Clinical outcomes of esophageal squamous cell carcinoma in patients aged over 80 years
Article information

Abstract
Background/Aims
The clinical outcomes and optimal treatment of esophageal squamous cell carcinoma (ESCC) in elderly patients are unclear. This study aimed to assess the clinical outcomes of ESCC in patients aged ≥ 80 years.
Methods
Medical records of patients diagnosed with ESCC between December 2008 and February 2024 were retrospectively reviewed. In total, 479 patients with ESCC were included and divided into the elderly (n = 52) and younger (n = 427) groups based on age. The clinical outcomes and survival rates, according to treatment, were compared between the two groups.
Results
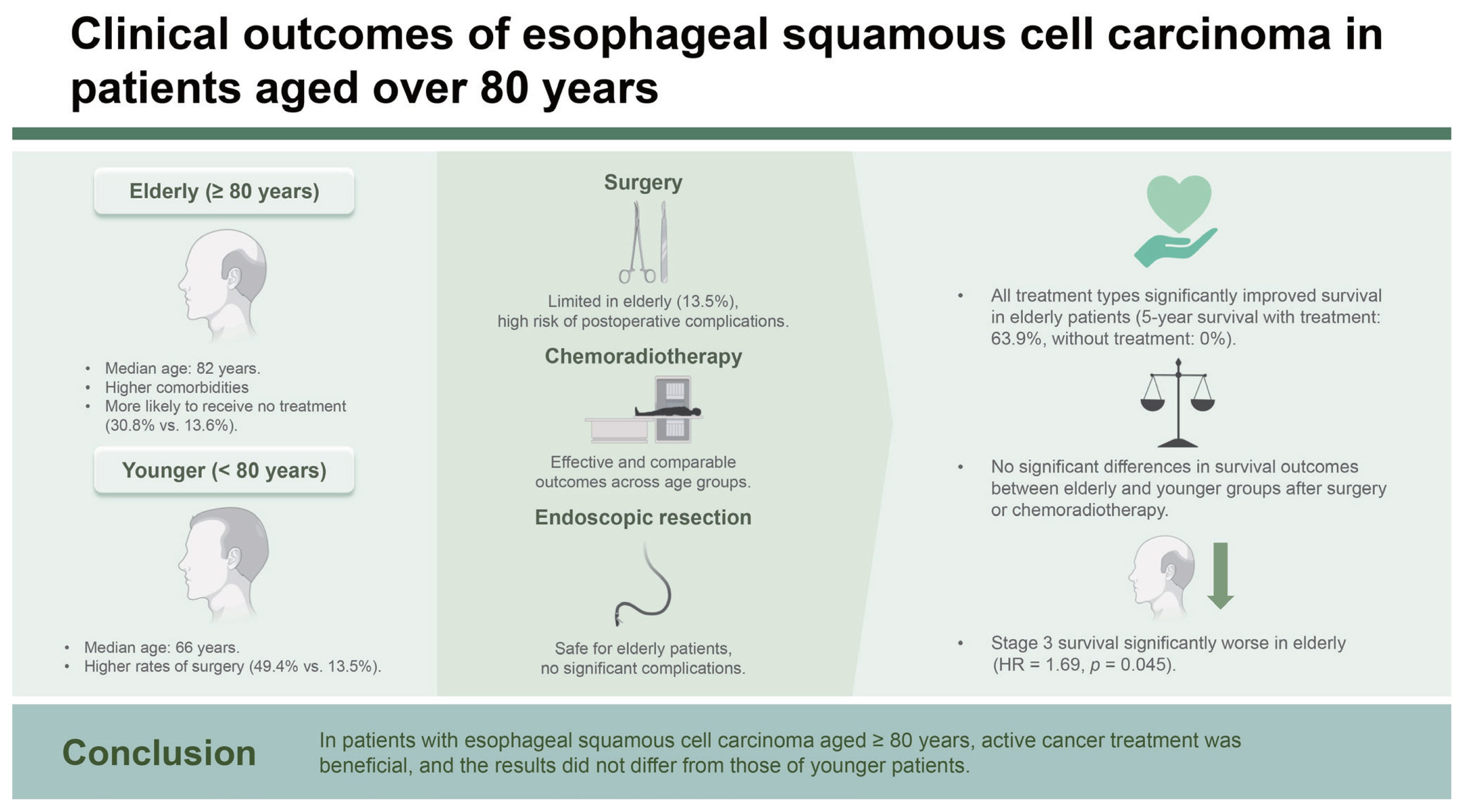
The median ages of the two groups were 82 years (range, 80–95 yr) and 66 years (41–79 yr). The overall survival was slightly lower in the elderly group; however, no statistical significance (hazard ratio [HR] 1.27, 95% confidence interval [CI] 0.85–1.91; p = 0.238) was observed. No differences were observed in the outcomes or survival between the two groups according to the treatment method (surgery, chemoradiotherapy or radiotherapy alone, and endoscopic resection). The elderly group was more likely to receive no treatment for cancer (30.8% vs. 13.6%, p = 0.002) than the younger group. However, when there was no treatment for cancer in the elderly group, survival was significantly lower than when treatment was administered (HR 0.08, 95% CI 0.03–020; p < 0.001).
Conclusions
In patients with ESCC aged ≥ 80 years, active cancer treatment was beneficial, and the results did not differ from those of younger patients.
INTRODUCTION
As life expectancy gradually increases worldwide, the number of elderly patients with cancer is also increasing, creating a burden. It is difficult for elderly patients with cancer to choose a treatment method, and they sometimes worry about whether to treat or not. The standard age for the elderly has gradually increased, and currently, the American Geriatrics Society defines an “older person” as being 75 years or older [1]. Moreover, as the number of elderly individuals with good general condition has increased, the number of elderly cancer patients receiving treatment has also increased.
Esophageal cancer is a representative cancer that occurs in the elderly and has a poor prognosis [2]. Recently, the peak incidence of esophageal cancer has moved to the 70s [3]. The main histological types of esophageal cancer are squamous cell carcinomas (SCCs) and adenocarcinomas (ACs). Although the prevalence of AC is increasing, SCC remains the most common histological type worldwide and is overwhelmingly prevalent in East Asia, including South Korea [4–6]. Some studies have been conducted on esophageal cancer in the elderly, but SCC has not been separately analyzed in patients aged ≥ 80 years. Therefore, this retrospective observational study aimed to identify clinical outcomes and survival of patients aged ≥ 80 years with esophageal squamous cell carcinoma (ESCC).
METHODS
Patients
The medical records of patients with esophageal cancer treated between December 2008 and February 2024 at Pusan National University Yangsan Hospital were reviewed. In total, 479 patients with histologically confirmed ESCC who underwent follow-up were included in the study. The patients were divided into elderly and younger groups based on age (80 yr). Esophageal cancer was staged according to the American Joint Committee on Cancer staging system, revised 8th edition [7]. The Eastern Cooperative Oncology Group (ECOG) performance status scale and comorbidities of all patients were investigated. The Charlson comorbidity index was measured based on the patients’ comorbidities [8]. All patients in this study had cancer; therefore, the standard for high-risk mortality patients was set at an index of 7. This study was approved by the Ethics Committee of Pusan National University Yangsan Hospital (Institutional Review Board no. 55-2024-065). The requirement for informed consent was waived because the participants’ medical records were anonymized before the analysis.
Surgery
Patients selected for surgery underwent Ivor Lewis esophagectomy with intrathoracic anastomosis and two- or three-field lymph node dissection if there were no anatomical abnormalities. Patients with anatomical abnormalities, such as gastrectomy, underwent colonic or jejunal interposition. Pathological analysis was used to evaluate resection completeness (R0) and lymph node metastasis. Anastomotic leakage was assessed 1 week after surgery using endoscopy and esophagography. Postoperative mortality was defined as mortality within 30 days of surgery or during postoperative hospitalization.
Chemoradiotherapy or radiotherapy alone
Chemoradiotherapy (CRT) was categorized as definitive CRT, performed with curative intent, or neoadjuvant CRT before surgery. Depending on their condition, some patients received definitive radiation therapy (RT), while others underwent palliative RT only for symptom relief. The RT schedules and doses were as follows: (1) Definitive CRT, 2 Gy × 25 fractions for 50 Gy; (2) neoadjuvant CRT, 1.8 Gy × 25 fractions for 45 Gy; and (3) palliative RT, 3 Gy × 10 fractions for 30 Gy. The chemotherapy regimens used for most patients were cisplatin/5-fluorouracil (cisplatin 75 mg/m2 for 1 day and 5-fluorouracil 750 mg/m2/d for 4 days at weeks 1 and 5) or paclitaxel/carboplatin (paclitaxel 50 mg/m2 and carboplatin area under the curve of 2 mg/mL/min on day 1 weekly over 5 weeks).
Endoscopic resection
Some superficial esophageal cancers without evidence of lymph node metastasis on preoperative examination and localized to the mucosa on endoscopic ultrasound were treated with endoscopic resection. Most patients underwent endoscopic submucosal dissection (ESD), and most procedures were conducted under conscious sedation via intravenous midazolam without general anesthesia. If no complications occurred, the patient was discharged 2 days after the procedure. A complete resection was defined as a single-piece resection without fragmentation and tumor-free margins during histological examination. Curative resection was defined as complete resection without submucosal invasion, lymphovascular involvement, or poorly differentiated features of the resected specimen.
Follow-up after treatment
After curative treatment (surgery, definite CRT, or endoscopic resection), endoscopy and chest/abdominal computed tomography (CT) were performed 2–3 months later, every 3 months for the first year, and every 6 months thereafter. Positron emission tomography (PET) was not conducted after surgery or endoscopic resection but was conducted 3–6 months after definitive CRT. Typically, surgery is performed within 2 months after the completion of neoadjuvant CRT; however, some patients are observed without surgery according to the results of the preoperative examination and their condition through a multidisciplinary approach. Clinically, complete response (cCR) after CRT was defined as no evidence of cancer in examinations performed 2–3 months after completing CRT, including endoscopy, endoscopic biopsy, chest/abdominal CT, and PET. For ambiguous examination results due to esophagitis or ulcers following CRT, the examinations were repeated after 2–3 months.
Statistical analysis
Categorical variables are presented as number (%), and continuous variables are presented as median (range). Student’s t-test and chi-square test and/or Fisher’s exact test were used to analyze continuous and categorical variables, respectively, for in-group comparisons. The Kaplan–Meier method was used to estimate survival, and the log-rank test was used to determine significant differences between groups. A Cox regression model was used to estimate the hazard ratio (HR) associated with survival. Statistical significance was set at p < 0.05. The Statistical Package for the Social Sciences version 27.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
RESULTS
Characteristics of the patients
During the study period, 479 patients with histologically confirmed ESCC, were identified and divided into the elderly and younger group. The median age of the patients was 69 years (range, 41–95 yr). The median follow-up period for the patients was 17 months (range, 1–182 mo). The older and younger age groups included 52 and 427 patients, respectively. The median ages of the two groups were 82 years (range, 80–95 yr) and 66 years (41–79 yr), respectively. No differences were observed in sex, tumor location, or cancer stage between the two groups. The elderly group was more likely to receive no treatment for cancer (30.8% vs. 13.6%, p = 0.002). The elderly group was less likely to undergo surgery than the younger group (13.5% vs. 49.4%, p < 0.001) and preferred CRT or radiotherapy alone (36.5% vs. 21.1%, p = 0.014). None of the patients received chemotherapy alone in the elderly group. The elderly group had higher ECOG performance status scale scores and more comorbidities. A Charlson comorbidity index of 7 or higher was significantly more prevalent in the elderly group (21.2% vs. 7.3%, p = 0.002). The baseline characteristics between the two groups are summarized in Table 1.

Baseline characteristics of patients
Surgery
A total of 218 patients underwent surgery, with seven in the elderly group and 211 in the younger group. The median age of the patients in the elderly group who underwent surgery was 82 years, and all patients were male. All patients in the elderly group underwent esophagogastric anastomosis, and most tumors were located in the lower thoracic esophagus (71.4%). In the elderly group, none of the patients received neoadjuvant CRT; however, R0 resection was performed in all patients. No significant difference was found in the postoperative pathological stage between the groups. No significant difference was observed in anastomotic leakage (14.3% vs. 9.5%, p = 0.674) or postoperative mortality (14.3% vs. 10.4%, p = 0.745) between the groups. The incidence of anastomotic strictures did not differ between the two groups (14.3% vs. 16.1%, p = 0.897). In the younger group, 16 patients were classified as stage IV based on surgical results showing that the cancer had invaded adjacent organs or major blood vessels or had 7 or more lymph node metastases. A comparison of the two groups of patients who underwent surgery is summarized in Table 2.

Comparison of the two groups that underwent surgery
CRT
A total of 109 patients underwent CRT or RT alone, 19 in the elderly group and 90 in the younger group. No significant differences were observed in sex, cancer location, or chemotherapy regimen between the groups. Stage 3 patients were more in the elderly group (73.7% vs. 38.9%, p = 0.009). All patients in the elderly group were administered reduced doses of chemotherapy. The proportions of patients who underwent RT alone (31.6% vs. 15.6%, p = 0.109) and the proportions of patients who did not complete the CRT schedule because of side effects (10.5% vs. 8.9%, p = 0.822) were higher in the elderly group; however, the difference was not statistically significant. Two patients in the younger group died during the CRT. The achievement of cCR after CRT was similar in both groups (47.4% vs. 51.1%, p = 0.767), and no differences were observed between the stages. Among patients who achieved cCR, four in the non-elderly group experienced cancer recurrence during follow-up, resulting in three deaths and one receiving supportive care. The incidence of radiation-induced strictures did not differ between the two groups (15.8% vs. 10.0%, p = 0.468). A comparison between the two groups of patients who underwent CRT, including RT alone, is summarized in Table 3.

Comparison of the two groups that underwent chemoradiotherapy including radiotherapy alone
Endoscopic resection
Fifty-seven patients underwent endoscopic resection: 10 in the elderly and 47 in the younger groups. No differences were observed in sex or lesion location between the two groups, and most lesions were removed using ESD (80.0% in the elderly group and 93.6% in the younger group). The procedure time (median, 29 vs. 22 min, p = 0.715) and hospitalization duration (median, 4 vs. 4 days, p = 0.408) did not differ between the two groups. Postprocedural complications (one hemorrhage and one perforation) occurred only in the elderly group. No deaths were associated with endoscopic resection. The complete resection (80.0% vs. 80.9%, p = 0.951) and curative resection (60.0% vs. 66.0%, p = 0.720) rates did not differ between the groups. None of the patients in the elderly group received additional treatment even after non-curative resection. Of the 16 patients who underwent non-curative resection in the younger group, three underwent additional esophagectomy, and six underwent RT. During follow-up, no significant difference was observed in stricture occurrence (20.0% vs. 6.4%, p = 0.190) between the two groups. One case of local recurrence occurred in each group after endoscopic resection. The patient in the elderly group was cured with RT, and the patient in the younger group was cured with ESD again. A comparison between the two groups of patients who underwent endoscopic resection is summarized in Table 4.

Comparison of the two groups that underwent endoscopic resection
Survival
The median follow-up period was 11 months (range, 1–104 mo) for the elderly group and 19 months (range, 1–182 mo) for the younger group. Of the surviving patients (25 elderly and 211 younger), the median follow-up duration was 23 months (range, 3–104 mo) for elderly patients and 60 months (range, 5–182 mo) for younger patients.
Overall, patient survival was lower in the elderly group but not statistically different (HR 1.27, 95% confidence interval [CI] 0.85–1.91; p = 0.238) (Fig. 1A). Cancer-specific survival was worse in the elderly group; however, there was no statistical significance (HR 1.42, 95% CI 0.95–2.12; p = 0.084) (Fig. 1B). Survival after surgery (HR 1.37, 95% CI 0.43–4.33; p = 0.597) or CRT including RT alone (HR 0.86, 95% CI 0.41–1.82; p = 0.691) was similar between the two groups (Fig. 1C, D). No deaths were noted among the patients who underwent endoscopic resection in either group. The overall survival rates at 1, 3, and 5 years were 49.8%, 41.6%, and 41.6%, respectively, in the elderly group, and 64.4%, 50.2%, and 49.4%, respectively, in the younger group. The overall survival rates at 1, 3, and 5 years postoperatively were 50.0%, 50.0%, and 50.0%, respectively, in the elderly group and 82.0%, 62.2%, and 60.9%, respectively, in the younger group. The overall survival rates after CRT or RT alone at 1, 3, and 5 years were 62.3%, 44.5%, and 44.5%, respectively, in the elderly group and 59.2%, 45.9%, and 44.2%, respectively, in the younger group.
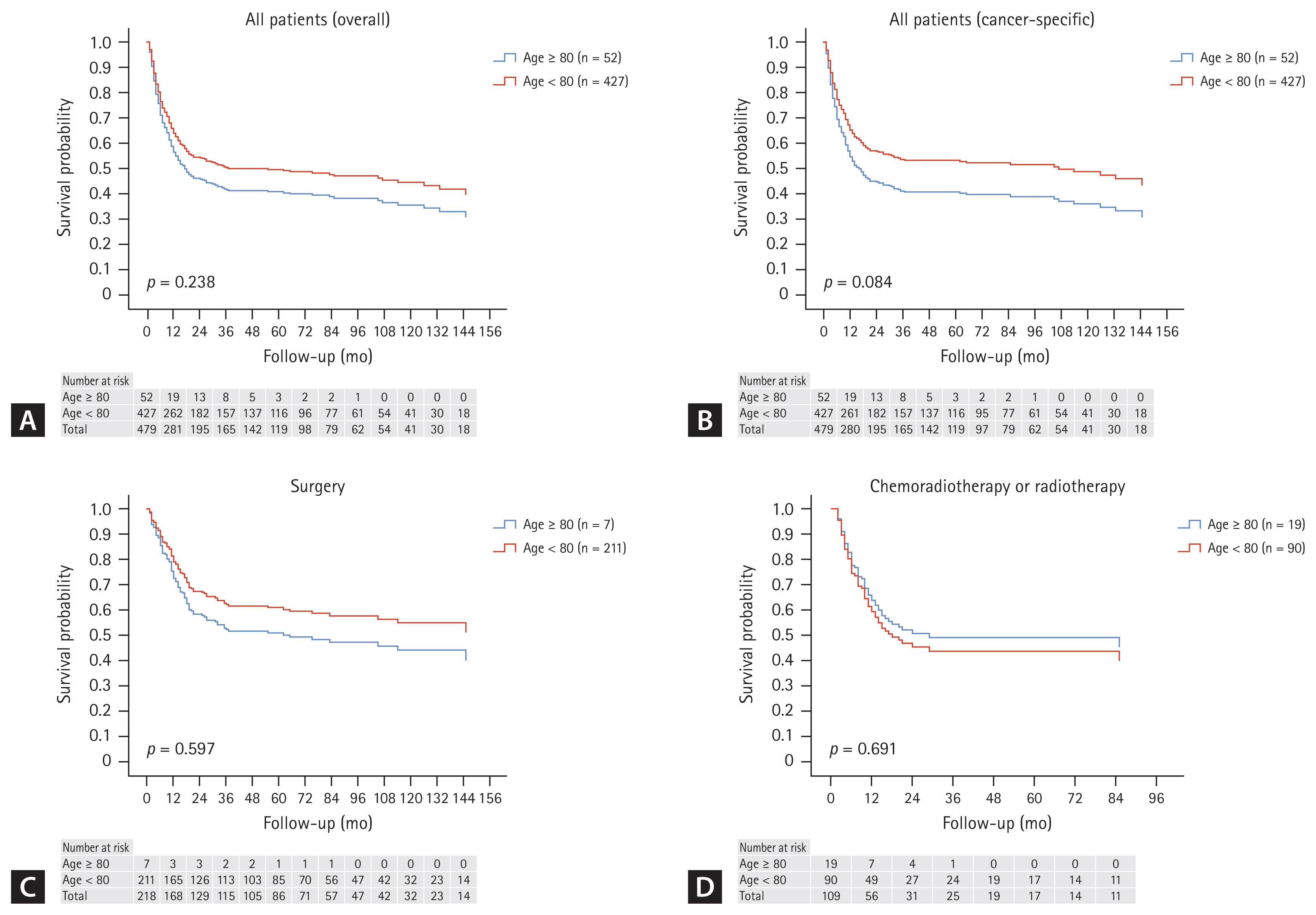
Overall survival curves between the two groups. (A) Overall survival between the two groups for all patients. (B) Cancer-specific survival between the two groups for all patients. (C) Survival between the two groups after surgery. (D) Survival between the two groups after chemoradiotherapy.
Figure 2 shows the comparison of survival according to stage between the two age groups. Except for stage 3 (HR 1.69, 95% CI 1.01–2.83; p = 0.045), the two groups did not differ in survival.
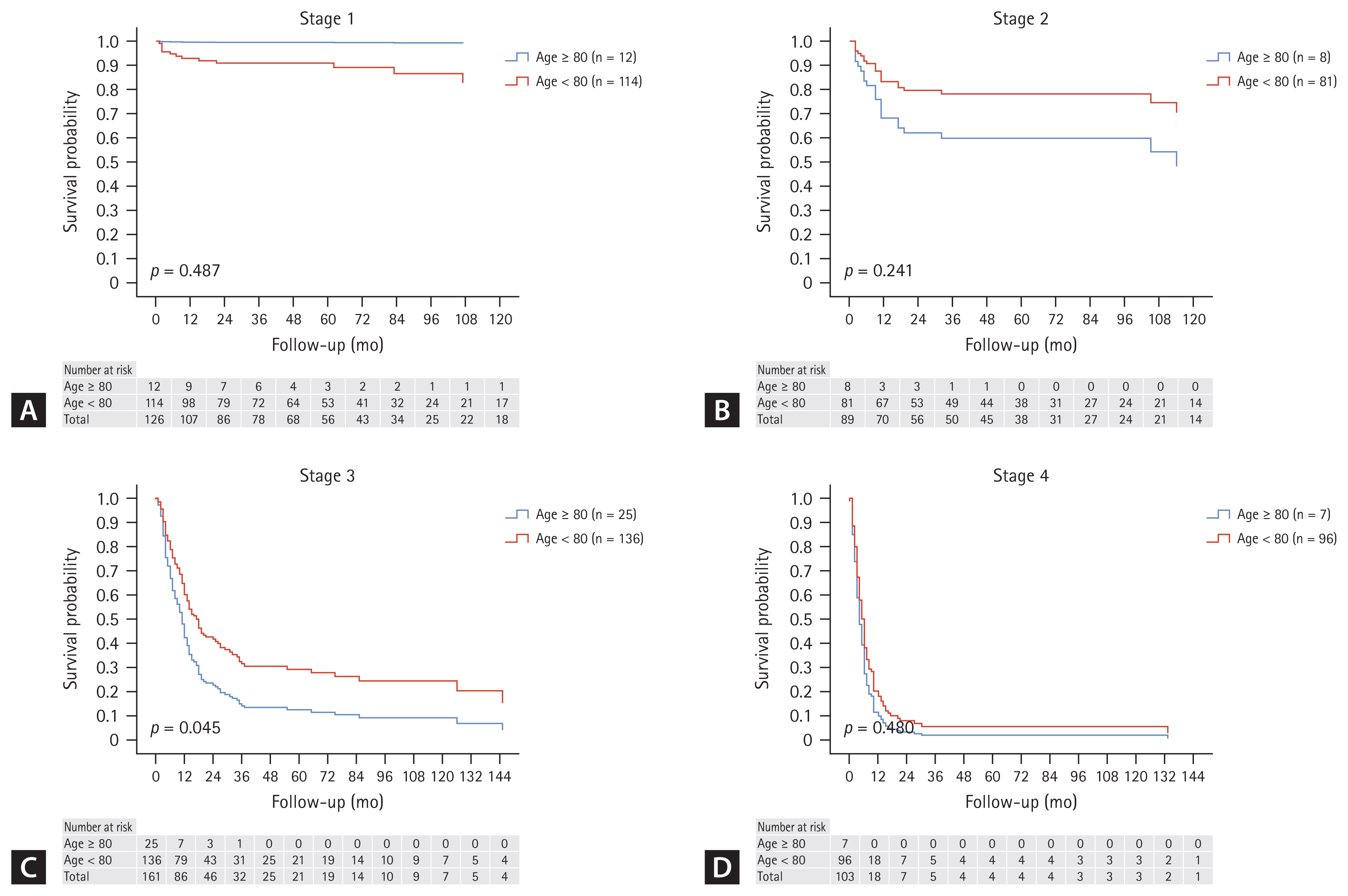
Comparison of overall survival curves between the two groups according to stages. (A) Stage 1. (B) Stage 2. (C) Stage 3. (D) Stage 4.
Outcomes and survivals of patients over 80 years old
Figure 3A depicts survival according to the treatment method among the patients. All treatments showed superior survival compared to no treatment. Survival after surgery and CRT, including RT alone, was similar in patients over 80 years old (HR 0.82, 95% CI 0.22–3.11; p = 0.774). Figure 3B shows survival rates with and without treatment, which significantly increased with treatment (HR 0.08, 95% CI 0.03–0.20; p < 0.001). The overall survival rates with treatment at 1, 3, and 5 years were 72.5%, 63.9%, and 63.9%, respectively. The overall survival rates without treatment at 1, 3, and 5 years were 5.9%, 0%, and 0%, respectively. There was no difference in comorbidities between the group that received treatment for cancer and the group that did not. However, the survival rate was significantly worse in the group that did not receive treatment for cancer, regardless of the Charlson comorbidity index (Table 5).
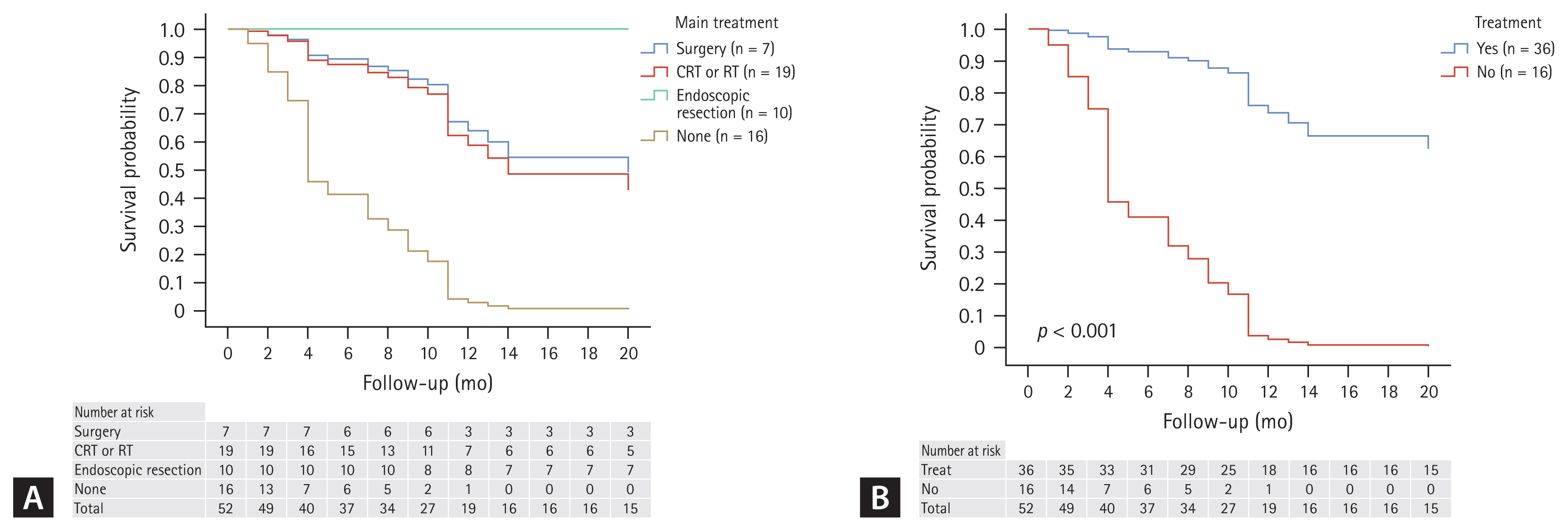
Overall survival curves for the elderly group. (A) Survival according to each treatment. (B) Survival compared to with and without treatment. CRT, concurrent chemoradiotherapy; RT, radiation therapy.
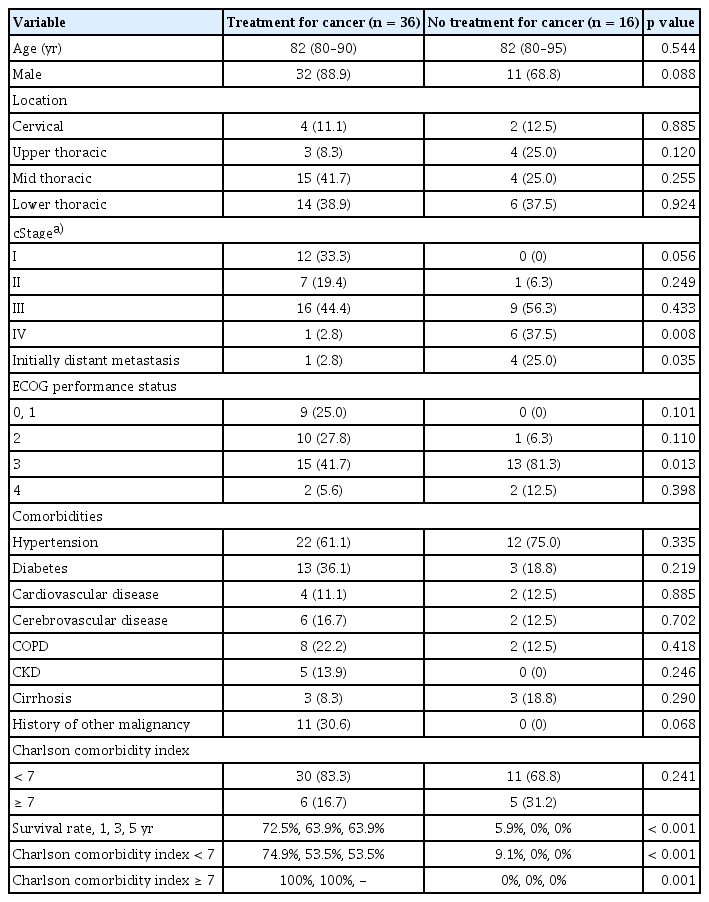
Comparison of groups with and without treatment in patients over 80 years of age
DISCUSSION
This study shows that it is better to actively treat patients all with ESCC, even those over 80 years old. Although the number of patients aged over 80 years was small, no differences were observed in outcomes and survival according to each treatment compared with younger patients. However, in actual clinical practice, as in our study, many patients over 80 years of age with esophageal cancer do not receive cancer treatment. Additionally, patients aged over 80 years had more comorbidities. However, no difference was seen in comorbidities when comparing patients who received treatment for cancer with those who did not in our study.
Cancer is the leading cause of death worldwide. The number of new cancer cases and associated deaths continues to rise [9]. As life expectancy increases, the number of patients diagnosed with cancer at an older age also increases. Although cancer treatments have advanced, treating elderly patients with cancer remains a challenge. Esophageal cancer is a representative cancer that occurs frequently in the elderly and its incidence is gradually increasing worldwide [4,10]. The peak incidence of esophageal cancer has moved to the 70s [3,11], and in a large-scale study in the Netherlands, 33% of patients diagnosed were over 75 years old, and 8% were over 85 years old [11]. As the number of elderly individuals with good general condition has increased, the number of elderly patients with esophageal cancer receiving active treatment has also increased [12].
Esophagectomy can be risky for elderly patients owing to its high morbidity and mortality rates [13,14]; however, CRT, another treatment option for esophageal cancer, may be relatively safer than surgery [15]. Among esophageal cancers, ESCC is particularly sensitive to radiation, and thus RT may be more effective [5]. When surgery is performed after neoadjuvant CRT for ESCC, the pathological complete response rate is > 40% [16,17]. Moreover, the guidelines recommend that in ESCC cases, observation instead of surgery is possible when no evidence of disease remains after neoadjuvant CRT [18]. In our study, 109 patients (19 in the elderly group and 90 in the younger group) were followed up with CRT or RT alone, and 55 patients (50.5%) (9 [47.4%] in the elderly group and 46 [51.1%] in the younger group) achieved cCR.
Some comparative studies have been conducted on esophageal cancer in the elderly population, including two meta-analyses on surgery [19,20]. One study defined the elderly as those over 70 years old [20], and another study defined them as those over 80 years old [19]. In both studies, elderly patients had significantly worse postoperative mortality and survival [19,20]. The postoperative mortality of patients aged ≥ 80 years was reported as 0–23% [19]. Although the number of surgical patients in our study was very small (n = 7), only one surgery-related death occurred (14.3 %). Postoperative survival was worse in the elderly group; however, no statistical significance was observed in our study (HR 1.37, 95% CI 0.43–4.33; p = 0.597).
There have been only three studies on CRT, including RT alone, for patients with esophageal cancer aged > 80 years old [21–23]. In one study, pulmonary toxicity was higher in elderly patients with esophageal cancer; however, no difference was observed in the survival rate [23]. One study used the Japanese Nationwide Cancer Database and found that CRT, early-stage cancer, and SCC were favorable factors for overall survival in esophageal cancer patients over 80 years old [21]. The most recent study showed that surgery had the best 3-year survival rate in patients with esophageal cancer over 80 years old; however, the survival rate was worse when CRT was performed in T4 patients owing to side effects [22]. In our study, patients over 80 years old had similar survival rates as younger patients after both surgery and CRT, and surgery and CRT did not differ in this regard even when compared among patients over 80 years old.
There are no studies on endoscopic resection in patients with esophageal cancer aged ≥ 80 years; however, there is one study in patients aged ≥ 70 years [24] and another in patients aged ≥ 75 years [25]. In the study comparing patients aged ≥ 70 years, no complications were observed in the elderly group, and the curative resection rate was 84%, which was not different from that in the younger group [24]. In the study comparing patients aged ≥ 75 years, no differences were observed in complications (8%), curative resection rates (77%), or hospital stay after the procedure (8 days) in the elderly group [25]. However, these two studies included only 23 and 13 elderly patients, respectively [24,25]. In our study, 10 patients with esophageal cancer aged ≥ 80 years underwent endoscopic resection, and no differences were observed in the results between the two groups.
This study had some limitations. This was a single-center retrospective study, and elderly patients with ESCC may be in a relatively poor condition; hence, biases in treatment selection were prominent. Second, the number of patients aged ≥ 80 years is inevitably small, and if divided by treatment, the number becomes even smaller. Third, it was difficult to determine whether the deaths of elderly patients were due to cancer or other causes.
In conclusions, many patients with ESCC over 80 years old did not receive treatment for their cancer; however, survival significantly improved when they received any treatment. Compared with younger patients, no differences were observed in outcome and survival between surgery and CRT, including radiotherapy alone, and endoscopic resection was safe in patients aged ≥ 80 years. Therefore, even if patients with ESCC are ≥ 80 years of age, active cancer treatment is recommended. A long-term observational study with a larger number of patients with ESCC is needed in the future.
KEY MESSAGE
1. Patients aged ≥ 80 years with ESCC more often do not receive active cancer treatment.
2. Even among patients aged ≥ 80 years with ESCC, receiving any treatment significantly improved their survival rate, and the clinical results of each treatment did not differ from those of younger patients.
Notes
CRedit authorship contributions
Dae Gon Ryu: conceptualization, methodology, resources, investigation, data curation, formal analysis, validation, writing - original draft, visualization; Cheol Woong Choi: methodology, validation, writing - review & editing, supervision; Su Jin Kim: resources, validation; Su Bum Park: validation; Jin Ook Jang: resources, validation; Bong Soo Son: methodology, validation
Conflicts of interest
The authors disclose no conflicts.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by Korea government (Ministry of Science and ICT; no. RS-2023-00242011).