Physiologic approach for coronary intervention
Article information
Abstract
When invasively assessing coronary artery disease, the primary goal should be to determine whether the disease is causing a patient's symptoms and whether it is likely to cause future cardiac events. The presence of myocardial ischemia is our best gauge of whether a lesion is responsible for symptoms and likely to result in a future cardiac event. In the catheterization laboratory, fractional flow reserve (FFR) measured with a coronary pressure wire is the reference standard for identifying ischemia-producing lesions. Its spatial resolution is unsurpassed with it not only being vessel-specific, but also lesion-specific. There is now a wealth of data supporting the accuracy of measuring FFR to identify ischemia-producing lesions. FFR-guided percutaneous coronary intervention of these lesions results in improved outcomes and saves resources. Non-hemodynamically significant lesions can be safely managed medically with a low rate of subsequent cardiac events.
INTRODUCTION
Coronary angiography remains the reference standard for evaluating patients with angina, abnormal noninvasive stress imaging tests, and suspected or known ischemic heart disease. However, numerous studies have revealed the limitations of coronary angiography and, in particular, its inability to accurately detect ischemia-producing coronary artery disease. Recently, more refined methods for invasively determining the functional significance of coronary artery disease have been developed and extensively tested. The goal of this manuscript is to review the physiologic evaluation of patients with ischemic heart disease.
BACKGROUND
The presence of myocardial ischemia is a strong predictor of adverse outcome. The presence and severity of ischemia detected noninvasively with myocardial perfusion imaging correlates directly with the rate of cardiac death during long-term follow-up [1]. Moreover, relieving myocardial ischemia, whether by medical therapy or by coronary revascularization improves outcomes [2]. Conversely, performing percutaneous coronary intervention (PCI) on lesions that are not responsible for ischemia does not improve outcomes and may worsen them [3]. Therefore, a primary goal should be to identify patients with a large degree of myocardial ischemia and effectively treat them to reduce their ischemic burden.
Unfortunately, although our noninvasive tests detect the presence or absence of ischemia, their spatial resolution does not provide accurate information regarding the ischemic potential of a particular coronary stenosis in a particular coronary vessel, especially when multivessel coronary disease is present [4]. For these reasons, interventional cardiologists turn to coronary angiography as the reference standard for diagnosing coronary artery disease. However, studies have shown that interventional cardiologists can accurately identify an ischemia-producing lesion when it is angiographically very severe (i.e., > 90% narrowed), however, when it is between 50% to 90% narrowed on coronary angiography, our ability to determine the lesion's functional significance based on the angiogram alone is poor [5].
The realization that the accurate detection of ischemia-producing lesions, and perhaps as important, non-ischemia-producing lesions is critical in determining whether or not to perform PCI has led to a shift from so-called anatomic complete revascularization (i.e., revascularizing all lesions greater than 50% narrowed) to a new paradigm termed "functional" complete revascularization (i.e., revascularization of only ischemia-producing lesions and medical therapy for non-ischemia-producing lesions) [6]. The invasive physiologic evaluation of patients with ischemic heart disease using wire-based techniques to measure indices, such as fractional flow reserve (FFR), allow for a more refined approach to our patients with ischemic heart disease and help to guide our decisions regarding the need for PCI.
FFR
FFR has become the reference standard for invasively assessing the physiologic significance of intermediate coronary disease. First described by Pijls et al. [7], FFR is defined as the maximum flow down a vessel in the presence of a stenosis compared to the maximum flow in the hypothetical absence of the stenosis. It is based on the assumption that at maximal hyperemia microvascular resistance is minimized and constant. Under this condition, resistance is minimized and myocardial flow becomes proportional to pressure. The equation for FFR can be changed to the hyperemic distal coronary pressure in the presence of a stenosis compared to the coronary pressure in the hypothetical absence of the stenosis. In a normal epicardial artery, there is very little loss of pressure from the proximal to distal region. For this reason, in a diseased vessel the proximal pressure is a reflection of what the distal pressure would be if there was no disease. Therefore, FFR can be defined as distal coronary pressure divided by proximal coronary pressure during maximal hyperemia (Tables 1 and 2).
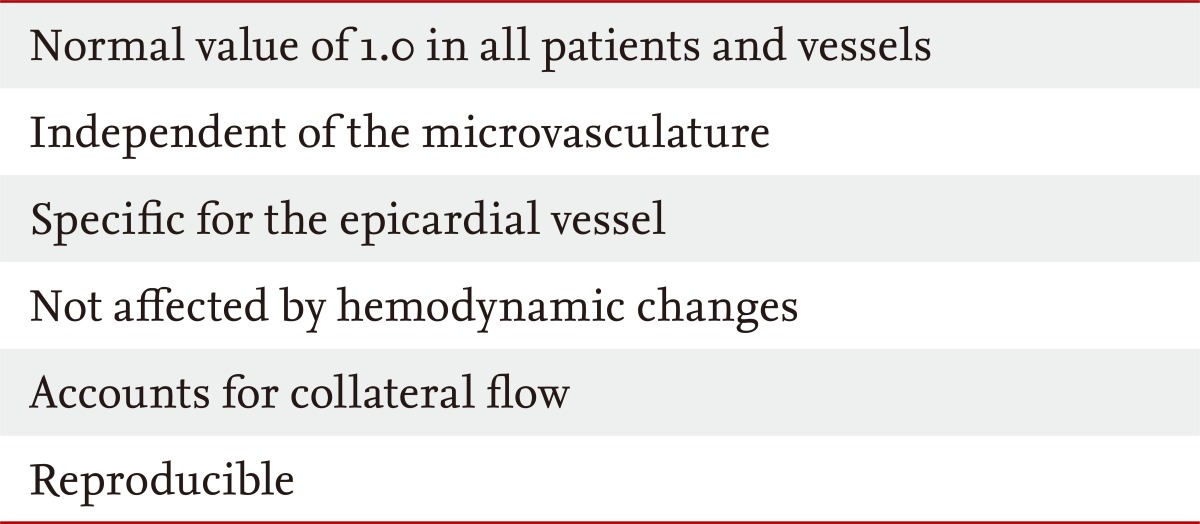
Unique aspects of fractional flow reserve
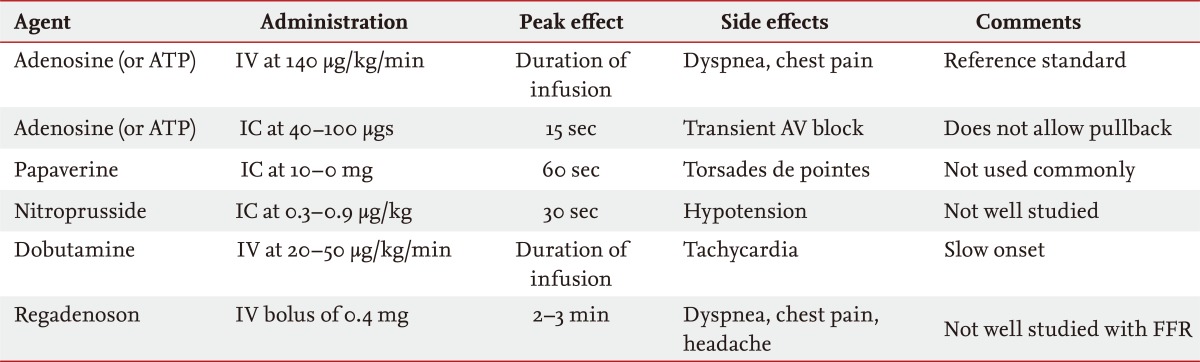
Hyperemic agents
In a landmark study, Pijls et al. [8] validated FFR for the assessment of intermediate coronary narrowing by comparing it to three different noninvasive stress tests. If any one of the stress tests was positive for ischemia, then the patient was defined as having ischemia. By using composite information from all three stress tests, the authors were able to increase the accuracy of the noninvasive diagnosis of ischemia. Using a cutpoint of 0.75, they found that 100% of the 21 patients with an FFR below 0.75 had ischemia and 88% of the 24 patients with an FFR of 0.75 or greater did not have ischemia. Importantly, revascularization was not performed in these 24 patients and at an average of 14 month follow-up there were no cardiac events in this group. The overall accuracy of FFR for identifying ischemia-producing lesions in patients with single vessel intermediate disease was 93%.
A number of subsequent studies have confirmed the accuracy of FFR for diagnosing ischemia-producing intermediate lesions in a variety of patient populations, including multivessel coronary disease, in comparison to a variety of noninvasive stress tests, and after myocardial infarction [9]. The best cut-off value in most of these studies has been between 0.75 and 0.80. This region has been termed the "grey zone." If the FFR is above 0.80, one can be fairly certain that significant ischemia is not present, and as described in more detail below, the patient will do well with medical therapy alone. If the FFR is below 0.75, one can be certain that ischemia is present and revascularization will improve symptoms and may improve outcomes. When the FFR falls in the "grey zone," clinical judgment is required. If a patient has a proximal left anterior descending coronary lesion and classic symptoms, one might opt for revascularization. If on the other hand, the patient has atypical or no symptoms, an equivocal stress test and/or is undergoing evaluation for noncardiac surgery, one might opt for medical therapy.
Safety of deferring PCI based on FFR
The safety of deferring revascularization of intermediate coronary narrowings which are not hemodynamically significant (i.e., FFR ≥ 0.75) was tested in the DEFER study [10]. In this multicenter trial, 325 patients with single vessel intermediate coronary disease underwent FFR measurement. If the FFR was below 0.75 then the patient underwent PCI. If the FFR was ≥ 0.75, then the patients were randomized to either PCI (with bare-metal stents in approximately 50% and angioplasty alone in the remainder) or to deferral of PCI with medical treatment. At 2-year follow-up, the event-free survival was similar in the defer group as compared to the perform group (89% vs. 83%, p = 0.27). More recently, follow-up was extended to 5 years and the event-free survival remained similar between the two groups (80% vs. 73%, p = 0.52) and the cardiac death and myocardial infarction rate in the defer group was less than one-half of what it was in the perform arm (3.3% vs. 7.9%, p = 0.21) [3]. This study and a number of other retrospective single center studies have confirmed the safety of treating hemodynamically non-significant intermediate coronary disease with medical therapy alone [11].
FFR and intermediate left main coronary disease
An important subset of intermediate coronary lesions in which FFR measurement has been applied is the group with indeterminate left main coronary stenosis. Because of the importance of the left main coronary and the size of the myocardial territory supplied by the left main, there has been concern that FFR, in general, and in particular, a cut-off of 0.75 to 0.80 may not be valid in this subset. In a recent review of published single center studies evaluating a strategy of deferring revascularization of intermediate left main lesions with an FFR > 0.75 to 0.80 found that in 236 patients the survival at greater than 2-year follow-up was 100% and the event-free survival was excellent and similar, if not better than in patients with an ischemic FFR who underwent revascularization [12].
The largest and most recent study evaluating FFR measurement in patients with moderate left main disease found that in 213 patients with equivocal left main disease, if the FFR was 0.80 or higher, as it was in 138 patients, the 5-year survival rate was 90% and compared favorably to the 85% survival rate in the 75 patients with an FFR < 0.80 who underwent coronary artery bypass grafting [13]. The 5-year event-free survival was 74% in the patients with an FFR of 0.80 or higher and also similar to the revascularization group. This study and the previous smaller studies support the idea that FFR measurement in left main disease is safe and useful in guiding the decision to perform revascularization, just as it is in patients with intermediate coronary disease not involving the left main coronary.
FFR-guided management of intermediate coronary disease
If an intermediate coronary narrowing has a non-ischemic FFR then it is unlikely to be responsible for a patient's symptoms and can be safely managed medically. If, however, an intermediate coronary narrowing is responsible for an ischemic FFR, then it is likely contributing to the patient's symptoms and may be more likely to cause future cardiac events. In this setting, if the lesion is amenable to PCI and particularly if the patient continues to have symptoms despite medical therapy, many would advocate revascularization with the aim at relieving symptoms and improving outcome. The data to support this FFR-guided approach come from the FFR versus Angiography for Multivessel Evaluation (FAME) trial [6].
The FAME study was a prospective, multicenter, international, randomized trial comparing two strategies for guiding PCI in patients with multivessel coronary disease, a significant proportion of whom had at least one intermediate lesion. Over 1,000 patients with stenoses ≥ 50% in two or three vessels which the operator deemed warranted PCI based on the angiographic appearance and clinical data were randomized to either angiography-guided PCI, in which case the identified lesions underwent routine PCI with drug-eluting stents, or to FFR-guided PCI, in which case FFR was measured and PCI was performed on a lesion only if the FFR was < 0.80.
Roughly three lesions were identified per patient and 47% of these were between 50% and 70% narrowed. The angiography-guided group received almost three stents per patient, while the FFR-guided group received approximately two stents per patient, a highly significant difference. Importantly, the FFR-guided approach did not take any longer than the angiography-guided one and significantly less contrast media was required in the FFR-guided patients.
The primary endpoint of the study was the 1-year major adverse cardiac event rate, a composite of death, myocardial infarction, and the need for repeat revascularization. This occurred in 18.3% of the angiography-guided patients and 13.2% of the FFR-guided patients, a significant difference (p = 0.02). The combination of death and myocardial infarction was also significantly reduced by the FFR-guided strategy (11.1% vs. 7.3%, p = 0.04) (Fig. 1).

Fractional flow reserve (FFR) versus Angiography for Multivessel Evaluation (FAME) trial: 1 year outcomes [6]. Data from the FAME trial [6] demonstrating a 30% to 40% reduction of each endpoint with FFR-guided percutaneous coronary intervention (PCI) as compared to angiography-guided PCI. The combination of death and myocardial infarction (MI) was significantly reduced, as was the primary endpoint, major adverse cardiac events (MACE).
These results have been extended out to 2 years with a persistent significant reduction in death and myocardial infarction (12.9% vs. 8.4%, p = 0.02) and a lower rate of major adverse cardiac events (22.4 vs. 7.9, p = 0.08) in the FFR-guided patients [14]. Importantly, of the 513 lesions in the FFR-guided patients on which PCI was deferred because the FFR was > 0.80, only one lesion (0.2%) caused a myocardial infarction and only 16 (3.2%) required revascularization. The percentage of FFR-guided patients free from angina at 2 years was 79.9% compared to 75.8% of the angiography-guided patients (p = 0.14).
Another important message from the FAME trial was the limitation of angiography for determining functionally significant lesions [15]. Of the intermediate narrowing between 50% and 70% narrowed, 35% had an FFR ≤ 0.80 and 65% did not. Of those lesions between 71% and 90% narrowed, a group typically deemed significant, 20% had an FFR > 0.80 and PCI was safely deferred. Of the patients in the FFR-guided group with angiographic three vessel coronary disease, only 14% had functional three vessel coronary disease and the majority had only one or two vessels with FFR ≤ 0.80. The FAME trial reinforced the safety of deferring PCI on lesions (many of which were intermediate) with an FFR > 0.80. It also highlighted a new paradigm of functionally complete revascularization in which ischemia-producing lesions are treated with PCI and non-ischemia producing lesions are treated medically.
Most recently, the role of FFR to guide intervention in stable patients with coronary disease was evaluated in the FAME 2 trial [11]. In this study, patients with stable coronary disease were randomized to either PCI or to best medical therapy. The key difference, however, between this study and previous ones comparing these two strategies, is that FFR was first measured across all lesions. If none of the lesions had an FFR ≤ 0.80, meaning none of the lesions was hemodynamically significant or likely to be responsible for symptoms or future events, then the patient was not included in the randomized study. This strategy excluded about a fourth of the patients who would not derived benefit from PCI. On the other hand, if at least one lesion in a major epicardial vessel had an FFR ≤ 0.80, then the patient was randomized to PCI versus medical therapy. In this manner, the population studied was enriched with patients with ischemia-producing lesions who would benefit most from PCI.
After enrolling about one-half of the target population of 1,600 patients, the independent data safety monitoring board strongly recommended stopping the trial because of a highly significant difference in the primary endpoint between the medical therapy group and the PCI group. There was no significant difference between death or myocardial infarction, but the need for hospitalization and urgent revascularization was significantly greater in the medical therapy arm (11.1% vs. 1.6%, p < 0.001). In addition, the FFR-guided PCI patients had significantly greater relief of angina. FAME 2 confirmed that stable patients with coronary disease who have significant ischemia do benefit from relief of their ischemia with PCI.
Limitations of FFR
FFR assumes that microvascular resistance remains constant. Therefore, in the culprit vessel of a patient with an acute ST segment myocardial infarction, FFR should not be utilized because a variable degree of transient microvascular stunning likely exists. In the acute setting, the maximum achievable hyperemic flow may be lower than it is a week later, after the microvascular stunning has resolved. Therefore, FFR in the culprit vessel might be overestimated. Multiple studies have shown that FFR can be accurately measured in the culprit vessel in the nonacute setting after ST segment myocardial infarction, as long as 3 to 6 days have passed [16].
It is important to note that FFR can be accurately measured in nonculprit vessels during the acute phase of ST segment elevation myocardial infarction [17]. These nonculprit vessels typically have intermediate lesions and invasively assessing them at the time of primary PCI can save time and resources and expedite decision making regarding the need for further PCI.
FFR has not been well-studied in patients with severe left ventricular hypertrophy. It is possible that in this setting the myocardium outgrows the microvasculature and requires a larger fraction of flow to avoid ischemia. For this reasons, the usual FFR cut-off value may not apply if there is severe left ventricular hypertrophy.
Another theoretical concern for a false negative FFR is exercise-induced vasoconstriction. A patient may have an intermediate coronary lesion, which itself is not flow-limiting. However, with exercise there may be vasoconstriction which increases the stenosis and results in myocardial ischemia. In the catheterization laboratory when FFR is measured with pharmacologic vasodilation, this exercise-induced vasoconstriction will be absent and the stenosis may not result in an ischemic FFR.
CONCLUSIONS
When invasively assessing coronary artery disease, the primary goal should be to determine whether the disease is causing a patient's symptoms and whether it is likely to cause future cardiac events. The presence of myocardial ischemia is our best gauge of whether a lesion is responsible for symptoms and likely to result in a future cardiac event. In the catheterization laboratory, FFR is the reference standard for identifying ischemia-producing lesions. Its spatial resolution is unsurpassed with it not only being vessel-specific, but also lesion-specific. There is now a wealth of data supporting the accuracy of measuring FFR to identify ischemia-producing lesions. FFR-guided PCI of these lesions results in improved outcomes and saves resources. Non-hemodynamically significant lesions can be safely managed medically with a low rate of subsequent cardiac events.
Notes
No potential conflict of interest relevant to this article is reported.