Clinical and economic analysis of the 2009 H1N1 influenza pandemic among pregnant Korean women
Article information
Abstract
Background/Aims
Unlike Western countries, the 2009 pandemic influenza infection among pregnant women was reported as mild in a previous interim study in South Korea. However, several mortalities were reported thereafter, suggesting that nationwide data were lacking.
Methods
This case-control study covers the entire 2009 pandemic inf luenza period, from May 2009 to February 2010. The clinical and economic data of pregnant (case) and age-matched non-pregnant (control) women with influenza A (H1N1) pdm09 virus (H1N1pdm09) infection were retrospectively collected from nine hospitals in South Korea.
Results
A total of 130 pregnant women with H1N1pdm09 infection were identified. The mean age of the pregnant women was 31.1 years (range, 19 to 41) and mean gestational age was 18.4 weeks (range, 3 to 40). Both case and control groups were similar in terms of age (p = 0.43) and comorbidities (p = 0.18). The overall rate of complications was comparable between the two groups (p = 0.648). However, mortality was reported only among the cases, so mean economic per capita burden is estimated to be higher for pregnant women compared to the control (4,821,992 Korean won [KRW] vs. 351,233 KRW, p = 0.31). Obstetric complications were observed in 12 cases, including preterm labor (n = 7), low birth-weight (n = 3), miscarriage (n = 1), stillbirth (n = 1), and cleft lip (n = 1).
Conclusions
Although statistically insignificant, the detrimental impact of influenza A H1N1pdm09 on pregnancy can be serious in some complicated cases in South Korea. Thus, the strong recommendation of influenza vaccination should be maintained for pregnant women as a high priority.
INTRODUCTION
Influenza is a major global cause of morbidity and mortality, resulting in an estimated three to five million cases of severe illness and 250,000 to 500,000 deaths annually [1,2]. The risk of complication from influenza is known to increase depending on risk factors, including age, comorbidity, and pregnancy [1-3]. Changes in the immune system, heart, and lungs of pregnant women make them more susceptible to severe illness from influenza, and result in serious problems for the unborn fetus, including premature labor and delivery [4-6]. The impact of influenza on pregnancy has been reported in previous pandemics, particularly the increased risk of complications among pregnant women compared to general population [7,8]. The 2009 influenza A (H1N1) pdm09 virus (H1N1pdm09) pandemic was the first influenza pandemic to occur in the era of modern obstetric and intensive care management; however, during this pandemic, these similar and serious outcomes were also found among pregnant women in many countries [3,9-14]. Accordingly, the World Health Organization recommends influenza vaccination for pregnant women as the highest priority group.
In contrast to most studies from countries other than Korea, which showed worse clinical courses from influenza during pregnancy in the 2009 pandemic, a few countries reported that influenza A H1N1pdm09 infection did not cause significant concern among pregnant women [15-18]. This regional disparity warrants the need to evaluate the significance of pregnancy in diverse geographic regions. In South Korea, multi-center analysis reported mild clinical features in pregnancy without any mortality during the 2009 pandemic [19]. However, after this interim analysis, several fatal cases were reported [20,21], suggesting that nationwide data on the clinical impact of the 2009 pandemic influenza on pregnant Korean women were lacking.
In this study, pregnant women with influenza A H1N1pdm09 infection were evaluated in comparison with non-pregnant controls with respect to disease complications and economic burden.
METHODS
Selection of study subjects
We performed a retrospective case-control study in women of reproductive age (ages between 18 and 44 years) admitted to nine university hospitals in cities of South Korea (Seoul, n = 2; Incheon, n = 1; Ansan, n = 1; Suwon, n = 1; Wonju, n = 1; Daegu, n = 1; Busan, n = 1, and Gwangju, n = 1) between May 2, 2009 (date of confirmation of the first case of pandemic influenza A(H1N1) pdm09 in Korea) and February 28, 2010 (decline of the influenza pandemic). A case was defined as a pregnant woman with laboratory-confirmed H1N1pdm09 infection, and was an outpatient or inpatient. H1N1pdm09 infection was diagnosed from respiratory specimens by using the rapid antigen test or real-time reverse-transcription polymerase chain reaction assay. Age-matched controls (age of case ± 5 years) were non-pregnant women with pandemic influenza infection who had visited the same hospital as a study subject during the study period. If multiple persons met the inclusion criteria, the person who visited the hospital on the nearest date to that of a respective case patient was selected as a control.
Data collection
A standardized case report form was used to collect the following data from the patients’ medical records: age, trimester of pregnancy (in case of pregnancy), previous medical history, hospital admission, intensive care unit (ICU) admission, duration of hospitalization, influenzarelated complications and mortality, obstetric results, medical treatments and procedures, and medical costs.
Calculation of medical costs
We classified costs as direct and indirect, and we used formula from a previous study for the calculation of medical costs [22]. Direct cost, the cost incurred during hospitalization or while visiting a clinic, was subdivided into direct medical cost and direct non-medical cost. The direct medical cost was defined as the cost of treatment. This was extracted from the hospital’s financial database, which included both outpatient and inpatient cost information such as: hospitalization expenditures, nursing, influenza-related prescription drugs, examination, fees, and so forth. Medication costs among outpatients were calculated by quantifying the total price using the reference price (http://www.kimsonline.co.kr/drugcenter/calculator/drugcalculator) of prescription drugs that were verified as influenza-related drugs by health-care professionals in each hospital. The direct non-medical cost was defined as a sum of transport expenses and nursing costs [23]. Data from the Korea Health Panel (2010) were used for transport expenses (7,597 Korean won [KRW]), which were corrected using the traffic price index of Korean Statistical Information Service (KOSIS) [24]. In the case of hospitalized patients, the transport expenses were calculated triple including the two visits of guardian per hospitalization. The nursing cost was applied as KRW 60,000 per day, according to the result of “research on the institutionalization of nursing services” reported by the Ministry of Health and Welfare and the Korean Institute for Health and Social Affairs.
For estimating the indirect costs, the human capital approach was used, which is based on the cost of lost workdays owing to the disease. Annual data of KOSIS were used to determine the employment rate and average daily income [24]. Based on the results of a previous study, the proportion was presumed to be one-thirds which meant that the indirect cost of three patients at a clinic was equivalent to that of one patient in a hospital ward [25]. The cost of lost income due to early death was restrictively applied to persons aged 20 to 65 years with an annual interest rate of 3%. The estimated costs of disease were calculated in KRW.
Statistical analysis
Data were analyzed using SPSS software version 12.0 for Windows (SPSS Inc., Chicago, IL, USA). Basic frequencies and proportions were calculated. We conducted univariate and bivariate analyses to compare the characteristics of the pregnant women with those of infected non-pregnant women; chi-square and Fisher exact tests were performed to test the significance of the differences in the proportions.
Ethical approval
This study was performed with the approval of the Institution Review Boards (IRBs) of the selected university hospitals (IRB No. AS14085, KUGH11088). The study was performed in accordance with the Helsinki Declaration of 1975, as revised in 2000. Each patient in the current study was informed about data usage for this investigation. However, because this study was a retrospective medical record- based study and the study subjects were de-identified, the IRB waived the need for written consent from the patients.
RESULTS
During the study period, 130 pregnant women with influenza A H1N1pdm09 infection presented to our hospitals. The characteristics of these women and the matched control group are shown in Table 1. The mean age of the pregnant women was 31.1 years (range, 19 to 41); 107 women (82.3%) were in the first or second trimester of pregnancy and 23 (17.7%) were in the third trimester of pregnancy. Overall, only five patients (3.8%) had medical comorbidities that put them at an increased risk of influenza-related morbidity.

Characteristics of pregnant (case) and non-pregnant women (age-matched controls) with confirmed pandemic influenza A H1N1pdm09 virus infection
The two groups were similar in terms of age (p = 0.43) and comorbidity (p = 0.18). It was difficult to assess the significance of comorbidities because of the low prevalence. Among 201 women (77.3%) with available data of vaccination history, the vaccination rate among the pregnant women was 32% which was similar to that of non-pregnant women (p = 0.631).
Receipt of antiviral treatment between the two groups was significantly different (71.5% of pregnant women and 87.7% of non-pregnant women, p = 0.001). However, in terms of starting antiviral treatment within 2 days of symptom-onset, the two groups showed similar results (75.6% and 79.1%, for pregnant and non-pregnant women, respectively) (p = 0.559).
The comparison of disease burden between the pregnant and non-pregnant women with influenza A H1N1pdm09 infection is shown in Table 2. Although the incidence was too small to verify any significant result, the overall rate of complications was similar between the two groups (p = 0.648), and mortality was reported only in the pregnant group. Overall 13 of the pregnant women (10%) were admitted. The hospitalization rate was higher among the pregnant women (p = 0.051), but the hospitalization period was shorter, with a mean length of hospital stay of 7.3 days among the pregnant women and 12.8 days in the non-pregnant group. Most pregnant women were admitted due to influenza-like illness (11 of 13 cases, of whom nine were uncomplicated, and two were complicated influenza-like illnesses), except two cases with pregnancy-related complications. We had two pregnant women with influenza A H1N1pdm09 infection complicated by pneumonia, one of whom died. The patient who died was a 30-year-old woman at 31 weeks of gestation, with gestational diabetes diagnosed at 28 weeks, who present with a 3-day history of fever, cough, and breathlessness. Despite receiving oseltamivir treatment and ICU care, she died on day 26 of hospitalization. Two non-pregnant women had infections that were complicated by pneumonia; neither of them was admitted to ICU or died.
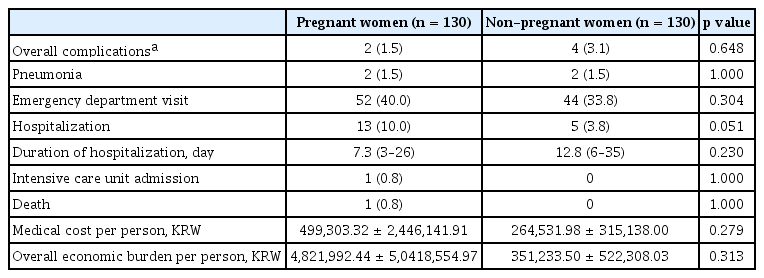
The Comparison of Influenza-related complications and economic burden between pregnant and non-pregnant women with pandemic influenza A H1N1pdm09 virus infection
Among the patients in the study, obstetric complications included preterm labor (n = 7), low birth-weight (n = 3), miscarriage (n = 1), stillbirth (n = 1), and cleft lip (n = 1) (Table 3). In the analysis of pregnant women with obstetric complications, the median maternal age was 30.5 years (range, 19 to 33) and only three of them (25%) had comorbidity. Of these cases with obstetric complications, only one had a respiratory complication during the treatment period, and she died owing to pneumonia.
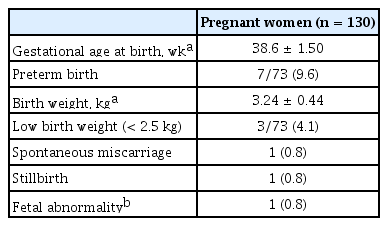
The pregnancy-related complications among pregnant women with pandemic influenza A H1N1pdm09 virus infection
When pregnant women with influenza A H1N1pdm09 infection were classified by gestational age, there was no substantial difference between the groups in terms of maternal age and comorbidities. Pregnancy-related complications and hospitalization rate tended to increase in the third trimester (pregnancy-related complications [n = 12], 13% in the third trimester, 8.3% in the second, and 8.5% in the first, p = 0.787; or hospitalization rate [n = 13], 17.4% in the third trimester, 8.3% in the second, and 8.5% in the first, p = 0.428). Assessing the association between respiratory complications and the stage of pregnancy was not possible because of the small number of events (n = 2).
Although not statistically significant, the overall economic per capita burden tended to be higher for pregnant women than for non-pregnant women (4,821,992 KRW and 351,233 KRW, respectively, p = 0.31) (Table 2). With the exception of one death, the average per capita burden for the pregnant women was 400,242 KRW, which was similar for both groups (p = 0.457), and direct medical costs accounted for more than 70% of the costs in both groups. However, in the analysis that included the one death, the cost owing to lost workdays was dramatically increased, changing the largest proportion of economic burden to indirect costs (86.7%) in the case group.
DISCUSSION
To the best of our knowledge, this was the first study to analyze the clinical impact of influenza infection on pregnant women during the entire period of the most recent pandemic influenza season in South Korea. This hospital-based case-control study identified the clinical and economic burdens of pandemic influenza A H1N1pdm09 infection among pregnant Korean women in comparison with those among non-pregnant women. There were no significant differences found between the two groups. Although the higher rate of admission could be understood in relation to disease severity, the preferential hospitalization of pregnant women might lead to an overestimation of the influenza burden in pregnant women. Evidence of this is found in the shorter length of hospital stay and the hospitalization of the majority of pregnant women owing to uncomplicated influenza-like illnesses.
The obstetric complications observed in this study were similar to those of the general population. Among 73 patients (56.2% of total) with available data, preterm delivery was 9.6%. This was much lower than previously found in countries outside Korea, with a premature birth rate of 15% to 36% [12,14,26,27] but similar to a baseline rate of preterm birth of 9.6% worldwide [28]. The incidence of low birth weight of 4.1% was also lower than the 9% to 30% reported in studies outside Korea [12,14,17] but similar to 4.9% reported in Korea birth statistics, 2009 [29]. Fetal abnormalities were recorded in one case (cleft lip, n = 1). It seemed to be more common in the study group than in the general population as reported in Korea (0.8% vs. 0.1%) [30]; however, these findings should be interpreted with caution considering the small number of events. Furthermore, it is difficult to confirm that these fetal abnormalities were directly related to influenza A H1N1pdm09 infection.
Observations from past pandemics and seasonal influenza epidemics have identified pregnant women to be susceptible to influenza-related mortality and morbidity. The 2009 pandemic outbreak appeared to be a severe one, as reported in the United States, Australia, and France [10,12,14,26]. However, a low clinical burden was also reported in some Asian countries including Japan, Singapore, and Indian Island [15-17]. In Korea, as shown in this study, pregnant women did not carry a higher burden of the disease than non-pregnant women did after influenza A H1N1pdm09 infection. Such mild clinical features among Korean pregnant women may be explained by several factors. First, the majority (96.2%) of our patients had no recognized comorbidities except for the pregnancy itself. In the United States, Australia and France, which reported a greater pandemic severity in pregnancy, overall 21% to 56% of infected pregnant women had documented comorbidities [10,12-14,26,31]. Second, a smaller number of pregnant women in their third trimester were enrolled in our study (17.7%) than in previous studies that reported worse outcomes (26% to 78%) [10,12,31]. Data from previous pandemics and seasonal influenza suggest that the risk of influenza complications might be higher in the advanced stages of pregnancy [27,32,33]. In accordance with this, our study observed a higher proportion of influenza-related complications occurring in the third trimester of pregnancy. The underlying mechanism is not well understood, but the physiologic changes that accompany the advanced stages of pregnancy such as decreased functional capacity of the lungs and increased oxygen consumption may support the concern about the increased risk of serious complications [33]. Third, early antiviral treatment might be related to favorable clinical outcome. Among the pregnant women, the majority (75.6%) received antivirals within 2 days of the onset of symptoms. Other countries that reported greater pandemic severity such as the United States and Australia also reported a similar proportion of antiviral use among pregnant women with influenza infection (50% to 85%) [10,26,31], but less than half of them received oseltamivir within 2 days of the onset of symptoms. Similarly, a French study found that delayed administration of antivirals was strongly associated with severe outcomes, regardless of antiviral use. Fourth, the high seasonal influenza vaccination rate among pregnant women could be interpreted as reflecting heightened public interest. The vaccination rate for seasonal influenza was only 4% among Korean pregnant women before the 2009 pandemic [34]; however, as many as 32% of the pregnant women were vaccinated during the pandemic season in this study. Increased interest may have aided in preventing them from contracting influenza or developing severe complications. Fifth, although not examined in this study, the maternal complications were low compared to other studies, which might be due to the relatively low prevalence of obesity in Korean women. Based on the Organisation for Economic Co-operation and Development (OECD) report, the prevalence of obesity (body mass index > 30) among Korean women was 4.1%, the lowest among OECD countries, except Japan [35]. Based on this report, Japan, China, and India, which also reported less pandemic severity among pregnant women [15,17,18], have a prevalence of obesity of less than 5%, suggesting that the lower rate of severe complications seen in Asian countries might be attributable to a relatively low body mass index. It was known that obesity was associated with increased maternal complications [18]. Lastly, cultural differences such as an easily accessible health care system in Korea might explain the mild course of the pandemic influenza in pregnant Korean women. This is supported by the findings that two-thirds of pregnant women were admitted to hospital within 24 hours of the onset of symptoms, compared to a median 1.5 to 6 days of interval between symptoms and presentation in other countries [14,26,31,36]. In addition, other factors such as genetic susceptibility, family size, crowding [37], local immunity and regional differences in virus strain [38,39] could be probable factors to explain our results of milder cases.
This study has the following limitations. First, this study had a retrospective design. We did not collect certain data that were relevant to influenza infection and pregnancy such as obesity. In addition, data related to gestational age and birth weight was only available in 56.2% of total cases. Second, this study was only conducted at tertiary referral hospitals. This might not be a significant bias among pregnant women because tertiary hospitals in Korea are easily accessible, and pregnant women with fever tended to visit tertiary referral hospitals. However, for the control group of these young patients with influenza, tertiary referral hospital can be a bias. Considering this, the clinical outcome among pregnant women with influenza infection might be underestimated. However, the baseline characteristics including comorbidities were not significantly different between the two groups in this study. Third, this study did not distinguish between seasonal influenza vaccine and pandemic monovalent vaccine. However, considering that monovalent influenza A H1N1pdm09 vaccine was not available for use in pregnant women until December 21, and 80% (104/130) of the pregnant women in this study were admitted before this date, the effect of the pandemic vaccine was thought to be negligible. Therefore we cannot estimate vaccine effectiveness in this study, but we can use the result to understand the public interest by observing the overall increased vaccination rate.
In conclusion, compared to non-pregnant women, pregnant women with influenza A H1N1pdm09 infection in South Korea did not carry a significant risk of complications. However, the overall economic burden in pregnant women was estimated to be higher because of one death reported in the pregnant group. The clinical outcome of influenza infection among pregnant women might be influenced by gestational age, accessibility to medical care, the timing of antiviral treatment, and host factors. Although statistical significance was not shown in this study, influenza vaccination should be recommended to pregnant women as a high priority, considering the serious and detrimental impact of influenza-related complications on pregnancy.
KEY MESSAGE
1. The economic burden of the 2009 pandemic influenza was higher for pregnant women than for non-pregnant women.
2. Obstetric complications were observed in 9.2% of the pregnant women during the 2009 pandemic influenza.
3. This study supports the current Korean recommendation to administer inf luenza vaccine during pregnancy as a high priority.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported by a grant of the Korea Healthcare Technology R&D Project from the Ministry of Health and Welfare Republic of Korea (No. A103001).