Efficacy of long-term tenofovir disoproxil fumarate therapy in chronic hepatitis B patients with partial virologic response in real practice
Article information
Abstract
Background/Aims
The optimal management of chronic hepatitis B (CHB) patients with partial virologic response (PVR) to tenofovir disoproxil fumarate (TDF) remains unclear. We aimed to evaluate the long-term efficacy of prolonged TDF therapy in treatment-naïve CHB patients with PVR to TDF therapy in real practice.
Methods
We retrospectively investigated the efficacy of prolonged TDF therapy in treatment-naïve CHB patients with PVR to TDF. PVR was defined as a decrease in serum hepatitis B virus (HBV) DNA over 2 log10 IU/mL from baseline, with detectable HBV DNA by real-time polymerase chain reaction at week 48.
Results
We included 232 patients who underwent TDF therapy for over 48 weeks. Forty-two patients (18.1%) showed PVR. In multivariate analysis, hepatitis B e antigen (HBeAg) positivity, and high levels of serum HBV DNA at baseline and week 12 were independent predictive factors for PVR during TDF therapy. Out of 42 patients with PVR, 39 (92.9%) achieved virologic response (VR) during continuous TDF treatment; the cumulative VR rates at 24, 36, and 48 months were 79.8%, 88.2%, and 95.6%, respectively. With an additional 12 months of therapy, VR was achieved in 28/31 (90.3%) patients with HBV DNA < 100 IU/mL, compared to 5/11 (45.5%) patients with HBV DNA ≥ 100 IU/mL, at week 48.
Conclusions
The vast majority of patients achieved VR through prolonged TDF therapy, thus TDF treatment can be maintained in nucleos(t)ide-naïve patients with PVR at week 48, especially in those with low viremia.
INTRODUCTION
Chronic hepatitis B (CHB) is a major health problem worldwide and a leading cause of liver cirrhosis and hepatocellular carcinoma (HCC). The primary aim of antiviral therapy for CHB is long-term suppression of viral replication, which prevents disease progression, and consequently HCC development [1,2]. During long-term antiviral therapy, drug resistance and incomplete viral suppression correlate with increased risk of adverse liver events, including progression to cirrhosis, HCC, and death [3]. Several studies have reported that early viral suppression is important to reduce the risk of resistance to nucleos(t)ide analogues (NAs) [4,5]. Partial virologic response (PVR) is defined as a decrease in hepatitis B virus (HBV) DNA of more than 1 log10 IU/mL or 2 log10 IU/mL, but still detectable by real-time polymerase chain reaction (PCR) at week 24, according to previous CHB practice guidelines [6-8]. PVR is related to increased risk of antiviral resistance, treatment failure and progression of liver disease, especially in NAs with low genetic barrier to resistance, such as lamivudine (LAM), telbivudine (LdT), or adefovir (ADV) [9,10]. Therefore, early treatment modification, including switching to more potent NAs should be recommended in patients with PVR to these antiviral agents.
Currently, the main treatment option for CHB patients is a potent NA with high barrier to resistance, such as entecavir (ETV) and tenofovir disoproxil fumarate (TDF), which show predictable long-term antiviral efficacy [11]. Compared to LAM or ADV in treatment-naïve CHB patients, ETV and TDF showed superior virologic and biochemical responses. Furthermore, several studies reported that development of antiviral resistance was rare (< 1%) in ETV and did not occur in TDF after longterm treatment [11]. In case of antiviral therapy with drugs of high potency and lower rate of resistance, determination of PVR has been recommended at week 48 [2,11]. In clinical trials for treatment-naïve CHB patients with ETV monotherapy, 10% to 30% of patients show persistent detectable HBV DNA at week 48 [12,13]. However, recent studies have reported that continuous treatment using ETV lead to consistently increasing virologic response (VR) rate until after 1 to 4 years [14-16]. These results support the idea that treatment adaptation is not necessary in patients treated with high potent NAs with high genetic barriers including ETV, unlike less potent NAs with low barrier to resistance [11].
However, there are limited data regarding the VR to prolonged TDF therapy in patients with PVR. It is thus uncertain whether adjustment of antiviral therapy is required for patients treated with TDF. Therefore, the objectives of this study were to evaluate the efficacy of TDF in clinical practice for NAs-naïve CHB patients during a long-term period, to investigate baseline and on-treatment factors predicting PVR to TDF therapy, and to assess whether PVR affects long-term clinical outcomes of TDF treatment.
METHODS
Patients
CHB patients, treated with 300 mg TDF daily between January 2013 and March 2016 at Daegu Catholic University Hospital, were identified using the electronic medical records. The following inclusion criteria were applied: (1) treatment-naïve CHB patients, (2) over 18 years old, and (3) over 12 months TDF treatment. Patients were excluded if they had preemptive treatment during chemotherapy, or antibodies against hepatitis C virus, or human immunodeficiency virus or HCC, or poor compliance before achieving complete virologic response (CVR).
All patients were assessed at baseline and every 3 to 6 months during TDF therapy, including tolerability of medication, blood chemistry, HBV DNA titer, hepatitis B e antigen (HBeAg), and antibody against HBeAg (anti-HBe). Patients underwent HCC surveillance every 6 months: (1) abdominal ultrasound, (2) measurements of serum α-fetoprotein. During baseline assessment, we diagnosed cirrhosis clinically, based on imaging findings (abdominal ultrasonography or computed tomography, or magnetic resonance imaging) and compatible clinical features.
Definitions and study endpoints
The level of HBV DNA was quantified using real-time PCR (COBAS Taq-Man HBV quantitative test, Roche Molecular systems Inc., Branchburg, NJ, USA; detection limit = 20 IU/mL). Hepatitis B s antigen (HBsAg), HBeAg, antibodies against HBsAg, and anti-HBe were assayed using electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany).
CVR was defined as undetectable level of HBV DNA (< 20 IU/mL) at week 48 and VR was defined as undetectable serum HBV DNA during TDF treatment. PVR was defined as a decrease in HBV DNA of more than 2 log10 IU/mL, but still detectable by real-time PCR at week 48 in patients with good compliance [8]. Virologic breakthrough (VBT) was defined as an increase in serum HBV DNA of more than 1 log10 IU/mL compared to nadir during continued treatment [8]. Definition of alanine aminotransferase (ALT) normalization differed according to sex: < 30 IU/L for males and < 19 IU/L for females.
Statistical analysis
SPSS version 21.0 was used for all statistical analysis (IBM Co., Armonk, NY, USA). To compare categorical variables, we applied the chi-square or Fisher’s exact tests. Continuous data were compared between the groups using Student’s t test. Serum HBV DNA levels were logarithmically converted for analysis. Kaplan-Meyer statistics and the log-rank test were performed to compare the cumulative rate of VR. Univariate and multivariate analyses to identify clinical factors predicting PVR were performed using logistic regression. To determine the optimal cut-off values for HBV DNA level predicting PVR, median HBV DNA levels were calculated and validated by area under receiver operating characteristic (AUROC) curve. Statistical significance was accepted for p < 0.05.
Ethics statement
This study protocol was reviewed and approved by the Institutional Review Board (IRB) of Daegu Catholic University Hospital (CR-18-166). Documentation of informed consent was waived by the IRB because this study was a retrospective analysis of existing clinical data.
RESULTS
Baseline characteristics of patients
A total of 299 treatment-naïve CHB patients were administered TDF at Daegu Catholic University Hospital from January 2013 to March 2016. Among them, 67 patients were excluded; one patient due to HCV co-infection, 14 patients due to poor compliance before CVR, 19 patients due to HCC, 27 patients due to short treatment period (< 12 months), and six patients because of preemptive treatment. The remaining 232 patients were included in the analysis (Fig. 1). The median treatment duration was 40.4 months (range, 12.3 to 65.1). Baseline characteristics and laboratory data are summarized in Table 1. The mean age of patients was 51.3 ± 11.3 years, and more than half were male (55.2%). One hundred and twelve patients (48.3%) had liver cirrhosis and 125 patients (53.9%) were HBeAg-positive. Two hundred and twelve patients (91.4%) had abnormal ALT levels. The mean baseline serum ALT level was 245.3 ± 445.6 IU/L and the serum HBV DNA level was 6.30 ± 1.42 log10 IU/mL.

Flow diagram of the selected study population. TDF, tenofovir disoproxil fumarate; CHB, chronic hepatitis B; HCV, hepatitis C virus; HCC, hepatocellular carcinoma; CVR, complete virologic response; PVR, partial virologic response.

Baseline characteristics
Clinical outcomes of TDF therapy at week 48
Among the 232 patients, 190 (81.9%) achieved CVR at week 48. A total 42 patients (18.1%) showed PVR at week 48 even though drug compliance was optimal (Table 2). HBeAg-negative patients showed a significantly higher rate of CVR compared with HBeAg-positive patients (95.3% vs. 70.4%, p < 0.001), and a significantly lower rate of PVR (4.7% vs. 29.6%, p < 0.001). Overall mean reduction of HBV DNA from baseline was 6.30 ± 1.42 log10 IU/mL. The degree of HBV DNA reduction was significantly greater in HBeAg-positive than in HBeAg-negative patients (6.99 ± 1.15 log10 IU/mL vs. 5.50 ± 1.28 log10 IU/mL, p < 0.001). The proportion of patients with normal ALT was 70.6% at week 48 and it was not significantly different between HBeAg-positive and HBeAg-negative patients (67.2% vs. 75.3%, p = 0.226). Out of the 125 HBeAg-positive patients, 20 (16.0%) showed HBeAg seroconversion or loss at week 48.

Clinical outcomes of tenofovir disoproxil fumarate therapy at week 48
Factors associated with PVR
We attempted to determine predictive factors for PVR. Comparison of characteristics between patients with CVR and PVR showed that younger age (51.9 ± 11.3 vs. 48.2 ± 10.8, p = 0.047), HBeAg positivity (46.3% vs. 88.1%, p < 0.001), higher serum HBV DNA level at baseline (6.03 ± 1.36 log10 IU/mL vs. 7.56 ± 0.91 log10 IU/mL, p < 0.001) and week 12 (1.45 ± 1.17 log10 IU/mL vs. 3.22 ± 0.91 log10 IU/mL, p < 0.001), and higher rate of detectable serum HBV DNA at week 24 (27.4% vs. 100%, p < 0.001) were significantly associated with PVR (Table 3). We analyzed the optimal cut-off levels of HBV DNA at baseline and week 12 for TDF therapy that could maximally predict PVR. The optimal cut-off value of serum HBV DNA level for the prediction of PVR was 6.34 log10 IU/mL at baseline (AUROC, 0.718; 95% confidence interval [CI], 0.655 to 0.775; sensitivity, 85.7%; specificity, 57.9%), and 1.91 log10 IU/mL at week 12 (AUROC, 0.776; 95% CI, 0.717 to 0.828; sensitivity, 95.2%; specificity, 60.0%) (Supplementary Fig. 1and 2).

Comparison of clinical characteristics between patients with complete virologic response and patients with partial virologic response at week 48
The clinical factors that are associated with PVR at week 48 were analyzed using univariate and multivariate logistic regression analysis (Table 4). We included age, liver cirrhosis, HBeAg positivity, baseline serum HBV DNA level ≥ 6.34 log10 IU/mL, and HBV DNA at week 12 ≥ 1.91 log10 IU/mL for analysis. HBeAg positivity (odds ratio [OR], 3.875; 95% CI, 1.352 to 11.109; p = 0.012), baseline serum HBV DNA level ≥ 6.34 log10 IU/mL (OR, 3.766; 95% CI, 1.406 to 10.088; p = 0.008), and HBV DNA at week 12 ≥ 1.91 log10 IU/mL (OR, 16.829; 95% CI, 3.848 to 73.612; p < 0.001) were independently associated with PVR.

Univariate and multivariate logistic regression analysis of clinical factors associated with partial virologic response during tenofovir disoproxil fumarate therapy
Overall clinical outcomes during long-term continuous TDF therapy
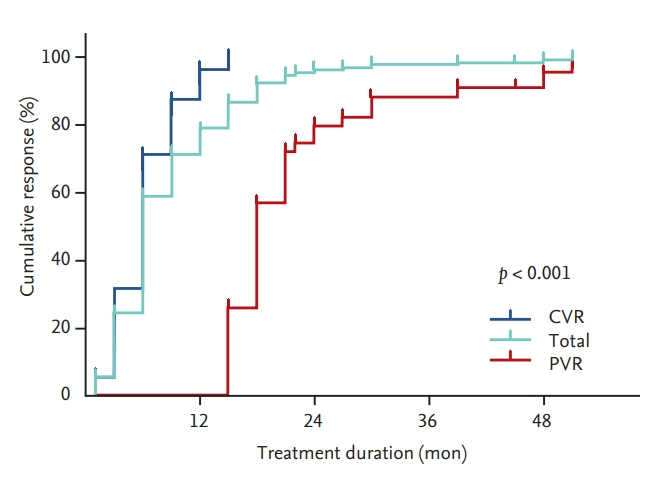
During long-term TDF therapy, 229 patients (98.7%) achieved VR, irrespective of PVR. The overall cumulative rates of VR at 12, 24, 36, and 48 months were 78.9%, 96.3%, 97.9%, and 99.2%, respectively (median time to VR, 6 months; range, 1.0 to 51.0) (Fig. 2). Out of 42 patients with PVR, 39 (92.9%) achieved VR during continuous TDF treatment. The three patients that did not achieve VR at the end of follow-up included one that was lost to follow-up after 18 months and another two that showed a continuous decline of serum HBV DNA level. The median time to VR in patients with PVR was 18 months (range, 15 to 51). The cumulative rates of VR in patients with PVR at 24, 36, and 48 months were 79.8%, 88.2%, and 95.6%, respectively (Fig. 2). We performed subgroup analysis of VR in patients with PVR during long-term TDF therapy according to the HBV DNA level at week 48. The cumulative rates of VR at 24, 36 and 48 months were significantly higher in patients with HBV DNA level < 100 IU/mL at week 48 compared to those with HBV DNA level ≥ 100 IU/mL at week 48 (92.9%, 96.5%, and 96.5% vs. 45.5%, 65.9%, and 100%, respectively; p = 0.019) (Fig. 3).
Cumulative rates of virologic response between patients with partial virologic response (PVR) and patients with complete virologic response (CVR) at week 48.

Cumulative rates of virologic response in patients with partial virologic response according to the level of hepatitis B virus DNA at week 48.
Overall rates of ALT normalization and HBeAg seroconversion during long-term follow-up were 86.8% and 19.2%, respectively. Among patients with PVR, 34 (85.0%) showed ALT normalization and three (8.1%) achieved HBeAg seroconversion during prolonged TDF therapy. Three patients with HBsAg loss and two patients with HBsAg seroconversion were observed (median duration 21 months; range, 17 to 24). Among three patients with HBsAg loss, one patient with PVR showed HBV reactivation at 12 months after stopping TDF treatment.
Ten patients with CVR (5.3%) and one patient with PVR (2.4%) showed VBT after 48 weeks. All VBT in patients with CVR was caused due to skipping medication for more than 2 weeks, and these patients achieved VR within 1 to 6 months after continuous TDF therapy. We performed genetic mutation test in one patient with PVR, who showed VBT at 19 months despite drug compliance. There was no genotypic resistance to TDF according to restriction fragment mass polymorphism, and the patient achieved VR at 51 months after prolonged TDF therapy.
In our study, deterioration of renal function was not observed in any patient during the entire treatment period. After a median 42.8 months of treatment, six out of the 42 patients with PVR showed mild hypophosphatemia (serum phosphorus level < 2.7 mg/dL) while their serum creatinine levels did not exceed 0.5 mg/dL. During long-term TDF therapy, the most common liver-related events were HCC (n = 16), followed by variceal bleeding (n = 3), and ascites (n = 1). All events of variceal bleeding and ascites were developed within 12 months after starting TDF treatment. Sixteen patients developed HCC during a median follow-up period of 22 months (range, 6 to 49). One patient died from hepatic failure due to reactivation of HBV after stopping TDF treatment. There was no significant difference in any liver-related events between patients with and without PVR.
DISCUSSION
During treatment with oral antiviral agents, persistent viral replication has been related to adverse treatment outcomes [9,10]. Thus, it is important to check PVR at an adequate time point according to the antiviral potency and genetic barrier to resistance. Early treatment adaptation was recommended to prevent treatment failure and development of resistance in patients with PVR receiving LAM, LdT, or ADV [7]. However, for patients with ETV or TDF therapy showing PVR, recommendations in international guidelines are not uniform as to whether treatment should be continued or switched to another drug [2,11,17]. Currently, several studies have reported that the vast majority of treatment-naïve patients with PVR under ETV therapy achieved further VR during prolonged ETV therapy without treatment adaptation [14-16]. In contrast, there are very limited data for patients with PVR to TDF and it is still uncertain whether TDF therapy is modified or continued in patients with PVR.
In this study, 42 out of 232 patients treated with TDF failed to achieve CVR at week 48. Among patients with PVR, 39 patients (92.9%) achieved further VR without treatment modification during a median period of 18 months (range, 15 to 51). This result is in accordance with previous studies of ETV therapy demonstrating that the vast majority of patients with PVR showed VR after prolonged ETV treatment [14-16,18]. Furthermore, the rate of VR in patients with PVR was higher in our study than in previous studies of ETV treatment. Thus, our study suggests that treatment should be continued using the same agent without modification in patients with PVR to TDF.
Several baseline and on-treatment predictors for PVR have been investigated in patients treated with NAs. Previous studies reported that high baseline HBV DNA and HBeAg positivity, as pretreatment factors, have been associated with PVR [14,16,18-20]. Regarding on-treatment factors during ETV therapy, Kwon et al. [15] suggested that more than 2,000 IU/mL of serum HBV DNA at week 12 and detectable serum HBV DNA at week 24 were significantly associated with PVR. However, it is unclear which clinical factors can predict PVR in NAs-naïve patients treated with TDF. In this study, we showed that high levels of serum HBV DNA at baseline and week 12, and HBeAg positivity were independent predictive factors for PVR during TDF therapy. The optimal cutoff value of baseline HBV DNA level to predict PVR was 6.34 log10 IU/mL. The rate of PVR in patients with higher baseline HBV DNA (≥ 6.34 log10 IU/mL) and in those with lower baseline HBV DNA (< 6.34 log10 IU/mL) were 31.0% (36 of 116 patients) and 5.2% (six of 116 patients), respectively. HBeAg positivity was another baseline predictive factor for PVR. HBeAg-positive patients showed higher PVR rate than HBeAg-negative patients. In particular, most HBeAg-negative patients (95.3%) achieved CVR. We also found on-treatment factors to predict PVR during TDF therapy, for example serum HBV DNA level at week 12. Using the optimal cut-off value of HBV DNA level at week 12 (1.91 log10 IU/mL), the rate of PVR was higher in patients with HBV DNA level ≥ 1.91 log10 IU/mL at week 12 than in those with lower level of HBV DNA at week 12 (34.5% vs. 1.7%, p < 0.001).
We showed that most patients with PVR at week 48 achieved further VR after prolonged TDF therapy (79.8% at 24 months, 88.2% at 36 months, and 95.6% at 48 months). According to the HBV DNA level at week 48, the cumulative rate of further VR was higher in patients with HBV DNA level < 100 IU/mL than in those with HBV DNA level ≥ 100 IU/mL at week 48. Furthermore, the vast majority of patients (28 of 31 patients, 90.3%) with HBV DNA level < 100 IU/mL at week 48 achieved VR within an additional 12 months of therapy, compared to patients with HBV DNA level ≥ 100 IU/mL (five of 11 patients, 45.5%). Two previous ETV studies also reported that lower viral load at week 48 could predict further VR in patients with PVR [14,15]. However, the level of HBV DNA at week 48 predicting VR was lower in our study than in previous ETV studies (< 1,000 IU/mL [14], < 2,000 IU/mL [15]). In addition, the cumulative rate of further VR in our study was higher than in previous studies of ETV therapy, especially in patients with higher viral load at week 48. These inconsistent findings may be due to the more potent antiviral efficacy of TDF than of ETV.
The clinical impact of long-term low-level viremia (HBV DNA < 2,000 IU/mL) in patients with CHB is unclear. In previous observation studies, the risk of developing liver cirrhosis and HCC was not higher in patients with persistent low-level viremia than in those with undetectable HBV DNA [21,22]. However, recently reported studies suggest that persistent low viral load might be considered as a risk factor for HCC development, particularly in patients with high level HBsAg or liver cirrhosis [23-25]. With regard to ETV therapy, consistent low viral load is associated with a higher risk of HCC in patients with liver cirrhosis [26]. In our study, two (4.8%) out of 42 patients with PVR and 14 (7.4%) out of 190 patients with CVR developed HCC during a median follow-up period of 22 months (range, 6 to 49). This result did not show any clinical impact of persistent low-level viremia on developing HCC in patients receiving TDF therapy. Further prospective studies with larger sample size are required to determine the exact outcomes of long-term TDF treatment.
Tenofovir alafenamide (TAF), a recently developed prodrug of tenofovir, delivers the active ingredient to the hepatocytes more efficiently and requires a lower dose than TDF to achieve a therapeutic concentration in hepatocytes [27]. The long-term TDF therapy results in high systemic exposure to tenofovir, which is related to renal and bone toxicity [28,29]. International phase III trials comparing the efficacy and safety of TAF with that of TDF in CHB patients showed that the virologic efficacy was similar between TAF therapy and TDF therapy; however, the ALT normalization, renal and bone safety were in favor of TAF therapy [30]. In these studies, the TDF group showed declines in fasting total cholesterol, low density lipoprotein cholesterol, and high density lipoprotein cholesterol levels while median changes in fasting lipid profiles were small in TAF group [30]. When safety profiles of TDF and TAF are compared, switching to TAF therapy will be a better strategy than continuing TDF in patients with PVR as TDF therapy contributes to renal or bone toxicity.
Our study has some limitations. First, it was a retrospective, single tertiary center study, thus characteristics of patients might be limited. Second, data on other clinical factors affecting VR were insufficient, including genotypes, precore/core promoter mutation, and HBsAg levels. Despite the drawbacks of our study, our results suggest that most patients with PVR to TDF can achieve undetectable HBV DNA during long-term TDF treatment without modification of antiviral therapy.
In conclusion, adaptation of TDF therapy in NAs-naïve patients with PVR at week 48 is unnecessary. TDF therapy in NAs-naïve patients shows excellent viral suppression in real-world practice. Although the time to reach VR was delayed, prolonged TDF therapy beyond week 48 results in further VR in most patients with PVR, particularly in those with HBV DNA < 100 IU/mL at week 48.
KEY MESSAGE
1. Continuous tenofovir disoproxil fumarate (TDF) treatment beyond week 48 results in further virologic response in most patients with partial virologic response.
2. There was no significant difference in any liver-related events between patients with and without partial virologic response.
3. Adaptation of TDF therapy in nucleos(t)ide analogues-naïve patients with partial virologic response is unnecessary.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The authors thank Sang Gyu Kwak, PhD, Department of Medical Statics, Daegu Catholic University School of Medicine, for his statistical consultation for this study.