Systemic venous air embolism after percutaneous lung biopsy
Article information
A 76-year-old man with suspected lung cancer underwent a computed tomography (CT)-guided percutaneous core needle biopsy (PCNB) (Fig. 1A). The immediate post-procedural CT scan showed intravenous air that originated from the intercostal vein and extended to the azygos vein (Fig. 1B). Moreover, free air was identified in the right atrium and coronary sinus (Fig. 1C). These findings were suggestive of systemic venous air embolism (AE) as a complication of PCNB. The patient was asymptomatic. He was observed with a 100% oxygen supply and adjusted to the left lateral decubitus position with his head down for 15 minutes in the CT room. He was then kept in this position with high-flow oxygen administration (100% FiO2, 30 L/min of O2) in the general ward. A low-dose chest CT taken 24 hours later showed complete absorption of the systemic venous AE. He was discharged without any sequelae. To our knowledge, this is the first report of systemic venous AE after a percutaneous needle biopsy of the lung.
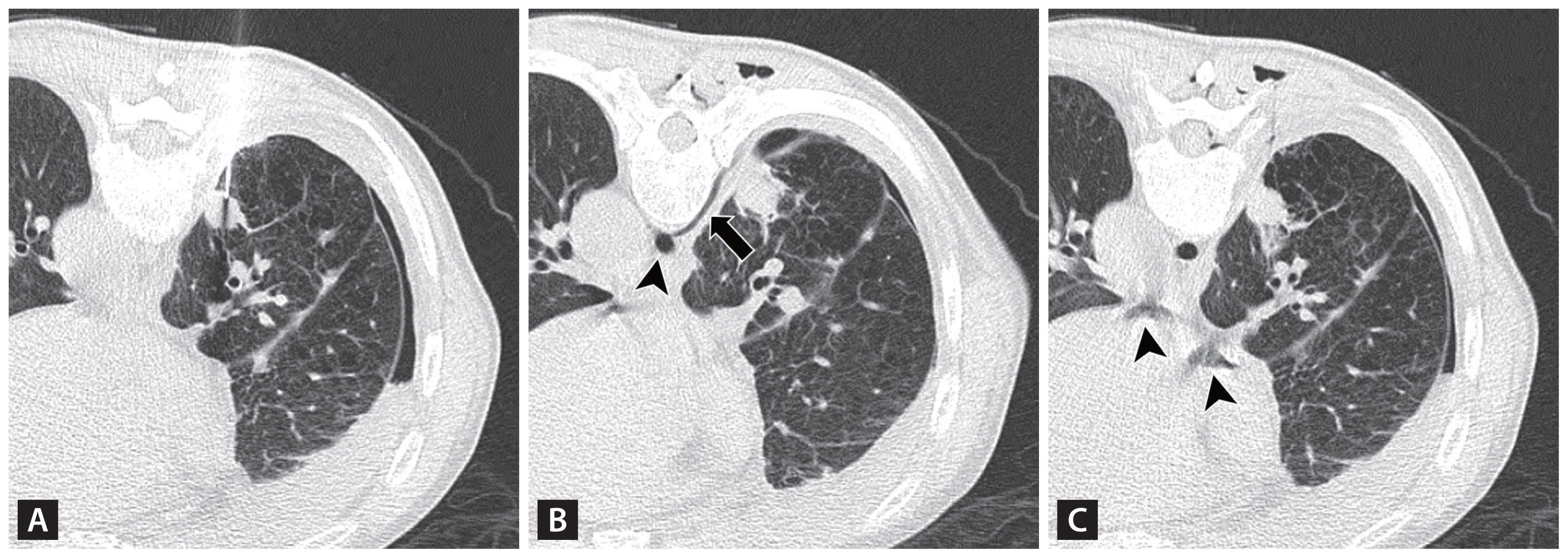
(A) Intra-procedural computed tomography (CT) scan for core biopsy of the lung nodule with the patient in the prone position using a 20-gauge core needle. (B) Post-procedural CT scan showing intravenous air arising from the intercostal vein (arrow) and extending to the azygos vein (arrowhead). (C) On post-procedural CT scan, free air with a flow-related motion artifact could be identified in the right atrium and coronary sinus (arrowheads). Air density was also detected in both the posterior external/internal vertebral venous plexus and right longissimus thoracis muscle.
AE is a rare complication of PCNB, but its consequences are potentially fatal. To our knowledge, only systemic arterial AE has been reported as a complication after percutaneous lung biopsy, as–to this point–there has been no case in which venous AE has been reported as such a complication. A patient with arterial embolization should be placed in the supine position to avoid exacerbating cerebral edema. By contrast, when venous embolization is suspected, a patient should be placed in the left lateral decubitus position to prevent right ventricular outflow obstruction by airlock [1]. The Trendelenburg position may also help relieve obstructions caused by air bubbles for venous AE [2]. Altogether, these results stress the importance of being aware that venous AE can occur after PCNB, as the optimal subsequent treatment will differ depending on whether it is arterial or venous.
Notes
CRedit authorship contributions
Min Kyung Jung: writing - original draft; Shin Young Kim: writing - review & editing; Jeong Min Ko: conceptualization, methodology, resources, writing - review & editing, supervision
Conflicts of interest
The authors disclose no conflicts.
Funding
None