Femoral veno-arterial extracorporeal membrane oxygenation with a novel biatrial cannula for venous drainage and left ventricular venting
Article information

A 42-year-old man, without any previous underlying disease, was transferred to our hospital due to acute myocarditis caused by Coxsackie virus infection. Despite 2 days of supportive care and intravenous inotropic administration, his left ventricular ejection fraction (LVEF; 57%→30%%→10%) and hemodynamic status worsened progressively. Cardiac arrest occurred while preparing for extracorporeal membrane oxygenation (ECMO). Left atrial veno-arterial (VA) ECMO (LA-VA-ECMO) was performed via the right femoral artery and vein for LV unloading. After trans-septal puncturing, a 23-Fr Bio-Medicus NextGen multistage cannula (Medtronic, Minneapolis, MN, USA) was inserted with its tip placed in the left atrium (LA); one set of ports was placed inside the LA for LV venting and the other in the inferior vena cava (IVC) for simultaneous left-sided venting and venous drainage (Fig. 1A). After ECMO insertion, the electrocardiogram showed asystole. However, the patient was alert, and awake ECMO was maintained. Intensive conservative management was conducted, including continuous renal replacement therapy. On the third day, his conduction system recovered. Six days after cannulation, the hemodynamic status improved, and ECMO support was discontinued. Thereafter, LVEF recovered to normal, and he was discharged with outpatient follow-up.
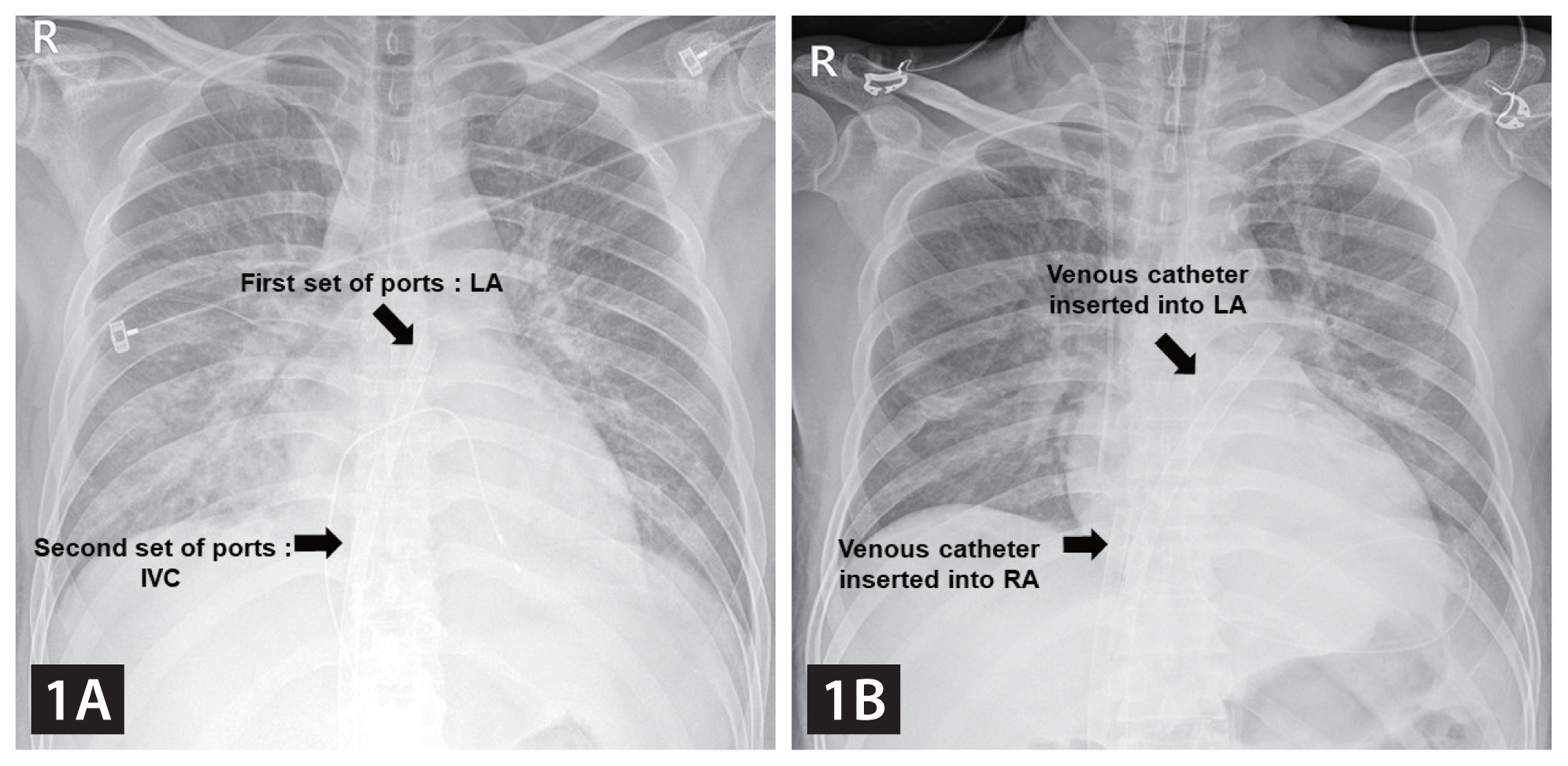
Comparing the use of a multistage cannula with conventional LA-VA-ECMO observed in chest X-ray. (A) Insertion of the Bio-Medicus NextGen multistage venous cannula across the atrial septum. One set of ports is placed in the LA through a trans-septal puncture and the other set in the IVC. (B) Conventional LA-VA-ECMO system. One venous cannula is located in the LA and another in the RA. LA, left atrium; VA, veno-arterial; ECMO, extracorporeal membrane oxygenation; IVC, inferior vena cava; RA, right atrium.
LV unloading is achieved by connecting the left atrial cannula to the inflow limb of a VA-ECMO circuit through a Y connector for biatrial drainage (Fig. 1B, 2B) [1]. The Bio-Medicus NextGen cannula was designed for minimally invasive cardiac surgery, utilizing an advanced multistage design to optimize drainage via the IVC, atrium, and superior vena cava. However, we have effectively used it for LA-VA-ECMO. One set of ports is placed in the LA through a trans-septal puncture and the other in the IVC, allowing effective venous drainage and simultaneous unloading of the LV venting using only one cannula. Moreover, it reduces the risk of vascular complications by eliminating additional vascular access (Fig. 2).

Differences in vascular access between a multistage cannula and conventional LA-VA-ECMO. (A) A multistage venous cannula. The ECMO circuit can be maintained the same as that for conventional VA-ECMO. (B) A conventional LA-VA-ECMO. A conventional LA-VA-ECMO is connected to the limb of the VA-ECMO circuit through a Y-connector. This requires vascular access of the bifemoral vein, increasing the risk of vascular complications. The complexity of the ECMO circuit also increases the risk of circuit-related issues. LA, left atrium; VA, veno-arterial; ECMO, extracorporeal membrane oxygenation.
Notes
CRedit authorship contributions
Jun Hwan Cho: conceptualization, writing - original draft, writing - review & editing, project administration; Woosik Han: conceptualization, writing - review & editing, project administration; Eun Jeong Cho: conceptualization, data curation; Sang-Yeub Lee: conceptualization, supervision; Sang-Wook Kim: conceptualization, supervision
Conflicts of interest
The authors disclose no conflicts.
Funding
None