Role of 68Ga-DOTATOC PET/CT in the Evaluation of Primary Pulmonary Carcinoids
Article information
Abstract
Background/Aims
Although carcinoid tumors usually have good prognosis, early and specific diagnosis is important. Computed tomography and magnetic resonance imaging do not provide findings that are specific for carcinoids, and somatostatin receptor scintigraphy suffers from low spatial resolution. 18-Fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) has limited sensitivity for carcinoids due to low uptake of the marker. A PET/CT system that uses the somatostatin receptor-based PET tracer 1,4,7,10-tetraazacyclododecane-NI,NII,NIII,NIIII-tetraacetic acid (D)-Phe1-thy3-octreotide (68Ga-DOTATOC) has also been used in the evaluation of carcinoids, although information regarding its use for the detection of primary pulmonary carcinoids is limited. Thus, we investigated the value of 68Ga-DOTATOC PET/CT for the diagnosis of primary pulmonary carcinoid tumors.
Methods
This was a retrospective analysis of patients with primary pulmonary tumors who underwent 68Ga-DOTATOC PET/CT. All the patients had a histopathologic diagnosis of carcinoid. The rate of detection of primary pulmonary carcinoid tumors using 68Ga-DOTATOC PET/CT was assessed.
Results
Twenty patients were diagnosed as having carcinoid, and 19 tumors showed significant uptake on 68Ga-DOTATOC (detection rate, 95%). The maximal standardized uptake value (SUVmax) ranged from 1.1 to 66, with a median value of 21.6. In one patient, 68Ga-DOTATOC PET/CT revealed additional lesions.
Conclusions
Our results demonstrate that 68Ga-DOTATOC PET/CT is useful in the evaluation of primary pulmonary carcinoids and should be included in the diagnostic work-up of these patients.
INTRODUCTION
Carcinoid tumors, which were first described in 1888 by Lubarsch [1], represent 2% of all lung tumors [2]. While patients with carcinoids usually have a good prognosis, early and specific diagnosis is crucial. Various methods are used to diagnose pulmonary carcinoids, including tumor markers, computed tomography (CT), magnetic resonance imaging (MRI), somatostatin receptor scintigraphy (SRS), iodine-131-meta-iodobenzylguanidine scintigraphy, positron emission tomography (PET), and histopathologic examination. Tumor markers are not very sensitive for this purpose [3], CT and MRI do not give findings that are specific for carcinoids [4], and SRS suffers from low spatial resolution [5]. 18-Fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) usually shows low uptake of the marker by carcinoids, and thus has low sensitivity for this type of tumor [6-8].
PET/CT with 1,4,7,10-tetraazacyclododecane-NI, NII, NIII, NIIII-tetraacetic acid (D)-Phe1-thy3-octreotide (68Ga-DOTATOC PET/CT) has also been used to evaluate carcinoid tumors. Initial reports of its use have been encouraging, although data on the application of this system to diagnose pulmonary carcinoids are limited [9-11].
We applied 68Ga-DOTATOC PET/CT to 20 patients with primary pulmonary carcinoids, which is the largest series of patients to be analyzed in this way.
METHODS
A retrospective analysis of the 68Ga-DOTATOC PET/CT findings of patients with pulmonary tumors, performed at our institution during a span of 3 years, was done. Approval for this study was obtained from the institutional ethics committee, and the guidelines established by the committee were followed during the trial. All the patients gave written informed consent at the time of their clinical work-up. Consent was obtained from the parents or legal guardians for patients < 18 years of age. All the necessary precautions were taken to protect the identities of the patients in the study.
In total, 20 patients with pulmonary carcinoids were enrolled, and their medical records were analyzed. All the patients underwent a thorough clinical examination, hemogram, routine biochemistry, chest X-ray, contrast-enhanced CT (CECT) of the chest and upper abdomen, 68Ga-DOTATOC PET/CT, pulmonary function testing, and bronchoscopy, together with biopsy when feasible, followed by surgery (except for case 15). The tissues diagnosis involved histopathologic examination of either the biopsy or the surgical specimen. The detection rate of 68Ga-DOTATOC PET/CT for these tumors was calculated retrospectively.
68Ga-DOTATOC PET/CT protocol
PET scans were performed on a dedicated PET/CT scanner (Siemens Biograph 2; Siemens, Erlanger, Germany), using lutetium oxyorthosilicate (LSO; Lu2SiO5:Ce) detectors with attenuation coefficient of 0.89 cm-1, photo-fraction of 30%, and decay constant of 40 nanoseconds. The energy resolution at 511 KeV was 10, with spatial resolution of 6 mm. After fasting for at least 4 hours and verification of the serum glucose level, the patient was kept in a resting state in a quiet room, and 68Ga-DOTATOC PET/CT was performed 45 to 60 minutes after intravenous injection of 74 to 111 MBq of the radiotracer. CT acquisition was performed on a spiral dual slice CT with a slice thickness of 4 mm and a pitch of 1. The image was acquired using a matrix of 512 × 512 pixels, with a pixel size of about 1 mm. After the transmission scan, three-dimensional PET acquisition was carried out for 5 to 8 minutes per bed position. The PET data were acquired using a matrix of 128 × 128 pixels. CT-based attenuation correction of the emission images was employed.
The PET images were reconstructed through an iterative method of ordered subset expectation maximization (two iterations and eight subsets) using a 5-mm filter. After completion of PET acquisition, the reconstructed, attenuation-corrected PET images, CT images, and fused images of matching pairs of PET and CT images were available for review in the axial, coronal, and sagittal planes, as well as in maximum intensity projections and three-dimensional cine mode.
Two experienced nuclear medicine physicians, who were blinded to the structural imaging findings and clinical findings of the patients, evaluated the data independently. PET images were assessed for areas of increased radiotracer uptake. The corresponding areas in the CT images and fused PET/CT images were identified for corroboration. If the lesion showed a definite increase in DOTATOC accumulation compared with the background, it was interpreted as being visually positive for a viable tumor. For semi-quantitative analysis, a region of interest (ROI) was drawn around the site of abnormal uptake in the consequent four to six PET/CT slices. The slice that showed maximal uptake in the ROI was chosen for quantitative measurement of metabolic activity/uptake of the tracer (SUV). From these ROIs, the SUVmax was calculated according to the formula:
SUVmax = ROI (at the pixel with maximum uptake, MBq/g) / (injected dose, MBq / body weight, g).
RESULTS
The study involved 20 patients (11 males and nine females) with a mean age of 32.7 years (range, 16 to 53). The patients' characteristics and the structural imaging and 68Ga-DOTATOC PET/CT findings are summarized in Table 1.
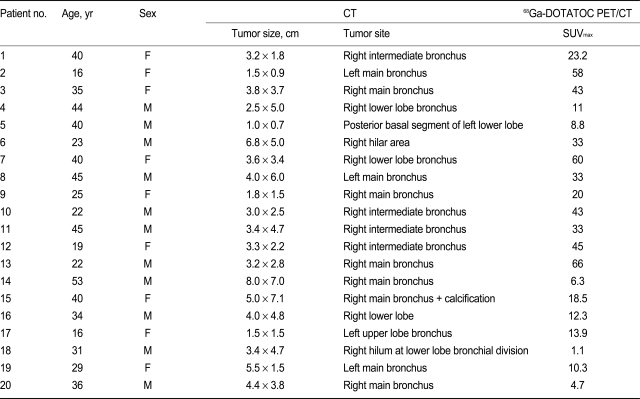
Patients' characteristics and results of structural imaging and 68Ga-DOTATOC PET/CT imaging
Among the patient, cough was the commonest symptom (n = 19), followed by expectoration (n = 17), hemoptysis (n = 14), dyspnea (n = 7), and chest pain (n = 4). One patient had Cushing's syndrome (case 5).
Chest X-rays revealed either collapse or opacity in 19 patients, and the findings were normal in one patient (case 5). CECT of the chest revealed the primary lesion in every patient. All the lesions exhibited contrast enhancement. No additional lesions were found in any patient. Most of the tumors were detected on the patient's right side (n = 15).
68Ga-DOTATOC PET/CT, by virtue of its CT component, revealed all the lesions anatomically. Overall, 19/20 tumors showed significant uptake of 68Ga-DOTATOC, giving visual positivity and a SUVmax value > 2.5. Thus, the detection rate for 68Ga-DOTATOC PET/CT was 95%. The median SUVmax value was 21.6 (range, 1.1 to 66.0). The lowest SUVmax value for tumors with significant uptake of the radiotracer was 4.7.
Of the 20 patients, 13 had typical carcinoid tumors, and seven had atypical carcinoid tumors. All the typical carcinoids showed significant uptake of Ga-68 DOTATOC. One atypical carcinoid lacked any significant uptake of Ga-68 DOTATOC (case 18). The typical carcinoids also showed significantly higher levels of Ga-68 DOTATOC uptake than the atypical carcinoids. In one patient (case 15), 68Ga-DOTATOC PET/CT facilitated the detection of additional lesions, which showed significant radiotracer uptake, in the mediastinal lymph nodes, pancreas, thyroid, and pituitary, none of which was identified in the conventional CT. Biopsies of the mediastinal lymph nodes confirmed the presence of metastatic deposits of the carcinoid tumor.
DISCUSSION
Pulmonary carcinoids are usually detected in structural imaging systems such as CT or MRI, which detect a space-occupying lesion. However, because these techniques do not provide information on the specific characteristics that would allow unambiguous identification of the tumor as carcinoid, they have low specificity [4]. Functional imaging has been used in the work-up of patients with carcinoids. 18F-FDG PET/CT suffers from low sensitivity due to low uptake of the tracer by carcinoids, which is related to their poor metabolism. Rege et al. [6] evaluated a patient with a pulmonary carcinoid and history of ectopic adrenocorticotrophic hormone secretion using 18F-FDG PET; the lesion was found to be hypometabolic for 18F-FDG. Erasmus et al. [7] evaluated seven cases of pulmonary carcinoids using 18F-FDG PET and found that three of these patients were visually negative, three patients were hypometabolic and were erroneously categorized as benign nodules, and one patient was visually positive. Kruger et al. [8] evaluated pulmonary carcinoids in 13 patients and found that 6/12 (50%) had typical carcinoids with SUVmax < 2.5.
DOTATOC has high affinities for SSR2 and SSR3 and lower affinity for SSR5. 68Ga-DOTATOC PET/CT has been shown to be highly accurate in the diagnosis of neuroendocrine tumors, meningiomas, thyroid malignancies, and prostatic cancers. It has also been used successfully to evaluate primary lung cancers, particularly the small-cell form. The high resolution of PET enables high detection rates for small tumors. As with most investigative tools, DOTATOC PET/CT also has limitations. It can theoretically show positivity for non-tumor tissues, such as those in the pancreas (especially the uncinate process), in the pituitary gland, and in chronic inflammatory conditions (e.g., granulomatous diseases and sarcoidosis). Nonetheless, this technique represents an advance in diagnostic oncology.
Because carcinoid tumors are rich in somatostatin receptors (SSR), they typically show high-level uptake of 68Ga-DOTATOC. Although various studies have demonstrated the utility of 68Ga-DOTATOC PET/CT in the evaluation of carcinoids, little information is available on the use of this tool for pulmonary carcinoids, especially primary carcinoids in the lungs. The value of 68Ga-DOTATOC PET/CT for the diagnosis of primary pulmonary carcinoids remains to be established due to the lack of specific studies.
Hofmann et al. [9] compared the diagnostic values of 111In-octreotide scintigraphy and 68Ga-DOTATOC PET to morphologic imaging in eight patients with histologically proven metastatic carcinoid tumors (six abdominal and two bronchial carcinoids). 68Ga-DOTATOC PET identified all the lesions, whereas 111In-octreotide scintigraphy identified only 85% of the lesions. Koukouraki et al. [10] used 68Ga-DOTATOC PET to evaluate 15 cases of carcinoid tumors, including two cases of pulmonary carcinoids, and reported an overall sensitivity of 92%. Gabriel et al. [11] used 68Ga-DOTATOC PET to evaluate 84 patients with neuroendocrine tumors, including five patients with bronchial carcinoids, and reported a sensitivity of 97%, specificity of 92%, and an overall accuracy of 96%. These results were far superior to those obtained using SPECT or CT.
Other 68Ga-labeled peptides with profiles similar to that of 68Ga-DOTATOC have been used to evaluate pulmonary carcinoids. Ambrosini et al. [12] evaluated 11 patients with bronchial carcinoids using PET/CT with 68Ga-DOTANOC (1,4,7,10-tetraazacyclododecane-NI,NII,NIII,NIIII-tetraacetic acid-1-Nal3-octreotide). There were no false-positive findings, and 68Ga-DOTANOC PET/CT detected more lesions than did CT (37 vs. 21). Kayani et al. [13] evaluated 18 patients with pulmonary neuroendocrine tumors using PET/CT with 68Ga-DOTATATE (1,4,7,10-tetraazacyclododecane-NI,NII,NIII,NIIII-tetraacetic acid (D)-Phe1-thy3-octreotate) and 18F-FDG PET/CT; they detected 11 cases of typical carcinoid, two cases of atypical carcinoid, two cases of diffuse idiopathic pulmonary neuroendocrine hyperplasia, one small-cell neuroendocrine tumor, one large-cell neuroendocrine tumor, and one case of adenocarcinoma with neuroendocrinal differentiation. They found that the majority of the carcinoids showed significant uptake of 68Ga-DOTATATE.
In the present study, all the patients presented with a primary tumor. There was significant uptake of 68Ga-DOTATOC in 19/20 patients (detection rate of 95%), and these findings corroborated the diagnosis of carcinoid. The findings for a typical positive case are shown in Fig. 1. Case 5 had symptoms of Cushing's syndrome. CT demonstrated a small, suspicious-looking lesion in the left lower lobar parenchyma, but the finding was not conclusive. Obtaining a biopsy was not possible owing to the small size of the lesion. 68Ga-DOTATOC uptake by the lesion was high, supporting the diagnosis. Excision of the lesion resulted in a complete clinical response for this patient. The results obtained with CECT and 68Ga-DOTATOC PET/CT were concordant with respect to the primary lesions. CECT did not reveal any lesions other that the primary tumor in any of the patients. 68Ga-DOTATOC PET/CT detected additional lesions in case 15 (Fig. 2) and facilitated tumor staging, prognostication, and decisions as to the choice of treatment offered to this patient. The tumor, which did not show any significant uptake of 68Ga-DOTATOC, was defined as an atypical carcinoid (case 18). Atypical carcinoids are known to exhibit low-level differentiation and decreased somatostatin receptor expression, which may explain the lack of uptake on 68Ga-DOTATOC PET/CT [13].

CT (A), 68Ga-DOTATOC PET whole-body projection image (B) and fused 68Ga-DOTATOC PET/CT image (C) for case 3, showing intense uptake of the tracer by the tumor (arrow). The SUVmax value is 43. SUVmax, maximal standardized uptake value.

Whole-body projection image (A) and fused PET/CT images (B-D) for case 15 using 68Ga-DOTATOC PET and showing tracer uptake by the thyroid (B, arrow), superior-mediastinal node (C, dotted arrow) and pancreas (D, bolded arrow).
The present study, which is the largest conducted to date for the evaluation of primary pulmonary carcinoids, reveals that 68Ga-DOTATOC PET/CT has a high detection rate for primary pulmonary carcinoids. Although histopathology remains the confirmatory modality, 68Ga-DOTATOC PET/CT can provide highly useful guidance during the evaluation of patients with pulmonary masses, as compared with conventional investigative modalities. If the tumor shows uptake on 68Ga-DOTATOC PET/CT, there is a high likelihood that it is carcinoid. Thus, the clinician may be helped in resolving a dilemma that is often encountered during the diagnosis of pulmonary masses.
As 68Ga-DOTATOC PET/CT provides both anatomical information (by virtue of the CT component) and information on the functional status of the tumor (by virtue of the PET component), the need to perform a separate CECT is eliminated. 68Ga-DOTATOC PET/CT also facilitates proper staging and planning of the treatment modality to be offered to the patient. Moreover, based on the results of the present study, it is superior to CECT. 68Ga-DOTATOC PET/CT can also be used to plan eventual targeted radionuclide therapies and may help in the selection of patients who are likely to benefit from radio-immunotherapy with 177Lu- or 90Y-labeled DOTATOC [10].
Therefore, 68Ga-DOTATOC PET/CT represents an important component of the diagnostic work-up for patients with pulmonary carcinoids and should be used more widely.
Notes
No potential conflict of interest relevant to this article was reported.