–35]. In contrast to previously reported positive associations between BMI and DR, other study demonstrated protective effects of higher BMI on DR, predominantly among Asians [35]. Additionally, recent meta-analyses reported no increased risk of DR by elevated BMI [33,34]. Discriminating between obesity and weight gain, the current results demonstrated that weight gain after new-onset diabetes could be a strong and novel independent risk factor of DR. A possible mechanism for this is that weight change influences glycaemic control, in turn affecting clinical outcomes and presumably related to hemodynamic and vascular endothelial growth factor (VEGF)-dependent mechanisms, because improved hyperglycaemia by weight loss may downregulate VEGF expression in retinal cells. Also, other various metabolites derived by unstable weight change may facilitate the aggravation of DR, which needs further investigation [7,8,36–38].
The comorbidity of DN and DR is the unlucky linkage and the association of two diseases has been discussed because of the proximity of vascular structural determinants and overlap of pathogenetic pathways including genetic determinants. The prolonged hyperglycemia-induced vascular endothelial dysfunction of small vessel contributed to both the development and progression of DN and DR. DN has been implicated in the marked expression of VEGF, which is induced by mitochondrial damage to accelerate glomerular sclerosis and renal fibrosis, thereby promoting the progress of renal decline [39]. In addition, VEGF is linked with DR as a key driver behind neovascularization [40]. Although it is unclear how weight change has effect on the degree of vascular endothelial dysfunction, in terms of common pathologic process with a high VEGF expression between DN and DR, the current findings are interesting in that weight loss early after new-onset diabetes attenuated the risk of PDR whereas it did not affect the risk of ESRD.
Several caveats of the current analysis warrant further consideration. First, the follow-up period was relatively short to access the risk of incident ESRD and PDR. Second, we were not able to know whether body weight change were intentional or unintentional. For example, we could not fully exclude the other conditions affecting body weight change, such as medications or thyroid disease. Third, this was an observation study and the association between weight changes and the risk of incident ESRD and PDR may not be causal. Fourth, there is a limitation in the operational definition of PDR and ESRD because of the intrinsic characteristics of a nationwide cohort. Finally, there may have been possible selection bias when we excluded the subjects without the second health examination in 2009 to 2012, because we could not check the demographic equality of the excluded group with eligible study subject. Nevertheless, the strength of this study is that it evaluated a nationwide cohort of patients with new-onset diabetes with a large sample size and longitudinal design. In addition, this analysis did not focus simply on obesity or fragility, but weight gain and weight loss after new-onset diabetes, which includes a series of metabolic alterations over time. To our knowledge, this is the first study to evaluate the associations between weight change and diabetic microvascular complications in patients with new-onset diabetes, using abundant data including socioeconomics, biomedical information and lifestyle variables.
In conclusion, this large-scale cohort study of the Korean population showed that weight gain early after diabetes was associated with increased risk of ESRD and PDR, whereas weight loss was with decreased risk of PDR, but not ESRD. Regarding the risk of diabetic microvascular complications, we may suggest active surveillance for body weight in patients with new-onset diabetes.
KEY MESSAGE
1. Weight gain early after diabetes diagnosis was associated with increased risk of end-stage renal disease (ESRD) and proliferative diabetic retinopathy (PDR) whereas weight loss with decreased risk of PDR, but not ESRD.
2. Considering the risk of diabetic microvascular complications, we propose the active surveillance for body weight in patients with new-onset diabetes.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was performed using the database from the National Health Insurance System (NHIS-2018-1-258), and the results do not necessarily represent the opinion of the National Health Insurance Corporation. The research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2018R1D1A1B07049079). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.