The Clinical Usefulness of Serum Fructosamine and HbAlc in Patients with NIDDM
Article information
Abstract
To evaluate the clinical values of serum fructosamine and HbAlc, serum fructosamine and HbAlc were assessed in 50 normal controls and 36 patients with NIDDM (non-insulin-dependent diabetes mellitus). And we studied 10 patients selected at random among the 36 patients with NIDDM.
The values of serum fructosamine and HbAlc in controls were 2.1 mmol/L and 5.3%, respectively. The levels of serum fructosamine and HbAlc were significantly higher in NIDDM patients (3.27 mmol/L and 8.8%, respectively, p<0.005) compared with those in the controls. The serum fructosamine was significantly correlated with fasting plasma glucose and HbAlc (r=0.78, p<0.78, p<0.001; r=0.76, p<0.005, respectively). Also, in retrograde study, serum fructosamine concentration had a significant correlation to fasting plasma glucose determined 2 weeks before (r=0.72, p<0.002), and 4 weeks before (r=0.54, p<0.005).
It is concluded that serum fructosamine measurement may be useful in monitoring short-term control of plasma glucose in patients with NIDDM.
INTRODUCTION
Diabetes mellitus is a universal health problem and may occur at any age.2) The traditional biochemical measurements for initially detecting patients with diabetes mellitus are random estimations of blood and urine glucose concentration. Despite their common use, both tests are nonspecific, being influenced by a wide variety of drugs and conditions.3,4,5)
Measurement of the glycosylated hemoglobin concentration in random blood specimens is a simpler screening test for diabetes6,7) and has the advantage that it reflects blood glucose control under physiologic conditions.8) And it is an accepted method for assessing long-term diabetic control.9,10)
Since the measurement of fructosamine as an index of diabetic control was first published by Johnson (1982),12) Baker et1) al.,10,13) Jerntorp et al.11) and other investigators14,15,17) have reported that fructosamine concentrations were correlated with HbAlc and other measures of glycemia, and fructosamine appeared more useful than HbAlc for monitoring short-term changes of glycemia.
The present study was undertaken to determine the clinical usefulness of fructosamine estimations in monitoring short-term glycemic control during the management of patients with NIDDM.
MATERIALS AND METHODS
Serum fructosamine, fasting plasma glucose and HbAlc were measured in 50 normal controls and 36 patients with NIDDM. We studied four men and six women selected at random among the 36 patients with NIDDM, aged 21–73 years (median 47), who had been admitted to our hospital from Nov. 1988 to March 1989.
Table 1 summarizes the clinical details of patients. All patients had normal liver and renal function and normal hematologic profiles. Three patients have been associated with peripheral neuropathy and four patients had retinopathy (Table 1).
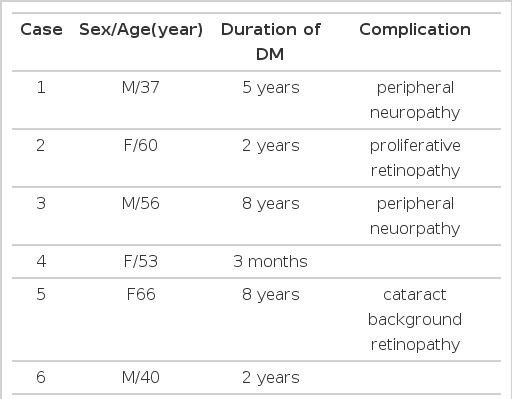
Clinical Details of Patients (M:4, F:6)
References for serum fructosamine, fasting plasma glucose and HbAlc values were determined in 50 non-diabetic volunteers aged 20–65 years (median 43). Diabetes was excluded from this reference population using the fasting plasma glucose, postprandial 2 hour glucose and urinary glucose results. The patients studied were on a diet regimen and had taken oral hypoglycemic agents or insulin injection. In these patients, fasting plasma glucose, serum fructosamine and HbAlc were measured on admission and at biweekly intervals to 8 weeks.
Fructosamine was measured using an ABBOTT VP automated analyzer by colourimetric test based on the ability of ketoamines to reduce nitroblue tetrazolium in alkaline medium (Fructosamine test, Roche). HbAlc was measured by a mini-column method using a Perkin-Elmer Junior model 35 spectrophotometer.
RESULTS
The range of values for serum fructosamine in controls was 1.7–2.6 mmol/L (mean 2.1 mmol/L). Fasting plasma glucose concentrations in the same subjects were 70–109 mg/dl (mean 90 mg/dl) and HbAlc values were 4.4–6.4% (mean 5.3%), which are compatible with normal ranges of other laboratory criteria. Fasting plasma glucose concentrations in patients with NIDDM were 174–374 mg/dl (mean 235 mg/dl). The levels of serum fructosamine and HbAlc were significantly higher in NIDDM patients (2.4–4.5 mmol/L: mean 3.27 mmol/L, 7.2–12.5%: mean 8.8%, respectively, p<0.005) compared with those in the normal controls (Table 2).

Serum Fructosamine & HbAlc Values in Normal Controls and NIDDM Patients
The correlation of serum fructosamine to fasting plasma glucose and to HbAlc was examined in normal controls and diabetic patients. The serum fructosamine was significantly correlated with fasting plasma glucose and HbAlc. Correlation coefficients were 0.78 and 0.76 respectively and p values indicate statistical significance (p<0.001, p<0.005 respectively) (Table 3, Fig. 1).
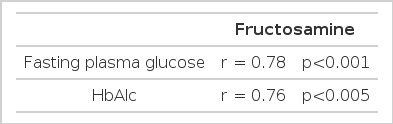
Correlation of Serum Fructosamine to fasting Plasma Glucose and to HbAlc
Correlation of serum fructosamine to fasting plasma glucose and HbAlc (r: correlation coefficient)
Also, in ten patients studied, retrograde assessment for the correlation of serum fructosamine to fasting plasma glucose was periodically performed after management of diabetes for 8 weeks. The serum fructosamine concentration had a significant correlation to the fasting plasma glucose level determined 2 weeks before (r = 0.72, p<0.002) and 4 weeks before (r = 0.54, p<0.005), but there were no significant correlations to the fasting plasma glucose levels 6 weeks before (r = 0.16, NS) and 8 weeks before (r = 0.18, NS) (Table 4).

Retrograde Study for Correlation of Serum Fructosamine to fasting Plasma Glucose After Management of DM for 8 Weeks
We studied the changes and regression rates of fasting plasma glucose, serum fructosamine and HbAlc during the management of diabetes for 8 weeks. Hyperglycemia was well controlled with symptomatic improvement, without newly developed complications including hypoglycemia. Fig. II indicates that the change of serum fructosamine shows a sharper downward slope than that of HbAlc until 6 weeks (Fig. 2).
The changes of fasting plasma glucose, serum fructosamine and HbAlc during the management of DM for 8 weeks.
The regression rates of serum fructosamine increased more than those of HbAlc at 2 weeks, 4 weeks and 6 weeks (17.5%, 22% and 21%; 10%, 9.8% and 16%, respectively). That is to say, until 6 weeks, serum fructosamine decreased more sensitively than HbAlc. Conversely, at 8 weeks, HbAlc decreased more sensitively than serum fructosamine (Table 5, Fig. 3).

Regression Rates of Serum Fructosamine and HbAlc

Regression rates of serum fructosamine and HbAlc
DISCUSSION
While the value of plasma glucose measurement at standard times throughout the day is established as a guide to modifying treatment, an accurate measure of mean blood glucose concentrations over several days or weeks would prove extremely useful in judging overall diabetic control and the response to changes in management.18) Fructosamine provides such a measurement, reflecting mainly the basal or fasting plasma glucose concentration with little contribution from transient postprandial hyperglycemia.1)
Measurement of the glycosylated hemoglobin concentration is an accepted method for assessing long-term diabetic control,19,20) Many studies reported that fructosamine, as an index of short-term diabetic control, correlated with HbAlc and other measures of glycemia and appeared more useful than HbAlc for monitoring short-term changes.1,10–15,17) Other previous reports showed that the fasting plasma glucose concentration varies in response to stress or exercise, urinary glucose is modified by the renal threshold, the HbAlc value depends on red cell turnover and fructosamine is influenced by alterations in serum protein metabolism.1,10)
In this study, all patients had normal liver and renal function and normal hematologic profiles.
In controls, serum fructosamine and HbAlc levels were compatible with normal ranges of other laboratory criteria. Serum fructosamine and HbAlc levels were significantly higher in NIDDM patients compared with those in normal controls and serum fructosamine was significantly correlated with fasting plasma glucose and HbAlc.
Also, in retrograde study, serum fructosamine concentration had a significant correlation to fasting plasma glucose determined 2 weeks before and 4 weeks before. In patients, hyperglycemia was well controlled with improved symptoms, without newly developed complications including hypoglycemia. During the management of diabetes for 8 weeks, serum fructosamine decreased more sensitively than HbAlc until 6 weeks. Conversely, at 8 weeks, HbAlc decreased more sensitively than serum fructosamine.
With these results, we believe that serum fructosamine and HbAlc measurement may be helpful in screening for diabetes mellitus, and serum fructosamine measurement may be useful in monitoring short-term control of plasma glucose in patients with NIDDM.
Further more, as an ongoing study, we will continue to monitor the serum fructosamine and HbAlc levels in patients with NIDDM.