Comparison of Acquired Cystic Kidney Disease between Hemodialysis and Continuous Ambulatory Peritoneal Dialysis
Article information
Abstract
Objectives
ACKD has been described mainly in patients treated with hemodialysis(HD), and there are only a few reports about the prevalence of ACKD in continuous ambulatory peritoneal dialysis (CAPD) patients. Therefore, we compared the prevalence of ACKD in patients receiving HD and CAPD, and evaluated the possible factors which may affect the development of ACKD.
Methods
Forty nine HD and 49 CAPD patients who had received dialysis therapy for at least 12 months were enrolled in this cross-sectional study. Patients who had a past history of polycystic kidney disease and had acquired cystic kidney disease on predialysis sonographic exam were excluded. Detection of ACKD was made by ultrasonography and ACKD was defined as 3 or more cysts in each kidney.
Results
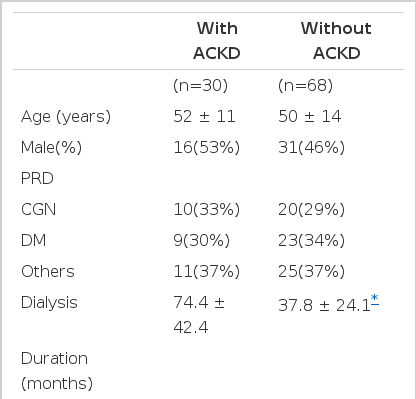
The prevalence of ACKD was about 31% (30/98) and there was no significant difference between HD and CAPD patients(27% vs. 34%, P> 0.05). The prevalence of ACKD was not associated with age, sex, primary renal disease, the levels of hemoglobin, BUN, and serum creatinine. However, the duration of dialysis was significantly related to the development of ACKD (presence of ACKD, 74.4±42.4 months vs. absence of ACKD, 37.8 ± 24.1 months, p < 0.05).
Conclusion
The prevalence of ACKD is not different according to the mode of dialysis, and the major determinant of acquired cyst formation is duration of dialysis.
INTRODUCTION
Acquired cystic kidney disease (ACKD) is characterized by the development of multiple cysts in the patients of chronic renal failure without a history of hereditary cystic renal disease. ACKD is for the most part clinically asymptomatic, but clinical concern about ACKD has increased because of its relation to renal cancer.
In 1977, Dunnil et al.1) first described ACKD in patients on maintenance hemodialysis (HD). Since then there have been a number of reports on the association of ACKD with HD2–8). However, there have been only a few reports about the prevalence of ACKD in patients receiving continuous ambulatory peritoneal dialysis (CAPD)9–11). We compared the prevalence of ACKD between HD and CAPD patients and evaluated the possible factors which might affect the development of ACKD.
MATERIALS AND METHODS
Of a total 375 patients with end-stage renal disease receiving HD or CAPD at the Kangnam and the Uijeongbu St. Mary’s Hospital, 98 patients (HD; 49, CAPD; 49) were enrolled in this study. We included patients who were treated with only one dialysis modality for more than 12 months and those without polycystic kidney disease or other cysts on predialysis ultrasonographic examination. One radiologist and one urologist, who were not aware of the patients’ information, performed renal ultrasonography and checked the presence, number and size of cysts and renal mass. To evaluate the possible factors that might affect the development of ACKD, we reviewed medical records and characterized the patients according to age, sex, duration of dialysis, erythropoietin use, and primary renal disease. During the study period, all patients had venous blood taken for the levels of BUN, creatinine, hemoglobin and hematocrit. For HD patients, blood sampling was done just before dialysis treatment. We defined ACKD as 3 or more cysts in each kidney2) and recorded the number of cysts from more affected kidneys. The results were expressed as mean standard deviation and analyzed with SPSS statistical program. Student’s t-test and Mann-Whitney U-test were used for continuous variables between 2 groups and chi-square test for categorical variables. P value less than 0.05 was considered significant.
RESULTS
1. PATIENTS’S CHARACTERISTICS
The mean age of our patients was 50 years (range, 15–79) and 47 patients were men. The mean dialysis duration of these patients was 49.3 months (range, 12–186 months). Primary renal disease consisted of diabetes mellitus (n=32), chronic glomerulonephritis (n=30), hypertension(n=12), unknown(n=10) and others(n=14). The clinical and laboratory findings of patients are shown in Table 1. There were no significant differences in age, sex, underlying renal disease, dialysis duration and the levels of hemoglobin and hematocrit between the two groups. The levels of BUN and serum creatinine in CAPD patients were significantly lower than in HD patients.

Comparison of clinical and laboratory characteristics between HD and CAPD patients.
2. PREVALENCE AND NUMBER OF CYSTS
The prevalence of ACKD was about 31% (30/98) and there was no significant difference between HD and CAPD patients (27% vs. 34%, p>0.05). The size of cysts was not different between the two groups, but the number of cysts in CAPD patients was higher than in HD patients (5.5 ± 2.7 vs. 3.5 ± 0.7, p < 0.05)(Table 2). The duration of dialysis in ACKD patients was not significantly different between the two groups (HD; 79.4 ± 36.4 vs. CAPD; 70.6 ± 40.1 months).

Comparison of prevalence and cyst characteristics of acquired cystic kidney disease between HD and CAPD patients.
3. CLINICAL AND LABORATORY PARAMETERS BETWEEN PATIENTS WITH AND WITHOUT ACKD
The presence or absence of ACKD is tabulated, based on the clinical and laboratory parameters (Table 3). The mean age, sex, underlying renal disease, erythropoietin use, and laboratory findings were not different between the two groups. However, duration of dialysis was significantly longer in the patients with ACKD than in those without ACKD. When the patients were divided into 2 groups according to the duration of dialysis, the prevalence of ACKD was 14% in the group of less than 3 years’ dialysis and 45% in the group of more than 3 years’ dialysis (P<0.05)(Table 4).
Comparison of clinical and biochemical parameters between patients with and without acquired cystic kidney disease
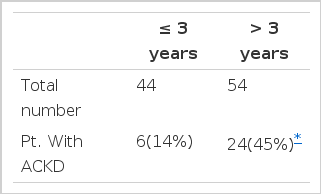
Prevalence of acquired cystic kidney disease according to the duration of dialysis
DISCUSSION
Our study demonstrates that prevalence of ACKD is not different between CAPD and HD patients. In general, CAPD is commonly supposed to be at less risk of developing ACKD than HD12,13). But recent studies have found the incidence is nearly equal between the two modes of dialysis10,11,14). Our study clearly shows that dialysis mode dose not affect the occurrence of ACKD.
ACKD is more commonly observed in patients on dialysis for longer periods14–16). Matson et al,14) have shown that, after 1 to 3 years of dialysis, the prevalence of ACKD is 10% to 20%, rising thereafter to reach 40% to 60% at 3 to 5 years of dialysis, and more than 90% after 5 to 10 years of dialysis. In our result, prevalence of ACKD was 14%(6 of 44 patients) in patients on dialysis for less than 3 years and 45%(24 of 55 patients) for more than 3 years. In addition, the mean dialysis duration of the patients with ACKD was significantly longer than that of the patients without ACKD (74.4 vs. 37.8 months). Our finding was consistent with previous reports14–18) that the major determinant of acquired cyst formation is duration of dialysis.
There has been a controversy over the relationship between erythrocytosis and ACKD. Some authors reported that there is a significant positive correlation between occurrence of ACKD and improvement of anemia, and this relation is associated with an increase of erythropoietin levels3,19) or cyst size4). On the other hand, others reported that there was no correlation between level of hemoglobin and presence of ACKD5,6,20). In our study, there were no significant differences in the level of hemoglobin, hematocrit and erythropoietin use between patients with and without ACKD. Even when we excluded patients who had received erythropoietin treatment, we could not find any relation between hemoglobin levels and ACKD. (Data were not shown)
Although the level of BUN was higher in HD patients than in CAPD patients, there was no difference between patients with ACKD and those without ACKD. This finding suggests that ACKD is not related to the degree of uremia.
In the majority of patients with ACKD, clinical features are asymptomatic and incidentally detected by ultrasound, CT scanning or at autopsy16,18). Apart from bleeding, the most significant complication of ACKD is the development of renal tumors. It is clear that the incidence of renal cancer is significantly increased in ACKD patients7,16,18). Truong et al.21), through a comprehensive review of the literature, represented that there is up to a 50-fold increased risk of renal cell carcinoma in ACKD compared to the general population. We already have experienced 2 cases of renal cell carcinoma associated with ACKD in our dialyzed patients. Both patients were men who had been treated exclusively with CAPD for more than 2 years. The presenting symptom of one patient was frank pain with perirenal hematoma, and the other was weight loss22). Therefore, it seems to be very important to detect ACKD before it develops into renal cell cancer, considering asymptomatic clinical features of ACKD.
It is generally agreed that there is a need for regular screening of symptomatic ACKD patients for early detection of renal cell carcinoma. However, whether screening is needed for asymptomatic patients remains controversial because of the lack of data about the effect of screening on the outcome of patients21,23). Nevertheless, many investigators recommend that patients should undergo annual screening after the third year of dialysis because the incidence of ACKD increases significantly after 3 years of dialysis5,16,17). Recently, Sarasin et al.24) reported that screening for ACKD offers dialyzed patients as much as a 1.6 year gain in life expectancy. They used strategies of performing either computed tomography or ultrasound every three years in all dialysis patients, and annually in patients who were found to have cysts.
Sonography or CT scanning is useful as initial screening tools. In general, CT scanning is preferable to sonography. The reasons are that the small kidneys of end stage renal disease and cysts less than 1cm are often difficult to image by sonography, and CT scanning is probably more sensitive than sonography for detecting solid tumor9,18,25). However, our preference is sonography as a screening procedure because of its easy availability and economic reason.
In summary, an ultrasound study in our patients with ESRD revealed a similar prevalence of ACKD, irrespective of the mode of dialysis, i.e., HD or CAPD. We also found that the duration of dialysis is significantly related to its development as shown by other studies. On the basis of our experience and previous literature, we recommend periodic screening of ACKD and renal tumor by ultrasonography in patients on dialysis.