Impact of COVID-19 on end-stage kidney disease incidence and clinical practice
Article information

The coronavirus disease 2019 (COVID-19) has affected nearly 8 billion people worldwide since the first reported case in Wuhan, China. People undergoing kidney replacement therapy (KRT) are vulnerable to many infectious diseases due to their decreased immunity and multiple comorbidities. Patients with end-stage kidney disease (ESKD) are at higher risk for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and complications compared to the general population due to comorbidities such as diabetes mellitus and cardiovascular disease, old age, and impaired immune function. However, it is unclear whether patients on hemodialysis (HD) have a higher incidence of COVID-19 than the general population. A study in the United States reported a SARS-CoV-2 seroprevalence of 9.3% among dialysis patients, compared to an estimated seropositivity rate of 9.2% in the United States general population during the same period [1]. In comparison, the mortality rate for dialysis patients (10–30%) is higher than that of the general population [2]. A study in South Korea found that in-hospital mortality was 22.4%, and the mortality rate for intenstive care unit admissions was even higher at 64.7% [3].
During the COVID-19 pandemic, the number of new ESKD cases differed by country. Figure 1 compares results from the United States Renal Data System (USRDS) [4], European Renal Association (ERA) registry [5], and Korean Renal Data System (KORDS) [6] from 2018 to 2022. In the United States and Europe, the number of incident cases trended upward until 2019, and declined sharply in 2020, when COVID-19 began. Since 2021, the ESKD incidence has recovered in the United States but continued to decline in Europe until 2021. By contrast, in South Korea, the number of new ESKD patients has remained similar since COVID-19, suggesting that the pandemic has not had an immediate or long-term effect on overall ESKD incidence. This may reflect the stability of the healthcare system in diagnosing and managing ESKD patients despite the challenges posed by the pandemic.
Interestingly, the prevalence of ESKD has continued to increase in South Korea after the COVID-19 pandemic, while its prevalence leveled off in the United States and continues to decline in Europe (Fig. 1). This may be related to the increase in deaths among dialysis patients. In the United States, the number of deaths per 1000 person-years among dialysis patients increased sharply from 131.7 in 2018 and 128.5 in 2019 to 151.8 in 2020 and 153.7 in 2021 [4]. In South Korea, unlike the United States and Europe, the prevalence of ESKD has continued to increase, which can be attributed to a well-operating medical treatment system, disaster preparedness among healthcare workers, and/or a rapid national response to COVID-19, which led to stable care and low mortality rates for Korean ESKD patients. The South Korea healthcare system has experience dealing with MERS, having developed disease preparedness among healthcare workers and guidelines for infection control in HD units.

Incidence and prevalence of end-stage kidney disease (ESKD) in different countries before vs. after the COVID-19 pandemic. (A) Incidence and (B) prevalence of ESKD in United States (US), European Union (EU), and South Korea.
In-center HD patients usually have to be moved to a dialysis center three times a week, making complete self-isolation impossible. In addition, the patient density in dialysis units is typically high, which increases the risk of infectious disease transmission. In comparison, peritoneal dialysis (PD) takes place at home, where patients are better isolated physically from the virus and are expected to be at lower risk of COVID-19 than in-center dialysis patients [7]. However, few studies have investigated whether the COVID-19 pandemic has affected dialysis incidence and modality selection.
Kim et al. [8] investigated changes in ESKD incidence, KRT modalities, and healthcare access in South Korea during the COVID-19 pandemic. Despite the pandemic, there was no significant increase in the overall incidence of ESKD and it remained stable. In addition, the distribution of KRT modalities continued the pre-COVID-19 treatment trend. In contrast, the COVID-19 pandemic has changed clinical practice patterns in the United States, where PD continues to grow as the KRT modality of choice for ESKD patients (Table 1). In addition, the Medicare dialysis prospective payment system was introduced in the United States in 2011 [9], and more ESKD patients are likely beginning and maintaining PD since its implementation.
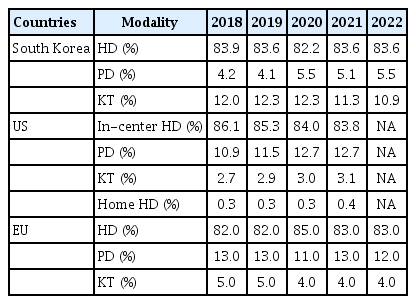
Changes in kidney replacement therapy selection for incident ESKD patients in different countries before vs. after the COVID-19 pandemic
Although patients who receive in-center HD are at higher risk of acquiring COVID-19, it is impossible to lockdown the HD unit because HD is essential for patient survival. Therefore, the continuation of uninterrupted dialysis services while adhering to infection-prevention guidelines is critical. HD units are required to follow clinical practice guidelines to prevent secondary COVID-19 transmission. These vary depending on the severity of the COVID-19 outbreak but include basic handwashing, wearing masks, not eating and drinking in the HD unit, and using antiviral medications in confirmed cases. If COVID-19 is confirmed, cohort isolation dialysis is implemented and if this is not feasible, patients are quickly transferred to a healthcare facility that can provide isolation treatment [10]. Finally, all ESKD patients should be vaccinated against COVID-19.
In conclusion, COVID-19 has had a significant impact on the incidence and prevalence of ESRD, with the extent of the effect varying by country. In South Korea, the national healthcare system remained relatively unchanged during the pandemic, and the impact of COVID-19 was minimal. For proper infection prevention and control, each dialysis unit should educate patients and healthcare staff, use personal protective equipment, maintain an optimal healthcare environment, detect infected patients early, and implement cohort isolation. In addition, improvement in the medical system to prepare for future renal disasters and infection is essential for the stable treatment of patients with ESKD.
Notes
Conflicts of interest
The authors disclose no conflicts.
Funding
None